Venous Blood Lead Level (BLL) testing is the most useful screening and diagnostic test for recent or ongoing lead exposure as opposed to past exposures.
Different tests have been used in the past to evaluate lead exposure and/or to gauge the effects of lead exposure.
Venous BLL testing is the most useful screening and diagnostic test for recent or ongoing lead exposure as opposed to past exposures.
Given the greater risk of contamination using the finger-stick method, an elevated BLL obtained through finger-sticking should always be confirmed through venipuncture. (AAP 1993 and CDC, 1997a)
BLLs respond relatively rapidly to abrupt or intermittent changes in lead intake (for example, ingestion of lead paint chips by children) and, for relatively short exposure periods, bear a linear relationship to those intake levels.
For individuals with high or chronic past exposure, however, BLLs often under-represent the total body burden because most lead is stored in the bone and may have “normal” levels in the blood.
One exception is patients with a high body burden under physiological stressful circumstances whose BLLs may be elevated from the release of lead stored in bones.
Erythrocyte protoporphyrin (EP), commonly assayed as zinc protoporphyrin (ZPP), was previously considered the best test for screening for asymptomatic children, however, is not sufficiently sensitive at lower BLLs and therefore is not as useful a screening test for lead exposure as previously thought.
Over the past 30 years, there has been a dramatic decline, nationwide, in blood lead levels (BLLs). Findings from the most recent National Health and Nutrition Examination Survey (NHANES), 1999 – 2002, indicate that BLLs are continuing to decrease across all age and racial/ethnic groups in the U.S. Although BLLs remained higher for young non-Hispanic black children, this group also experienced the greatest decline (72%) in elevated BLLs since1991-1994. (CDC 2005)
The overall prevalence of elevated BLLs (≥ 10 µg/dL) for the U.S. population was 0.7%. (CDC 2005)
The average BLL for children 1-5 years of age was 1.9 µg/dL in 2002, down from 15.0 µg/dL in 1976-1980 (before leaded gasoline was banned; CDC 2005).
The average BLL for adults 18-74 years of age was 14.2 µg/dL from 1976-70; in 1988-1991, the average BLL for adults was 3.0 µg/dL (CDC 1997b).
An attempt should be made to identify and minimize lead exposures when BLLs indicate that they are occurring at any blood lead level above background population levels.
If an adult has a BLL of 20 µg/dL, e.g., an unusual exposure is likely occurring and should be interrupted, if possible. This is especially important for fertile and pregnant females.
Recent data indicate that the EP/ZPP assay at lower BLLs is not sufficiently sensitivity, and therefore is not as useful a screening test for lead exposure as previously thought. EP/ZPP assays continue to be used at times as a complement to venous BLL testing and are required by OSHA for some workplace testing.
Normal values of ZPP are usually below 35 µg/dL.
EP is also elevated in
iron deficiency anemia
jaundice
sickle cell
other hemolytic anemias
In erythropoietic protoporphyria, an extremely rare disease, EP is markedly elevated (usually above 300 µg/dL).
There are different evaluation methods used to study patients with elevated BLL.
Complete blood count (CBC) may be useful for patients with extensive exposure. In lead-exposed patients, the hemocrit and hemoglobin values may be slightly to moderately low in the CBC, and the peripheral smear may be either normochromic and normocytic or hypochromic and microcytic.
There may be basophilic stippling in patients who have been significantly poisoned for a prolonged period.
However, because these results are not specific to lead exposure, the CBC test is not as valuable for detecting lead exposure as the BLL and EP assays.
A hypochromic, microcytic anemia should be appropriately differentiated from other causes, especially iron-deficiency anemia by the use of testing for iron, iron binding capacity, and ferritin.
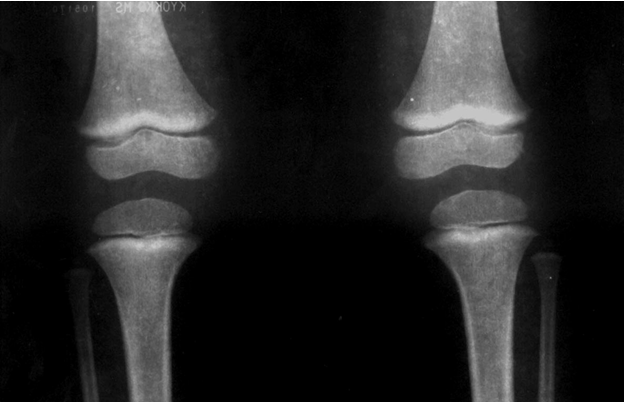
Abdominal radiographs may show the presence of radiodense lead foreign bodies in the gastrointestinal tract. These are helpful only in cases of acute ingestion (e.g. of lead sinkers, curtain weights, jewelry, or paint chips) or unusual persistence of high blood lead values. Longbone radiographs can show “lead lines”. These are lines of increased density on the metaphysis growth plate of the bone, showing radiological growth retardation. This is not a routine procedure to identify lead poisoning, but a radiological finding of chronic exposure. See Figure 2 and Figure 3.
Because hair and fingernails are subject to external environmental contamination, assaying their lead content is an uncertain estimate of body burden and is not recommended (AAP 1993; CDC 2002).
Longbone radiographs are not recommended for diagnosing lead exposure (CDC 2002), however, they are useful to determine reduced growth retardation.
Second tier tests (such as neurobehavioral/psychological evaluation for children with indicative findings on exam) should be considered, as appropriate.
Evaluation may also appropriately include tests for the health effects of lead.
Figure 2. Longbone Radiographs of Hands - “lead lines” in five-year-old male with radiological growth retardation and blood lead level of 37.7µg/dL. Photo courtesy of Dr. Celsa López, Clinical Epidemiologic Research Unit, IMSS, Torreón, México)
Figure 3. Longbone Radiographs of knees - “lead lines” in three-year-two-month-old girl with blood lead level of 10.6 µg/dL. Notice the increased density on the metaphysis growth plate of the knee. (Photo courtesy of Dr. Celsa López, Clinical Epidemiologic Research Unit, IMSS, Torreón, México)