Agency for Toxic Substances and Disease Registry
|
||||||||||||||||||||||
| Organ/System | Exposure Risks | |
|---|---|---|
| Respiratory | Asbestos, radon, cigarette smoke, glues | |
| Dermatologic | Dioxin, nickel, arsenic, mercury, cement (chromium), polychlorinated biphenyls (PCBs), glues, rubber cement | |
| Liver | Carbon tetrachloride, methylene chloride, vinyl chloride | |
| Kidney | Cadmium, lead, mercury, chlorinated hydrocarbon solvents | |
| Cardiovascular | Carbon monoxide, noise, tobacco smoke, physical stress, carbon disulfide, nitrates, methylene chloride | |
| Reproductive | Methylmercury, carbon monoxide, lead, ethylene oxide | |
| Hematologic | Arsenic, benzene, nitrates, radiation | |
| Neuropsychologic | Tetrachloroethylene, mercury, arsenic, toluene, lead, methanol, noise, vinyl chloride | |
| These substances are examples of toxicants that might affect organ systems; this is not an all-inclusive list. Bold type indicates that the substance is covered in one of the Case Studies in Environmental Medicine. |
||
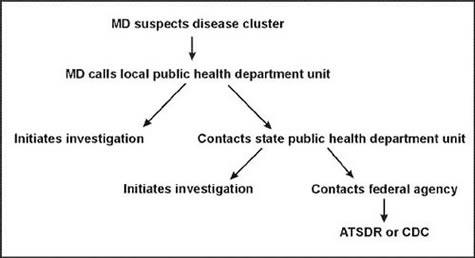
An initial goal of the public health unit's evaluation should be to decide whether the cluster is "unusual" (i.e., whether an unexpectedly increased incidence of disease really exists) and, if so, whether some plausible biologic hypothesis can explain that unexpected disease rate. The public health department can perform the following cluster evaluation components (Figure 2):
- Establish a case definition.
- Confirm the suspected cases.
- Define a "population denominator" measured in person-years and search for additional numerator cases within that population. Draw conclusions about the "unusualness" of the cases.
- Review the literature for risk factors and exposure hypotheses.
- Perform an exposure assessment.
- Generate biologically plausible hypotheses.
- Person-years are the most frequently used measure of person-time. Person-time is the sum of individual units of time that persons in the study population have been exposed to the condition of interest. This measurement is used as a denominator in person-time incidence and mortality rates.
- With this approach, each subject contributes only as many years of observation to the population at risk as he or she is actually observed; if the subject leaves after 2 years, he or she contributes 2 person-years. This method can be used to measure incidence over extended and variable time periods.
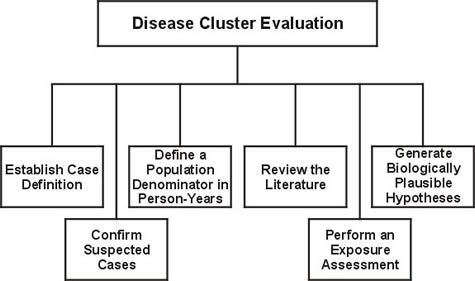
Figure 2. Components of a Disease Cluster Evaluation
|
| Agency for Toxic Substances and Disease Registry 4770 Buford Hwy NE, Atlanta, GA 30341 Tel: CDC Contact Center: 800-CDC-INFO • 888-232-6348 (TTY) |
Department of Health and Human Services |