Publications and Information Products
Information Sheet
November 2008
NCHS Data on Eating Behaviors
PDF version 126 KB
Page Content
About NCHS
Eating Behavior Data
NHANES Data
NHANES Weight History Data - Participants 16 Years of
Age and Older
Youth 8-15 Years of Age
Health Care Use
Hospital Discharges
Ambulatory Care Visits
Mortality Data
Deaths Due to Eating Disorders
Data Sources
About NCHS
The CDC's National Center for Health Statistics (NCHS) is the nation's principal health statistics agency, providing data to identify and address health issues. NCHS compiles statistical information to help guide public health and health policy decisions.
Collaborating with other public and private health partners, NCHS employs a variety of data collection mechanisms to obtain accurate information from multiple sources. This process provides a broad perspective to help us understand the population's health, influences on health, and health outcomes.
Eating Behavior Data
The public health community monitors eating behaviors which include eating disorders. Eating disorders are of particular concern because of their potentially serious health consequences. Obtaining reliable data on eating disorders, however, can be difficult because of the secretive nature of the behavior. Also, while NCHS surveys capture information on a wide range of health conditions and on health care use, not all health care providers are included and some of the surveys are conducted on small samples, making it difficult to detect and monitor conditions such as eating disorders that occur relatively infrequently.
NCHS obtains data on weight history and eating behaviors, health care use associated with eating disorders, and mortality due to eating disorders. Estimates of the prevalence of eating disorders are not obtained.
NHANES Data
Data from the National Health and Nutrition Examination Survey (NHANES) contribute to our understanding of eating behaviors. NHANES includes interviews, standardized physical examinations conducted in mobile examination centers, and laboratory tests.
- Data are obtained on the weight history of participants ages 16 years and older.
- Since 2005, NHANES has included weight-related questions targeted to youth 8-15 years of age.
- The height and weight of participants are measured, and underweight and normal weight status is determined based on body mass index calculated as weight in kilograms/height in meters squared.
NHANES Weight History Data - Participants 16 Years of Age and Older
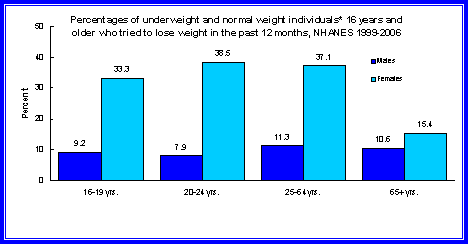
NHANES participants who are 16 years and older are asked questions about their weight history, whether they tried to lose weight in the past year, and methods used to lose weight in this time period. Measured height and weight are used to determine current weight status.
In 1999-2006, underweight and normal weight females were more likely than underweight and normal weight males to indicate that they tried to lose weight in the past 12 months (36.8 percent of underweight and normal weight females ages 16-64 years indicated that they tried to lose weight in the previous year as opposed to 10.4 percent of underweight and normal weight males ages 16-64 years).
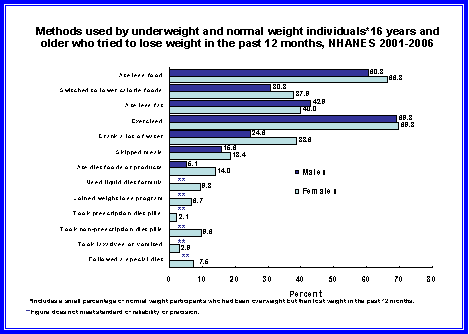
Data from 2001-2006 show that of those underweight and normal weight individuals who tried to lose weight, most used appropriate methods such as eating less food or exercising. Fewer than 3 percent of females reported taking laxatives or vomiting to lose weight.
Youth 8-15 Years of Age
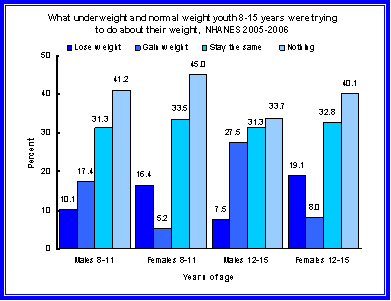
In 2005-2006, NHANES participants 8-15 years of age were asked if they were trying to lose weight and methods they used to do so. Measured height and weight are used to determine current weight status.
- In 2005-2006, underweight and normal weight females 8-15 years of age were more likely than underweight and normal weight males of the same age to report that they were trying to lose weight (16.4 percent of females ages 8-11 and 19.1 percent of females ages 12-15 as opposed to 10.1 percent of males ages 8-11 and 7.5 percent of males ages 12-15).
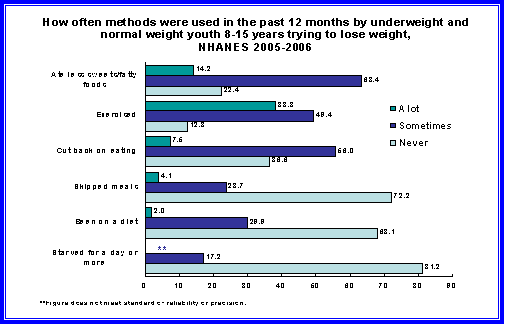
Data from 2005-2006 show that underweight and normal weight youth who were trying to lose weight were more likely to eat less sweets or fatty foods (77.6 percent reported that they did this a lot or sometimes) or exercise (87.7 percent reported that they did this a lot or sometimes) than the less commonly reported methods of skipping meals or starving for a day or more.
Health Care Use
Health care data are obtained from national surveys of providers and include information on patients, diagnoses, and treatments in selected medical care settings. Information on inpatient care is obtained from the National Hospital Discharge Survey - an annual survey of short-stay non-federal hospitals. The National Ambulatory Medical Care Survey, which surveys visits to offices of non-federally employed physicians providing office-based patient care, and the National Hospital Ambulatory Medical Care Survey, which surveys visits to hospital outpatient and emergency departments of non-federal short-stay hospitals, obtain information on ambulatory care.
Health care for persons with eating disorders is also provided in a variety of other settings, including specialty care centers and residential treatment centers. NCHS does not obtain data on care delivered in these settings and does not have information about the patients who seek care or the volume or type of care delivered in these settings.
Diagnoses associated with hospital discharges and ambulatory care visits for eating disorders include: anorexia nervosa, unspecified eating disorders, bulimia nervosa, pica, rumination disorder, vomiting associated with other psychological disturbances, and other eating disorders.
Hospital Discharges
- For 2004-2006, there were 5,000 average annual hospital discharges with an eating disorder diagnosis as the principal diagnosis or the first-listed diagnosis.
- For 2004-2006, there were 27,000 average annual hospital discharges with an eating disorder diagnosis listed among any of the first seven diagnoses (only seven diagnoses are coded).
Age |
First-listed diagnosis |
Any-listed diagnosis |
|---|---|---|
All ages |
5,000 |
27,000 |
Under 25 years old |
3,000 |
12,000 |
25-64 years old |
1,000 |
15,000 |
65 years and older |
* |
* |
NOTE: There were, on average, a total of 34.8 million annual hospital discharges for the period from 2004-2006.
*Figure does not meet standard of reliability or precision.
Source: National Hospital Discharge Survey
Ambulatory Care Visits
- For 2003-2006, there were, on average, 221,300 annual ambulatory care visits to physician offices and hospital outpatient and emergency departments with an eating disorder as the principal or first-listed diagnosis.
- For 2003-2006, there were, on average, 390,400 annual ambulatory care visits with an eating disorder listed in any of the first three diagnostic fields (only three diagnoses are coded).
| Age | First-listed (principal) diagnosis | Any-listed diagnosis |
|---|---|---|
All ages |
221,300 |
390,400 |
Under 25 years old |
143,700 |
229,100 |
25-64 years old |
66,400 |
139,100 |
65 years and older |
* |
* |
*Figure does not meet standard of reliability or precision.
NOTE: There were, on average, more than 1.1 billion annual ambulatory visits for the period from 2003-2006.
Source: National Ambulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey.
Mortality Data
For national mortality statistics, every death is attributed to one underlying cause based on information reported on the death certificate. Training materials are provided to support accuracy in reporting cause of death. Proper cause of death certification involves the reporting of a sequence of conditions leading to the underlying cause of death along with any conditions that contributed to death.
If the decedent is known to have died from an eating disorder, it is likely that the death certificate would reflect this in some way. There will be situations, however, where it is not known that a decedent had an eating disorder or where it is uncertain whether the eating disorder was a cause of death. If the eating disorder is not known, it would not be reported on the death certificate. In cases where it is not clear whether a decedent's eating disorder was a cause of death, the eating disorder may or may not be reported on the death certificate. The person certifying the cause of death (physician, medical examiner or coroner) would make a judgment as to the cause of death based on the evidence at hand. There is some indication that other conditions (for example, cardiac arrest) have been reported as the cause of death in cases of eating disorders, leading to an under-ascertainment of deaths caused by eating disorders.
Diseases are coded based on the International Classification of Diseases (ICD), a system that promotes international comparability in the classification of mortality statistics.
Deaths Due to Eating Disorders
Specific causes included in ICD-10 for classifying eating disorder deaths are: anorexia nervosa, bulimia nervosa, overeating associated with other psychological disturbances, vomiting associated with other psychological disturbances, and unspecified eating disorders.
In 2005, there were 56 deaths with an eating disorder reported as the underlying (primary) cause of death.
In the case of a death due to an eating disorder, it is not unusual to see a condition other than an eating disorder reported as the underlying cause with the eating disorder reported as a contributing cause. In 2005 there were an additional 78 deaths in which an eating disorder was a contributing cause of death.
As noted above, the death certificate may not capture all deaths associated with eating disorders. (This is the case with all causes but might be more pronounced in this cause).
| Year | Total | Less than 25 years | 25-64 years | 65 years and over |
|---|---|---|---|---|
2002 |
82 |
9 |
57 |
16 |
2003 |
83 |
12 |
54 |
17 |
2004 |
87 |
14 |
61 |
12 |
2005 |
56 |
5 |
40 |
11 |
Source: National Vital Statistics System.
Year |
Total |
Less than 25 years |
25-64 years |
65 years and over |
|---|---|---|---|---|
2002 |
159 |
15 |
106 |
38 |
2003 |
147 |
20 |
86 |
41 |
2004 |
161 |
22 |
106 |
33 |
2005 |
134 |
10 |
83 |
41 |
Source: National Vital Statistics System.
Data Sources
NCHS employs a variety of data collection mechanisms to obtain accurate information from multiple sources: They include:
- National Health and Nutrition Examination Survey (NHANES) - collects information about the health and diet of people in the U.S. NHANES is unique in that it combines a home interview with physical examinations and laboratory tests conducted in a Mobile Examination Center. NHANES can directly measure conditions and provide reliable information on health conditions regardless of whether the survey respondent is aware of them. (http://www.cdc.gov/nchs/nhanes.htm)
- National Health Care Surveys - a family of provider surveys, obtaining information about the facilities that supply health care, the services rendered, and the characteristics of the patients served. NCHS surveys hospitals, office-based physician practices, emergency and outpatient departments, ambulatory surgery centers, nursing homes, and home health and hospice agencies. These surveys provide a picture of how the delivery system works, and provide an opportunity to learn about patients, their illnesses, and treatment (http://www.cdc.gov/nchs/nhcs.htm)
- National Vital Statistics System - obtains information from death certificates in all 50 states and the District of Columbia, including characteristics of the decedent and causes of death. (http://www.cdc.gov/nchs/nvss.htm)
Other HHS sources for information on eating disorders and dietary behavior:
- CDC/Youth Risk Behavior Surveillance System (http://www.cdc.gov/HealthyYouth/yrbs/index.htm)
- NIH/National Institute of Mental Health (http://www.nimh.nih.gov/health/topics/eating-disorders)
- Substance Abuse and Mental Health Services Administration (http://mentalhealth.samhsa.gov/cmhs)
For further information about NCHS and its programs, visit us at http://www.cdc.gov/nchs, or call the Office of Planning, Budget and Legislation at 301-458-4100.
Page Last Modified: November 21, 2008
Data Source: CDC/National Center for Health Statistics
National Center for Health
Statistics
3311 Toledo Road
Hyattsville, MD 20782
Phone:
1-800-232-4636
nchsquery@cdc.gov
Centers for Disease Control and Prevention, 1600 Clifton Rd, Atlanta, GA 30333, U.S.A
Tel: (404) 639-3311 / Public Inquiries: (404) 639-3534 / (800) 311-3435