Fatality Assessment and Control Evaluation (FACE) Program |
|
Welder Dies from Fall off Rigging |
| |||||||||||
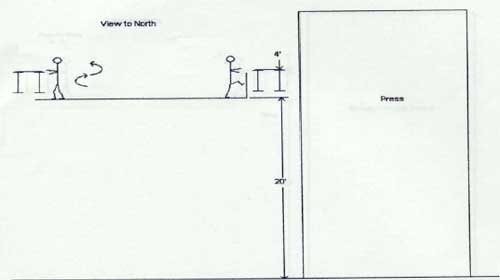
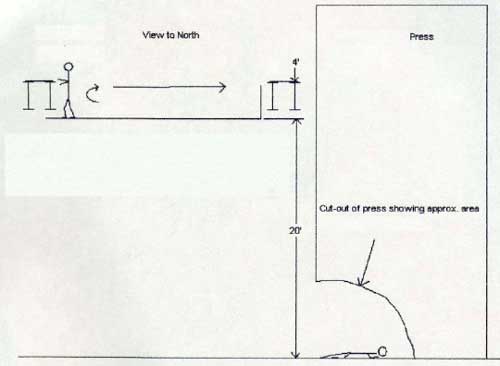
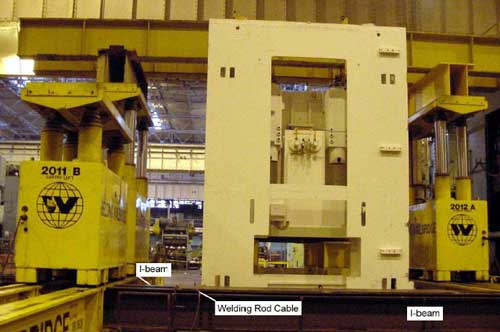
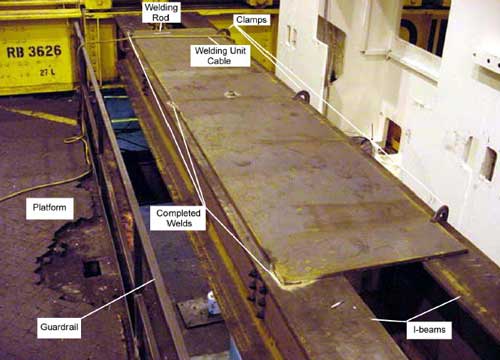
SummaryOn Saturday, November 22, 2003, a 44-year-old male welder fell 24 feet to a concrete floor at a metal stamping plant. He was a general welder in the plant's facility engineering department. The welder who fell, a co-worker who was an apprentice welder, and another worker were preparing the site for the installation of the top of a press, the crown, onto a large press. The crown was to be raised by a crane to a position in front of the press where it would be positioned onto a hydraulic lifting apparatus that traveled on rails located on either side of the press (Figure 1). The crown would then be raised by the lifting apparatus, rolled along the rails across the top of the press and set into place. Two I-beams in front of the press formed a bridge between the rails the lifting apparatus traveled along. The decedent and his co-workers were welding a steel plate to the top of the two I-beams to stabilize them to prevent them from twisting so they could support the weight of the crown as it was placed on the lifting apparatus. The decedent had tack-welded the steel plate onto the I-beam next to the platform he was standing on (Figure 2). He was preparing to tack-weld the far side of the plate onto the second I-beam that was closest to the press. The apprentice welder with whom he was working saw him start to climb over a guardrail onto the top of the plate to reach the far side of the steel plate, but then turned away to put some equipment away. When he next looked back in that direction, he did not see the decedent (Diagram 1). The decedent was not wearing any type of fall protection. He had fallen from the steel plate next to the left side of the press. When the apprentice welder realized that the decedent had fallen to the press floor below, he activated the 911 Emergency Call Box to notify the company's central emergency team, the plant nurse, and the plant emergency response team. The company's central emergency ambulance and team arrived within 4 minutes of receiving the call. The city's emergency medical team transported him to the hospital where he was placed in the trauma center. He was in a coma until he died approximately one month later on December 22, 2003.
IntroductionOn Saturday, November 22, 2003, a 44-year-old male welder fell 24 feet to a concrete floor. On November 22, 2003, MIFACE investigators were informed by the Michigan Occupational Safety and Health Act (MIOSHA) personnel who had received a report on their 24 hour-a-day hotline that a work-related serious injury had occurred. The decedent died in the hospital on Monday, December 22, 2003. On May 19, 2004, the MIFACE researcher interviewed a safety person within the company who had knowledge of the incident. He described the events on the day of the fatality as they had been told to him. She was shown pictures of the site taken after the incident occurred and obtained two for use in this report. During the writing of the report, the medical examiner's report, the company’s responding EMS run report, photographs, and the MIOSHA file and citations were reviewed. The plant in which the decedent worked stamps parts for the manufacture of automobiles. It employed approximately 1300 employees, 25 of whom had the same job title as the decedent, general welder. The decedent had been employed by the company and worked in this plant for 15 years. He was working overtime on a Saturday. The incident occurred at 8:40 a.m. Several people were working in the area at the time. At least one person saw him climb onto the steel plate beyond the guardrails, but this person did not see what he was doing before he fell. The company has a 3-day joint union/company training program specifically developed for working at heights in which the decedent had participated. The Wednesday before the incident, the decedent had been issued a harness and lanyard. However, the work being conducted required that the steel erection standard be followed. He had not received training under the steel erection standard. Maintenance employees and employees involved with "new construction" were those trained in steel erection. The decedent was not included in those categories. No one in the plant in a supervisory capacity on the day of the incident had been trained in fall protection requirements for either construction or steel erection. The MIOSHA investigation resulted in three Serious violations being issued to the company: Handling and Storage of Materials, Part 8, Rule R408.40836(5) addressed the use of structural steel nuts that were not rated for the lifting/setting type of installation/application being conducted; Steel Erection, Part 26, Rule 2645(1) addressed failure to protect an employee from fall hazards, and also, the use of a horizontal lifeline system in a manner for which it was not designed; Steel Erection, Part 26, Rule 2653(2) addressed the failure to follow the company's training program, the failure to identify unsafe actions of others and take immediate corrective action, and the failure to correctly erect/use the designed horizontal lifeline systems. Back to TopInvestigationOn Saturday, November 22, 2003, a 44-year-old male welder fell 24 feet to a concrete floor at a metal stamping plant. He was a general welder in the plant's facility engineering department. At the time of the incident there were five to six salaried and approximately 25 hourly employees in the plant doing assorted tasks. The decedent, a co-worker who was an apprentice welder, and another worker were preparing the site for the installation of the top of a press, the crown, onto a large press. The crown was to be raised by a crane to a position in front of the press where it would be positioned onto a hydraulic lifting apparatus that traveled on rails located on either side of the press (Figure 1). The crown would then be raised by the lifting apparatus, rolled along the rails across the top of the press and set into place. Two I-beams in front of the press formed a bridge between the rails the lifting apparatus traveled along. The decedent and his co-workers were welding a steel plate, 3/4 inch thick and approximately 3 feet by 8 1/2 feet, to the top of the two I-beams to stabilize them to prevent them from twisting so they could support the weight of the crown as it was placed on the lifting apparatus. The decedent had tack-welded the steel plate onto the I-beam next to the platform he was standing on (Figure 2). He was preparing to tack-weld the far side of the plate onto the second I-beam that was closest to the press. An opening of approximately one foot existed between the I-beam and the front of the press. The apprentice welder with whom he was working saw him start to climb over a guardrail onto the top of the plate to reach the far side of the steel plate, but then turned away to put some equipment away. When he next looked back in that direction, he did not see the decedent (Diagram 1). The decedent was not wearing any type of fall protection. No one actually saw him fall from the steel plate to the press floor 24 feet below. He had fallen from the steel plate between the hydraulic lift (2011B) and the left side of the press. The electric welding unit was examined and found to be in good condition. The welding rod had not been connected to the welding lead. No burn marks were noted when he was being tended to by the emergency responders. No reason for his fall was apparent. When the apprentice welder realized that the decedent had fallen to the press floor below, he activated the 911 Emergency Call Box to notify the company's central emergency team, the plant nurse, and the plant emergency response team. The company's central emergency ambulance and team arrived within 4 minutes of receiving the call. The city's emergency medical team transported him to the hospital where he was placed in the trauma center. He was in a coma until he died approximately one month later on December 22, 2003. There were employees in the plant who had had the appropriate steel erection training to conduct the work, but the work coordinator with responsibility for overseeing the decedent's task was not informed of their presence. They were from another area of the company that conducted work in all the plants at the site. When the coordinator learned of their presence in the plant, he planned to replace the decedent and his co-workers with these other employees. He was on his way to do so when he learned of the decedent's fall. Back to TopCause of DeathThe cause of death as stated on the death certificate was acute myocardial infarction as a consequence of a closed head injury. No autopsy was performed. Back to TopRecommendations/DiscussionRecommendation #1: Management and employees must work together to develop a plant culture that will not allow actions that might result in injury or death to be tolerated.The apprentice welder saw the decedent climb onto the plate without fall protection but said nothing to him. The culture of a plant allows this to happen. Even after safety training, there is no guarantee that safe practices will be followed. Job demands and previous use of shortcuts may be an encouragement for employees to go back to the “shortcut” way of performing the work. The employee may use his/her past experience is a guide – he/she may have done the work successfully and injury free using the shortcut. Companies that permit, encourage, allow, fail to identify and correct these inappropriate behaviors reinforce that behavior and give tacit approval to the unsafe action. The company’s safety culture, i.e., the safety attitudes, beliefs and behaviors that are generally shared within the organization, must have attention to safety in all activities. Management must demonstrate a commitment to safety and make it a high priority. Management must supervise the work of individuals and provide positive reinforcement for safe behaviors and negative consequences for unsafe behaviors. Employees must be aware of the importance of safety in their actions and be knowledgeable and competent to perform their jobs.
| ||||||||||||
 |
 |
|
Diagram
1. Depiction of Events |
MIFACE (Michigan Fatality and Control Evaluation), Michigan State University (MSU) Occupational & Environmental Medicine, 117 West Fee Hall, East Lansing, Michigan 48824-1315. This information is for educational purposes only. This MIFACE report becomes public property upon publication and may be printed verbatim with credit to MSU. The author of this report is affiliated with Wayne State University. Reprinting cannot be used to endorse or advertise a commercial product or company. All rights reserved. MSU is an affirmative-action, equal opportunity employer.
MIFACE Investigation Report # 03MI179 Evaluation (see page 9 of report)
To contact Michigan State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.