|
|||
|
|
Fatality Assessment and Control Evaluation (FACE) Program |
|
ROPS Equipped Soil Compactor Overturn Kills Operator - Tennessee |
| |||||||||||
SummaryOn August 18, 2003, a 43-year-old female highway construction worker (the victim) died after the compactor she was operating rolled over the edge of a sloping dirt surface. The victim’s job was to help in the construction of a dirt ramp by compacting the ramp surface as dirt was added. The victim was operating the compactor with seat belt fastened. A dump truck used to deliver fill dirt and a dozer used to spread the dirt were also on the ramp. As the dump truck pulled up the slope to empty a load, the victim backed the compactor to the side of the ramp to allow the dump truck driver sufficient room to empty the load. As she was backing the compactor, the right rear wheel went over the edge of the ramp. After rolling 2 ¼ times, the compactor came to rest. The victim was partially thrown from the seat but remained in the seatbelt. Emergency rescue personnel were immediately called and arrived in minutes. The victim was airlifted to the local hospital where she was pronounced dead as a result of multiple injuries. NIOSH investigators concluded that, to help prevent similar occurrences, employers should:
Additionally,
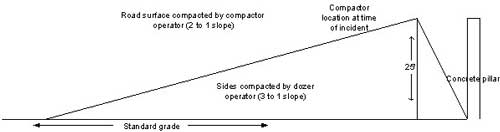
IntroductionA 43-year-old female equipment operator (the victim) died on August 18, 2003, when she was partially thrown from the compactor she was operating after it rolled over an embankment. On August 19, 2003, officials from the Tennessee Department of Labor and Workforce Development Division of Occupational Safety and Health (TOSHA) notified the National Institute for Occupational Safety and Health (NIOSH) Division of Safety Research (DSR) of the incident. On November 24, a safety professional from DSR met with the TOSHA compliance officer to discuss the case, review photographs and drawings of the incident collected during the compliance investigation, and visit the work site. The company president, the dozer operator and the primary contractor’s safety officer were interviewed. The equipment dealer who sold the equipment was interviewed via telephone. A subsequent trip was made to the equipment manufacturer by the DSR safety professional and two DSR engineers, and a Rollover Protective Structure (ROPS) manufacturer was consulted on the case. Copies of the operator’s manual and relevant standards were reviewed. Photographs of the equipment were taken. The employer, an earth-moving construction company which had been in the highway construction business about 5 months, was hired by the prime contractor to build a 4-lane packed dirt highway ramp that would be used to support the approach to a bridge over a railroad track. The prime contractor was hired by the State Department of Transportation to construct a roadway. The company (sub-contractor) where the victim worked was formed specifically for this project and this was the first major project the company had secured. At the time of the incident, the employer had 20 workers, all working at the site. The typical work shift was from 7:00 a.m. till 5:30 p.m., 6 to 7 days per week. Safety meetings were held two times per week by the prime contractor and attendance by the sub-contracting company employees was mandatory. The employer does not have a designated safety person but relies on the prime contractor for hazard identification and safety training. The employer did not have its own formal safety training program. Prior to employment with the construction company, the victim had never operated a compactor or other earth moving equipment. Previously, the victim worked in the furniture manufacturing industry. This was the company’s first workplace fatality. The victim had worked for the company 4 months and was hired specifically to operate the compactor. The company owner spent a few hours with the victim at the time of hire to provide instructions on maintaining the compactor fluid levels and using the operating controls. He rode along with the victim explaining the process and showing her the controls. Her responsibilities at the site were to compact the soil on the ramp. She had been working on the ramp at this site 6 days along with a dozer operator, a dump truck driver and a tractor operator. Back to TopInvestigationConstruction of the built-up ramp involved a four step process. First, a load of soil is dumped where the slope was to be created. Second, the dozer operator pushes the dirt to a gently sloping grade. Third, the tractor operator pulls a disc behind the tractor, breaks up large clumps of dirt, and levels the surface. Lastly, the compactor is driven over the smoothed surface. The process is repeated until the sloping dirt mound reaches 25 feet above standard grade and a width of approximately 85 feet. A profile of the ramp is shown in Figure 1. The compactor, a self-propelled articulated-frame design with an operating weight of 23,000 pounds was equipped with a ROPS and seatbelt and powered by a 125-horse power diesel engine. (Figure 2 and Photo 2) Its total height is ten feet, width seven feet nine inches, and length nineteen and a half feet. The variable vibrating drum is five feet five inches in diameter, and seven feet wide mounted on the front of the machine. Inside the drum a variable speed eccentric shaft rotates to create additional force on the ground up to 50,500 pounds. A single lever controls the compactor’s direction, speed and braking from a forward facing (toward the drum) bucket seat. The unit operates in two speed ranges, low for compacting and high for transporting. Maximum speed in low range is 4 miles per hour in both forward and reverse. At the time of the incident a dump truck used to deliver fill dirt and a dozer used to spread the dirt were also on the ramp. As the dump truck pulled up the slope to empty a load, the victim backed the compactor to the side of the ramp to allow the dump truck driver sufficient room to empty the load. The five-foot-four inch tall 175 pound victim was wearing a hard hat and was wearing the seatbelt on the compactor. According to a witness, the victim was looking over her left shoulder as she was backing the compactor. As the right rear tire went over the edge she called for help and appeared to be ‘trying to get up and out of the cab,’ but remained restrained by the seatbelt. It is not known if the seatbelt was loose or tight at the time. Tracks made by the compactor indicated the unit backed approximately 30 feet up the sloping surface prior to backing off the edge, rolled two and a quarter times and came to rest on its side. Emergency Medical Services (EMS) were called by the tractor driver from the site phone and responded minutes later. According to witnesses, the victim’s head was under the vertical support of the ROPS but was not trapped, nor was the ROPS resting on her head. She was slid out from under the ROPS after cutting the seatbelt and air lifted to the local hospital where she was pronounced dead. At the time of the investigation, the seat belt had been replaced by a local equipment dealer but the ROPS had not been replaced. The original seatbelt was not available for examination. Back to TopCause of DeathThe medical examiner investigation report noted head and neck injuries and multiple fractures of the skull and facial bones, leading to death. Back to TopRecommendations/DiscussionRecommendation #1: Employers should thoroughly train compactor operators before they operate machines, including training on the hazards of operating on slopes.Discussion: Employers should train heavy equipment operators in the proper use of the equipment and ensure equipment manufacturers’ recommended safety procedures are used in the training. Increasing responsibilities should be given to an employee only after they have been properly trained. Documentation of this training should be maintained. In this case, the operator had about 13 weeks of driving experience on a flat surface before going on a slope which requires additional skill in maneuvering the unit. Employers who acquire new equipment should seek training from either the dealer or manufacturer who is qualified to demonstrate and lead a safety course for the employees, particularly the designated operator(s). This training should include the proper use of seatbelts while on the equipment and what the operator should do in the event of a turnover. Training by the employer should be based on the recommendations in the operator’s manual which in this case states: “Always be sure that persons entrusted with work on the machine have read the operating instructions and in particular the chapter on safety before beginning work. Reading the instructions after work has begun is too late.” Further, the safety precautions and guidelines in the manual state to “Always keep at a distance from the edges of building pits,” and “Do not work in the vicinity of overhanging banks or on grades that could cause the compactor to slide or roll”. According to the employer, the employee had not read the operator’s manual prior to operating the machine. The employer should permit only those properly trained to operate the equipment (29CFR1926.20(b)(4)).1 The worker’s ability to perform the job should be assessed before assigning work.
| ||||||||||||
 |
 |
 |
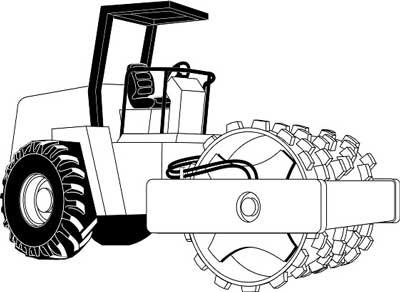 |
Figure
2. Compactor (permission to use this drawing was given by manufacturer). |
