Fatality Assessment and Control Evaluation (FACE) Program |
|
A Supervisor Dies When Crushed by a Machine That Manufactures Concrete Blocks |
| |||||||||||||
SummaryA 52-year-old Hispanic supervisor died when he was crushed in a machine used in manufacturing concrete blocks. Evidence suggests that the victim had climbed on top of the machine, possibly to reconnect an air line. The victim did not shut the machine down and lock and tag it out prior to climbing on top of it. The skip hoist had dumped product into the hopper portion of the machine and was on its down cycle when the incident occurred. There were no guards in place to prevent the victim from climbing on the machine while it was running. The CA/FACE investigator determined that, in order to prevent future occurrences, employers, as part of their Injury and Illness Prevention Program (IIPP), should:
In addition:
IntroductionOn June 10, 2005, at approximately 7:20 a.m., a 52-year-old Hispanic supervisor was crushed between the structural frame and skip hoist of a machine that makes concrete blocks. The CA/FACE investigator learned of this incident on June 23, 2005, through the Legal Unit of the Division of Occupational Safety and Health (Cal/OSHA). Contact with the victim’s employer was made on June 26, 2005. On July 26, 2005, the CA/FACE investigator traveled to the facility where the incident occurred and interviewed the plant manager and employees. The machine involved in the incident was photographed, and the area where the incident took place was examined. The employer of the victim was a concrete block manufacturing company. The company had been in business for over 50 years and had over 300 employees throughout its eight locations. The facility where the incident took place employed 26 people. The victim had been employed with the company for 15 years and at the facility where the incident occurred for two years. The victim was born in Mexico and had been in the United States for the past 33 years. According to his employer, he spoke both English and Spanish. The company had a written safety program in English. The program had procedures that were task-specific for employees to follow, including a lockout/tagout procedure. Safety meetings were held quarterly and were documented. The company had a training program that provided specific training to its employees for the machines being operated, including lockout/tagout. The training program consisted of a combination of classroom and on-the-job training. The victim taught most of the training for the company. Training was measured and verified by having the employee repeat back what was taught. Back to TopInvestigationThe site of the incident was a concrete masonry and interlocking concrete pavement manufacturing plant. The machine involved in the incident was an automatic block-making machine that formed and molded concrete blocks. On the day of the incident, the victim was performing his regular duties supervising employees who ran the automated systems and overseeing production. Physical evidence suggested that the victim climbed up on the automated block-making machine, most likely to connect an air line to the vibrating mechanism located on the outside and on the bottom of the hopper. The vibrating mechanism, which was retrofitted to the hopper, helped move the concrete mixture through the hopper depending on the product’s consistency. The air line had to be connected to the vibrating mechanism whenever it was needed, but it was not used all the time. The skip bucket cycle was automatic and was sequentially timed to keep the hopper filled with the concrete mixture needed to make the concrete blocks. No one witnessed the victim climb up onto the machine while it was running, but the machine operator saw the victim being dragged between the frame of the machine and the skip loader which was on a down cycle. The victim then dropped onto the machine mechanism below. The operator immediately shut off the machine and went to get help. Paramedics responded and treated the victim, and then transported him to a local hospital where he died from his injuries. Back to TopCause of DeathThe cause of death, according to the death certificate, was mechanical compression of torso. Recommendations/DiscussionRecommendation # 1: Ensure employees follow the proper lockout/tagout procedures on machinery before performing any repair, maintenance, connection, or adjustment.Discussion: Without the benefit of lockout/tagout, employees cannot be assured of their safety when climbing onto or into a machine, especially when the machine has not been properly shut down and all sources of energy dissipated. In this case, the machine was not stopped when repairs, maintenance, connections, or adjustments were needed by pressing an emergency stop button on the control panel. The machine was never locked out; therefore, the moving parts of the machine were in motion when the victim climbed onto the machine. Although the company had a lockout/tagout program, it was not being used in this case. Lockout/tagout programs should address the following issues:
Additionally, employers can encourage manufacturers to design machines and systems that make it easy to control hazardous energy.
| ||||||||||||||
 |
Exhibit 1. The automated machine
that made concrete blocks. |
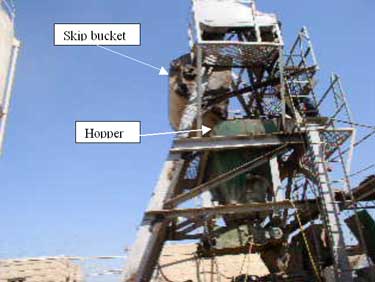 |
Exhibit 2. The portion of the
machine the victim climbed onto. |
 |
Exhibit 3. The place on the
machine where the victim was dragged by the skip bucket. |
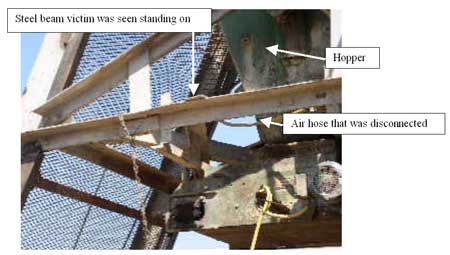 |
Exhibit 4: The portion of the machine
frame the victim was dragged between by the skip bucket. |
 |
Exhibit 5: The portion of the machine
the victim fell to after he was crushed by the skip bucket and machine frame. |
The California Department of Health Services, in cooperation with the Public Health Institute and the National Institute for Occupational Safety and Health (NIOSH), conducts investigations of work-related fatalities. The goal of this program, known as the California Fatality Assessment and Control Evaluation (CA/FACE), is to prevent fatal work injuries in the future. CA/FACE aims to achieve this goal by studying the work environment, the worker, the task the worker was performing, the tools the worker was using, the energy exchange resulting in fatal injury, and the role of management in controlling how these factors interact. NIOSH-funded, state-based FACE programs include: Alaska, California, Iowa, Kentucky, Massachusetts, Michigan, Minnesota, Nebraska, New Jersey, New York, Oklahoma, Oregon, Washington, West Virginia, and Wisconsin.
To contact California State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site. Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
