|
Putting Polytrauma Care 'on the Map'
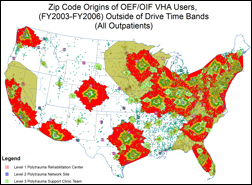
In a study to be presented at a national VA meeting in December,
investigators at VA's Rehabilitation Outcomes Research Center
(RORC) in Gainesville, Fla., used specialized geographic software
to track access to VA care for traumatically wounded veterans of
the Afghanistan and Iraq wars. The findings will help VA planners
decide where to locate services for current and future cohorts of
veterans.
The research, led by Diane Cowper Ripley, PhD, plotted the
home ZIP codes, counties and regions of nearly 8,000 seriously
wounded veterans—anonymous, for purposes of the study—who
needed rehabilitation care during 2003 or 2004. That information
was compared against the locations of VA facilities that deliver
polytrauma care.
Among the findings: About 88 percent of the veterans in the
database had "reasonable" access to VA’s multi-tiered system of
polytrauma care. The median driving distances to the top three
levels of facilities—from comprehensive "Level 1" facilities to
supportive "Level 3" sites—were 411, 121 and 64 miles,
respectively.
Other findings:
- Hearing impairment was the most common traumatic injury,
affecting some 63 percent of the veterans, followed by vision loss,
orthopedic injuries, traumatic brain injury (4.2 percent), burns,
spinal cord injury, and amputation (1.3 percent). Just over five
percent of the veterans had polytrauma wounds—multiple,
complex injuries requiring intensive therapy.
- Four counties in Alabama and one county in each of six states
were identified as areas with potential gaps in access to
rehabilitation care. The states were Nevada, North Dakota, Texas,Hawaii, Alaska, and Mississippi. Clark County, Nevada—the area
around Las Vegas—and El Paso County, Texas, had the highest
numbers of patients outside of what were considered reasonable
drive time bands.
- For each mile a veteran was closer to a Level 2 polytrauma
site, the odds of receiving rehabilitation services increased one
percent.
The study yielded numerous other analyses relating to the
places veterans live and the nearest VA rehabilitation services.
Partly as a result of the data, VA is now moving to upgrade the
polytrauma care available in San Juan, where, according to Cowper
Ripley, a relatively large portion of the population serves in the
military and a high percentage of veterans enroll in VA care.
The software used by the Gainesville group is known generally
as Geographic Information Systems, or GIS. It’s used widely by
planners in many fields—by retailers, for example, to know where
to build new stores, and by police departments to track crime
patterns. If you’ve ever used Web-based consumer programs like
Mapquest or Google Maps, you have a rough initial sense of what
GIS can do. Just imagine adding in lots of powerful analytical and
statistical features and a huge palette of mapping and graphics
tools.
Four levels of polytrauma care
- Level 1—These are VA’s four main polytrauma centers,
located in Tampa, Richmond, Minneapolis and Palo Alto. A
fifth is planned for San Antonio. These sites provide
comprehensive acute care and rehabilitation for veterans with
the most severe wounds, many of whom arrive straight from
military hospitals such as Walter Reed Army Medical Center.
- Level 2—These sites service veterans who need somewhat
less intensive care. Care teams at these sites coordinate longterm
rehabilitation services as needed. Each of VA’s 21
nationwide Veterans Integrated Service Networks, or VISNs,
has at least one Level 1 or Level 2 facility.
- Level 3—These facilities have teams with rehabilitation
expertise that deliver follow-up services in consultation with
regional and network specialists. By way of example, VISN 11,
which spans 90,000 square miles in four Midwest states, has
three Level 3 sites.
- Level 4—These sites have at least one person who handles
consultation, assessment and referral of polytrauma patients to
higher-level facilities.
Policymakers at VA headquarters who use the software rely on
studies at the RORC and other research sites to support their
efforts. "GIS is a nice way to communicate across disciplines and
for researchers to communicate with policy people," says Cowper
Ripley. "When you show the picture and point out what you’ve
done, people can see what you're talking about. It's a lot better
than presenting a statistical model."
The RORC researcher is quick to acknowledge that GIS-based
research is only one of many factors that policymakers need to
consider. But it makes their job infinitely easier, she says.
"This is a tool for policymakers so they can meet the needs of
the largest numbers of patients. It helps them narrow down the
possibilities and focus on key geographic areas." For instance, the
software allows users to quickly play out different scenarios—
adding a Level 2 or 3 facility in a particular location, for example,
and seeing, in theory, how many additional veterans would be
served.
Says Cowper Ripley, "I think GIS is really helpful to management
for making that first cut, and that’s what its real utility is."
Other Resources
VA Polytrauma System of Care
|



