| New York Case Report 00WA012 |
Release Date: December 27, 2004 |
Summary
On February 26, 2000, a 24 -year-old temporary employee died when he
was caught in a piece of machinery at a soft drink bottling plant. The
victim was an operator on the bottle depalletizer/bottle conveyor line. The
victim was employed and placed
at the bottling plant by a temporary employment service agency. He had
been on the job for about two years at the time of the incident. Somehow
the victim got caught in a machine called a chipboard remover, which was
part of a depalletizer conveyor system that was designed to remove empty
soft drink bottles from a pallet and funnel them single-file into the
system to be filled and capped. There were no witnesses to the incident.
Co-workers discovered the victim caught in the machine when they went
to find out why the bottle line had stopped. A call was placed to 911
and first aid and CPR were given to the victim immediately after being
removed from the machine. The local fire department emergency medical
team continued CPR on the victim but were unsuccessful and the victim
died at the scene as a result of his injuries.
To prevent similar occurrences, the Washington Fatality Assessment and
Control Evaluation (FACE) investigative team has identified the following
guidelines and requirements:
- Ensure that all machinery is properly safeguarded to prevent the exposure
of any part of a worker’s body to hazardous aspects of the machine’s
operation.
- Equip conveyor system with an emergency stop cable or similar safety
device that runs the entire length of the conveyor.
- The employer should work with the equipment manufacturer to address
safe processes to deal with equipment jamming and other operational
issues.
- Temporary employment service agencies should work with secondary
employers to establish specific job descriptions, training criteria,
and hazard analyses of each job assigned to temporary employees.
- Use a hand tool to help clear jammed or fallen containers, to prevent
exposure of any body part to the machinery.
Introduction
On February 28, 2000, the Washington State FACE Program was notified
by WISHA*, of the death of a 24-year-old bottling
plant worker in western Washington. The Washington FACE Field Investigators
met with the WISHA enforcement representatives for the region in which
the fatal incident occurred. The WA FACE team then traveled to the incident
site with the compliance inspectors where they met with the representatives
of the bottling plant involved in the incident.
The Washington FACE team also contacted the temporary employment service
agency (TESA), the primary employer in this case, and met with representatives
of the agency. The TESA has been in business nationally for over 50 years
and has over 4,000 owned and franchised offices worldwide. The local office
had been in the area for about 25 years. The total TESA office staff varied
from two to five full-time and part-time employees.
The local office of the TESA does not employ a safety person to oversee
their operations’ health and safety processes or training, but their
corporate and regional management did assign responsibilities and guidance
to the local office staff. When a new employee signs with the agency,
a local staff member provides a very brief, general safety orientation
to the new employee. The secondary employer (the bottling plant) involved
in the incident had a regular working relationship with the TESA to contract
labor to work at the bottling plant and at the time, only about 5% of
their employees were employed by the TESA.
The bottling plant is part of a multi-plant co-op of 10 soft drink franchise
operations located throughout the northwest. The bottling plant has been
in operation since 1992 and employs approximately 125 workers. The plant
had both new and temporary employee orientation processes. Written orientation
checklists were essentially identical for both new and temporary employees.
The plant supervisors, along with the human resources manager, had the
responsibility for new and temporary employee orientation. The company
did not have written job descriptions that outlined the duties of each
operation.
Either a plant supervisor or employee conducts “on the job”
training with the new and temporary employees prior to the employee being
assigned a job duty on their own. Depending on the complexity of the job
and other factors, training can range from one day to one week. Once the
new employee has been given the job to run on their own, there also may
be a week of observation.
The facility had an accident prevention program and had conducted hazard
analysis reviews on some elements of their production operations, but
the analyses were limited in scope and did not address the hazard involved
in the fatal incident. The plant had a safety committee that met on a
monthly basis at their facility, though none of the temporary employees
were on this committee.
The bottling plant was running their “plastic container”
soft drink bottling process under routine conditions at the time of the
incident. The victim was a 24-year-old male (temporary employee), who
was working as a depalletizer line operator at the bottling plant on the
date of the incident. His primary job was to manage the depalletizer machine,
which introduces empty containers (20 oz. bottles on the date of the incident)
into the production process, which are then filled with the soft drink
product that the line was running that day. The victim had worked at the
bottling plant on and off, as a temporary employee for just under two
years. Most of that time he had worked as a depalletizer operator.
The TESA records showed, via signed documents, that the victim had received
the agency’s very basic health and safety training prior to entering
employment at the bottling plant, approximately 2 years prior to the incident.
Specific training related to the employee’s job and the bottling
plant safety process were conducted at the bottling plant. The bottling
plant did not have any documentation of the victim’s training, as
they believe the records where purged after maintaining them for a year.
On the evening of February 26, 2000, the victim was caught in the depalletizer
machine that he was operating as part of the company’s soft drink
processing line. Co-workers responded after they noticed the process line
had stopped and saw the victim caught in the machine. A call was placed
to 911 and they began CPR prior to the arrival of a local fire department’s
emergency medical rescue unit. The victim died of his injuries at the
scene of the incident.
* Washington Industrial Safety and Health Act (WISHA), which is the OSHA
State Plan program in Washington State.
Back to Top
Investigation
On February 26, 2000, a Saturday evening, the victim was working the
second shift at a bottling plant in western Washington State. He had reported
to work at 2:30 PM, which was the normal start time for second shift.
The victim had been hired as a temporary employee via a TESA to work
at the bottling plant. He had worked there on and off for about two years.
His job at the time of the incident was to run the depalletizer line and
he had performed that job for about a year.
A supervisor at the plant indicated that the victim was very familiar
with the operation of the depalletizer. He also said that this part of
the process line was one of the easier parts of the operation and required
only a limited amount of training and supervision.
The depalletizer is an automated machine that transfers empty containers
(bottles and cans) from stacked palettes to single-file on the processing
line (see Figures 1, 2, and Photo
1). Pallets are brought by forklift from the bottling plant’s
container storage area and set into the initial feed mechanism of the
depalletizer.
The depalletizer raises the palletized stack of bottles up from floor
level to the operator’s workstation level (approximately 12ft from the floor).
The depalletizer mechanism then sweeps forward one layer of the palletized bottles that
are packed in an 11 by 12 formation, and funnels them into a single file
where a conveyor moves the bottles to the labeling and fill line.
Each layer of bottles on the pallet was separated by a piece of chipboard
(tier sheet/slip sheet) which travels with the stack of bottles up the
depalletizer hoist until it reaches the chipboard remover mechanism at
the top. The chipboard remover has five vacuum suction cups which descend
automatically onto the chipboard that covers each layer of bottles and
lifts the chipboard off the bottles (Photo 2 and
3). An electronic sensor triggers this action when
it senses the layer of bottles entering the chipboard remover area. The
suction cups apply approximately 20 pounds of vacuum pressure to lift
the chipboard approximately 2-1/2 ft off the layer of bottles. The chipboard
remover then moves approximately 5 -1/2 ft to the right and drops the
chipboard onto a stack of removed chipboards. The stack is periodically
taken out of the system by one of the bottling plant workers.
Once the chipboard is placed in the stack, the chipboard remover swings
back to the original position to pick up the next chipboard. Simultaneously,
the new layer of bottles is moved to the left by the sweeper arm onto
the conveyor that sends the bottles to the labeling and filling operations.
As the bottles travel along the conveyor system, an electronic sensor
sends a signal to the system to raise the next layer of bottles in place
for depalletizing. According to a bottling plant supervisor, this process
takes approximately 20-25 seconds to cycle each layer of bottles through
the system.
Sliding plexiglass interlocked guards (doors) prevent access to the front
of the chipboard remover from the operator’s side of the work platform. There was
a 16” x 24” opening in the guarding between the stack of bottles
and the removed chipboard sheets to allow the worker access to remove
the wooden stabilizing ring that is placed on top of the pallet load of
bottles. Prior to the chipboard remover cycling through its process, the
depalletizer operator had to reach into the opening and cut and remove
two straps and a large wooden ring off the top of the pallet of empty
bottles while it was in the depalletizer. This operation was done while
the machine was turned off.
Once the bands are cut and the wooden ring removed, the depalletizer
operator had to walk off the work platform and go down to the depalletizer
control panel located on the manufacturing floor level and set the machine
to the run mode. This re-activates the automatic cycle of removing the
chipboard and sweeping each layer of empty plastic bottles onto the conveyor.
The operator then walks back up to the operating platform and activates
the system at the control panel.
On the afternoon of Saturday February 26, 2000, the victim reported to
work at 2:30 PM as usual for the start of the second shift at the bottling
plant. A supervisor relieved the victim at approximately 4:15 PM for his
first break during the shift. Sometime between 6:00 and 6:30 PM, the supervisor
noted the victim at his workstation and noticed nothing out of the ordinary.
Between 7:15 PM and 7:45 PM the victim ate dinner with a co-worker in
the facility break area.
The line had been running well that evening until 8:01 PM, when down
time was recorded for a gap in the bottles traveling down the conveyor
from the victim’s work station to the fill line (i.e. the bottles
weren’t continuously being supplied to the processing line). At
8:05 PM the line was running again.
At 8:10 PM there was another gap in the bottles in the process line.
This time the line did not resume running and the system “jam”
warning light remained on. The labeler operator went to check to see why
bottles were not moving. He saw a bottle jam and went to clear the line.
He was about 30 feet from the depalletizer and observed the victim bent
over doing something on the machine. The labeler operator went back to
his work area, looked back and saw the victim caught in the chipboard
remover apparatus. Then he ran up to the victim’s location and found
the victim face down on a piece of the chipboard in the chipboard removing
apparatus. The labeler operator yelled at the victim to see if he was
all right but the victim did not respond.
The labeler operator hit the manual depalletizer control button to lift
the chipboard remover mechanism off of the victim but it was already at its highest point. He
noticed that the victim’s shirt was tangled around one of the chipboard
remover’s suction cups. When he realized that he was not going to
be able to get the victim free of the machine, he yelled to another co-worker
to call 911 and get additional help using his portable radio.
Several co-workers and the operation supervisor responded to the call
for help. They found the victim jammed in the machine. One of the co-workers
removed the interlocked safety doors from the front of the machine in
order to get to the victim. The victim was laying face down with his right
arm pressed under his body. His left arm was hanging down near the depalletizer
hoist. His upper body was wedged in the machine past his waist. It appears
as if the victim may have reached into the machine, past the safeguarding
system. His shirt and belt were tangled in the suction cups. It was noted
that the victim had a gash on his forehead and he had a blue color and
no pulse. The victim was eventually removed from the depalletizer by co-workers.
Co-workers started CPR as soon as they got he victim free of the machine.
The local fire department arrived within 10 minutes of being summoned
and continued CPR on the victim but to no avail. The victim was pronounced
dead at the scene.
The incident was unwitnessed, so no one saw the victim at the point in
time when he got caught in the machine. The victim’s co-workers
thought that he may have been pulled into the machine while trying to
reach in to align a bottle that had fallen. It was reported that sometimes
a plastic bottle will fall and block the electronic eye and stop the depalletizer
process until the bottle is cleared. Workers indicated that the 20 oz.
bottles, that were being run, had more instability problems than other
types of containers. They indicated that they often had to clear a minor
jam or re-align these bottles during the depalletizer process. On average
the workers indicated that they might have to deal with this 9 or 10 times
a shift while working the depalletizer.
The workers all agreed that there should be no reason for anyone to get
their hands or body into the system while the machine was running. The
way operators were instructed to deal with a “downed” bottle
was to switch the machine from automatic to manual mode at the control
panel, and then open the interlocked sliding doors that are the physical
machine guards for that apparatus. The interlocked doors shut the machine
down. The operator can then safely reach in and take care of the fallen
bottle. With the interlocked doors placed back in position, the machine
would then be reactivated and placed into automatic mode and the line
could proceed with the bottling process.
Cause of Death
The medical examiner listed the cause of death due to, or as a consequence
of, traumatic asphyxia or external chest compression after being caught in a machine.
Recommendations/Discussion
Recommendation #1: Ensure that all machinery is properly safeguarded
to prevent the exposure of any part of the body to hazardous aspects of
the machine’s operation.
Discussion: The victim in this incident was caught in
the machine that he was operating and died from the resulting crushing
pressure applied to his chest by a portion of the automated system. The
victim caught his upper torso in a space between the bottle depalletizer
conveyor system and the chipboard remover. The depalletizer conveyor system
appears to be very innocuous at first glance, but from a systems safety
approach, there are a variety of operational and physical hazards related
to this process. A full description of the process is found in the investigation
section of this report.
Given the fact that the bottles can get out of alignment and fall down
and/or jam the conveyor line, the operator must re-align the bottles and/or
un-jam the system. The point where the layer of bottles enters the chipboard
remover is only partially guarded. It is guarded in the front of the operator’s
work platform but is open between the stack of bottles and stack of chipboard
to allow the operator to remove the wooden stabilizing rings which are
approximately 3ft by 4ft.
If there is a problem in the area of the chipboard remover requiring
the operator to get into the system, the operator is supposed to open
interlocked guards (plexiglass doors), which shuts down the automatic
cycle of the chipboard remover and the conveyor system.
In this incident, the victim did not open the interlocked chipboard remover
guard, but physically put his body in the opening between the conveyor
and the guard and was able to access the space adjacent to the chipboard
remover apparatus. He by-passed the guard and safety interlocking device
that was on the equipment.
The guard on this machine allowed a person to get their arms and body
into a hazardous part of the machine, which resulted in the death of the
victim. The bottling plant should work closely with the equipment manufacturer
and get their help to devise additional guarding and safe operational
practices for employees who run and maintain the depalletizer system.
It is very important, and is especially true when automated moving and
reciprocating machinery is involved, that effective guarding be in place
to prevent a worker from coming in contact with or be pulled into a hazardous
area of the operating machinery.
Recommendation #2: Equip the conveyor system with an emergency stop cable
or similar safety device that runs the entire length of the conveyor.
Discussion: In this incident, the victim by-passed the existing interlocked
machine guard system and was caught in the chipboard remover. In addition
to the interlocked guard, the depalletizer system was also equipped with
an E-stop (emergency stop) at the operator’s control panel located
at the depalletizer work platform. The E-stop, if activated would have
shut down the machine. The Estop had not been activated during the incident.
Once the victim was caught and pulled into the chipboard remover, he would
not able to reach the E-stop to shut down the machine.
There are many types of safe guards available that could have been activated
to stop the machine. They range from basic mechanical/electronic emergency stop systems
to more sophisticated technology such as light curtains and a variety of automated
sensing devices that can detect objects, other than the desired materials,
entering hazard zones.
Emergency stop cables or safety trip wires are commonly used safety stop
devices on conveyor systems. Safety trip controls provide for a quick
method of shutting down a machine in an emergency. Safety trip wires should
be situated and located around the perimeter of the machine/conveyor and
be easily accessible to persons working near it, so it can be quickly
shut down. If safety stop cables/trip wires had been available, the victim
may have suffered a much less severe injury.
There are also a number of different types of presence sensing devices
to choose from. These devices range from photoelectric sensors to radio
frequency devices and electromechanical systems. Photo electrical (e.g.
light curtains) devices for example, use a light source with controls
that stop or interrupt a machine’s operation. If the light field
is broken, a signal shuts the machine down and has to be reset in order
for it to start up again. Since the incident, the company has installed
light curtains around the depalletizer machine operation to provide increased
protection to help prevent a similar event from occurring.
It is important that emergency stop mechanisms be tested at the start
of every shift if possible, to ensure operational safety. If the safety
devices are not working properly, they must to be repaired prior to the
operation of the machine.
Any and all safety devices that a company plans to add to their equipment
should be reviewed with the equipment manufacturer.
Recommendation #3: The employer should work with the equipment manufacturer
to address safe processes to deal with equipment jamming and other operational
issues.
Discussion: The depalletizer in this incident is a machine
designed to function in both manual and automatic mode depending on the
situation and the material being processed. Since the containers vary
depending on production needs, the system is designed to be as versatile
as possible without making major mechanical changes or adjustments. The
system is programmable to allow for the operating parameters to be entered
and machine adjusted to the size container being run.
Often times, there are problems with automated machines that are designed
to be versatile. This may have been the case with this bottling line.
The machines may be capable of running some of the materials/containers
through the system well, but could have problems running one or two of
the types of containers.
It appears that this might have been the case with the 20 oz. plastic
bottles. According to the workers at the bottling plant, the 20 oz bottles
gave them the most trouble when running the depalletizer. Some of the
problems they experienced were that the bottles would fall and either
jam the system or they would get in the way of the sensor and would keep
the automated process from running. There are a number of potential factors
leading to the problems associated with running the 20 oz. containers
such as size, weight, center of gravity, design of the bottles, and the
stacking of bottles on the pallets, that would effect how well the bottles
could run on the system.
The problem with running 20 oz. bottles seemed to be well recognized
by the supervisors and the workers running this equipment. It is recommended
that the employer should work with the equipment manufacturer to address
safe processes to deal with equipment jamming and other operational issues.
Manufacturers are often willing to help the customer address not only
production and quality issues but also help them with safety concerns
associated with the operation of their machinery. The manufacturer might
have a solution to the problem that is already on hand or could be in
the process of actively working on a solution.
The manufacturer can be an important partner in reviewing safety and
operational problems and should be contacted to develop processes and
procedures, help make equipment adjustments, and help establish safeguards
to eliminate or minimize the risk of an injury involving the equipment.
Some depalletizer manufacturers have container stabilization capabilities
designed into their systems, which might have eliminated or reduced the problems that this
employer was experiencing. One company has a vacuum system that keeps the bottles in
place during the depalletizing process while another has four guides that hold the bottles
in place while the chipboard is removed.
Recommendation #4: Temporary employment service agencies should work with
secondary employers to establish specific job descriptions, training criteria,
and hazard analyses of each job assigned to temporary employees.
Discussion: In this fatal incident, the victim, in essence
was working for two employers, the TESA (the primary employer) and the
bottling plant (the secondary employer). Both employers had developed
and utilized safety training programs that were presented to each employee
prior to beginning work.
Although there were positive elements in each of the employer’s
training programs, there also were weaknesses. These weaknesses failed
to provide the support to the worker that was needed for him to gain the
knowledge and understanding of the job tasks and the safe operational
responsibilities of the machine.
It is recommended that each employer work more closely with the other
to establish and develop more defined, specific job descriptions and duties
for each employee assigned to the bottling plant by the TESA. This should
also extend to all of the TESA’s client companies.
A hazard analysis of the job should be conducted and reviewed jointly
by each employer (bottling plant and TESA). Identified hazards should include appropriate
controls to prevent worker injuries. Any changes to production processes
and procedures should initiate a new hazard analysis of the job.
The bottling plant (secondary employer) has direct supervision over the
employee and therefore is responsible for providing training specific
to job requirements. The TESA (primary employer) should review training
contents and have a process to assure that appropriate training is available
and presented in an effective manner to employees before they begin work.
Employee training, including that for temporary workers, should not only
encompass all required training, as mandated by regulatory agencies such
as OSHA or WISHA, but include job specific training that incorporates
the elements of the job hazard analysis and detailed safety measures that
need to be applied while on the job. The training should not only include
the various elements of performing the job, but should also discuss what
to do when there are system upset conditions and the machine does not
run correctly or jams. Training should include how to properly shut down
the machine, use the emergency stop systems, safely clear a jam, safely
remove and re-align downed bottles, and safely cut the bands and remove
the wood rings from the bottle pallets.
The training should detail what processes or procedures should be followed
and what to do in an emergency situation. The importance of training employees
on safe operating procedures should be emphasized and discussed in sufficient
detail that the information is understood and provides clear expectations
from management on how the job is to be performed safely by the employee.
Documentation of training contents, presentation and evidence of effectiveness
is recommended.
Recommendation 5: Use a hand tool to help clear jammed or fallen containers
to prevent exposure of any part of a worker’s body to the machinery.
Discussion: In this automated bottle depalletizer process,
there are a variety of possible ways to deal with routine upsets of equipment
or material in the container processing line. As we have discussed in
the earlier recommendations, improved machine guarding and mechanical
process changes would help prevent serious incidents by helping engineer
out the hazard and exposure to the hazards.
Another recommendation that could be explored is to find a tool that
could be used to pick up or realign downed bottles and to remove bottles
that are causing a jam in the process. The bottling plant should consider
working with the equipment manufacturer and an industry association that
can help identify a safe tool that can be used to pick up downed bottles
that are causing production problems on the depalletizer line.
There are a variety of extension grabbers and reaching tools available
on the market that could work with bottles and similar objects.
It is very important that the tool be used correctly and safely within
acceptable operating conditions when performing the job. The tool should
not create an additional hazard. The tool should not
be used to bypass safety devices and guards designed for worker protection
when the machine is in operation. Specific training and guidelines for
the use of the tools should be developed and training conducted for each
individual who might have a need to use the tool.
The depalletizer system should be shut down and locked-out prior to the
use of any tool within the system that would expose a worker to caught-in
hazards of the machinery.
Ensuring the safety of workers is a critical mission that requires a
multi-faceted approach. The fatal incident described in this report highlights
this fact. In combining a machine and process that periodically would
allow bottles to fall and disrupt the flow of product, with machine guarding
that allowed worker access to a potentially hazardous area of the machine,
and possible worker incentives to keep the processing line in operation,
a deadly situation developed. Only by using a systems approach that addresses
the entire process, including the machine, the interface between the workers
and the machine, the workers’ training, the workplace’s safety
culture, and the physical work environment, can this hazard and other,
unforeseen hazards be truly controlled to prevent serious injury and death.
Because this incident involved the interaction of a temporary worker with
two different employers, it is especially important to formalize this
systems safety approach so it is carried out for the protection and benefit
of all parties involved.
Back to Top
Resources
- Contingent Workers: Incomes and Benefits Lag Behind Those of the
Rest of Workforce. United State General Accounting Office. GAO/HEHS-00-76.
June 2000.
- Lamar, Gregg. Contingent Worker Safety: A Full-Time Job in a Part-Time
World. Occupational Hazards. October 1997.
- Worker Protection: Labor’s Efforts to Enforce Protections
for Day Laborers Could Benefit from Better Data and Guidance. United
States General Accounting Office. GAO-02-925. September 2002.
- Aronsson, Gunnar. Editorial: A new employment contract. Scandinavian
Journal of Work, Environment & Health, Vol 27, No. 6. 2001
- Naso, Markisan A. Safety is never Temporary: Short-term workers
become hot commodities during economic rebounds. Keeping them safe should
always be a priority. Safety & Health. April 2002.
- Rousseau, Denise M., Carolyn, Libuser. Contingent workers in high
risk environments. California Management Review, Berkley. Winter
1997.
- Foley, Michael P. Flexible Work, Hazardous Work: The Impact of
Temporary Work Arrangements on Occupational Safety and Health in Washington
State 1991-1996.Research in Human Capital and Development, Volume
12, JAI Press Inc. 1998.
- Safety Standards for General Safety and Health, Chapter 296-24 WAC,
State of Washington, Department of Labor and Industries.
- Kochan, T.A. Managing workplace safety and health: The case of
contract labor in the U.S. petrochemical industry. Lamar University
Press, Dallas TX. 1991.
Acknowledgements
In conducting the investigation of the death of a worker at a bottling
plant, the Washington State FACE investigation team requested that the
contents of this report be reviewed by key representatives from the labor
and business communities involved and Washington State and Federal worker
safety agencies, prior to it's publication.
Though we are not able to acknowledge specific individuals for their
invaluable input into this document, we would like to recognize the following
for their help and support to the FACE process:
• The bottling plant employer involved in the incident
• The temporary employment service agency employer involved in
the incident
• WISHA Enforcement
• WISHA Policy & Technical Services staff
• Federal Face Program Management (NIOSH)
• Safety & Health Assessment & Research for Prevention
(SHARP)
• Washington State Labor Council
• Center for a Changing Workforce
• Washington State Attorney Generals Office
Back to Top
Appendix - Other issues for Temporary Worker Health & Safety
Temporary workers or employees of a temporary services employment agency
(TESA) are only one of many types of contingent workers. Temporary workers
generally have two employers: the TESA who pays their salary, benefits,
and workers’ compensation insurance and the employer at the work
site who controls the work environment and conditions.
This is a relatively common arrangement for a number of business reasons.
Some of which are to:
• Accommodate seasonal and non-seasonal supplies of and demands
for their
products and services and thus employees,
• Fill in for permanent workers’ vacation and sick leave,
• Evaluate and hire workers for permanent positions,
• Reduce overhead from benefits and workers’ compensation
costs, and
• Increase the employers’ flexibility for downsizing of
their workforce.
Having two employers can lead to a number of safety-related outcomes
ranging from both employers being very responsible and assessing all hazards and doing all
that is within their power to reduce the hazards in the workplace to one where neither employer
takes responsibility for the temporary workers. In the incident that was investigated
in this report, both employers took some responsibility, but neither took ultimate responsibility.
For the TESA, this mainly entails site-specific assessments, worker training,
and possibly the supply of appropriate personal protective equipment.
Because the TESA doesn’t directly control the work site, it can
be difficult for them to change how the workers interact with the hazards,
let alone, physically control the hazards. Because the TESA may control
the work site employers’ source of employees, it may be possible
for them to leverage that control and get the work site employer to effectively
control their exposures.
For the work site employer, this entails site-specific assessments, worker
training, and physically reducing hazards using an assortment of control
strategies. It is also within the work site employer’s realm to
affect the work site’s safety culture. It is not known for certain
if it was a factor in this case, but temporary workers may feel pressure
to be more productive than their permanent worker counterparts if there
is the possibility of being hired as a permanent employee of the work
site employer. With this type of incentive, workers may ignore certain
safety rules, that if broken would have a low probability of causing an
injury, but a high probability of increasing their short-term productivity.
By setting up a work site safety culture that values safety more than
productivity, opportunistic activities that favor productivity over worker
safety can be reduced.
These activities must be accomplished with coordination between the TESA
and the work site employer. Hazards must be assessed, control schemes
evaluated, and the system for rolling temporary workers into permanent
positions evaluated for potential incentives to disregard personal safety
for job advancement. Both employers need to assess and alter their safety
cultures if they find productivity over-rules worker safety.
Back to Top
Appendix 2 – Applicable Regulations
In reviewing the WISHA standards, there are defined requirements that
deal with manufacturing and temporary labor agency safety and health issues.
Although the investigation of this incident was not regulatory in nature,
we offer the following code requirements for information and reference
purposes. This is not intended to be a complete list of regulatory guidelines
that address these issues but are representative of requirements established
under the Washington Administrative Codes:
Machine guarding:
Types of guarding. One or more methods of machine guarding shall be provided
to protect the operator and other employees in the machine area from hazards
such as those created by point of operation, ingoing nip points, rotating
parts, flying chips, and sparks. Examples of guarding methods are - barrier
guards, two-hand tripping devices, electronic safety devices, etc. WAC
296-24-15001 (1)
Point of operation guarding:
The point of operation of machines whose operation exposes an employee
to injury, shall be guarded. The guarding device shall be in conformity
with any appropriate standards therefore, or, in the absence of applicable
specific standards, shall be so designed and constructed as to prevent
the operator from having any part of the employee's body in the danger
zone during the operating cycle. WAC 296-24-15001 (3) (b)
Special hand tools for placing and removing material shall be such as
to permit easy handling of material without the operator placing a hand
in the danger zone. Such tools shall not be in lieu of other guarding
required by this section, but can only be used to supplement protection
provided. WAC 296-24-15001 (3) (d)
Programmatic:
Establish, supervise, and enforce rules that lead to a safe and healthy
work environment that are effective in practice. WAC 296-800-11035
Develop, supervise, implement, and enforce safety and health training
programs that are effective in practice. WAC 296-800-14020
Back to Top
Photographs and Figures
|
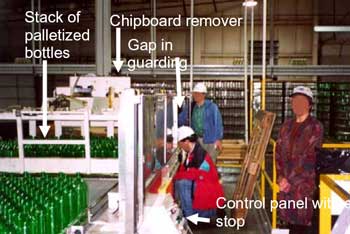
Photo 1. View of depalletizer from operator’s
platform.
|
|
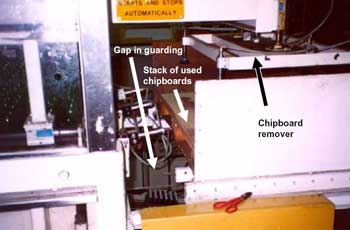
Photo 2. Gap in guarding showing chipboard
remover.
|
|
Photo 3. Bottles and chipboard remover.
|
|
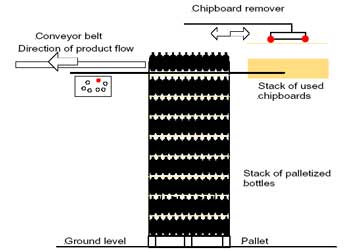
Figure 1. Side view of depalletizing
operation.
|
|
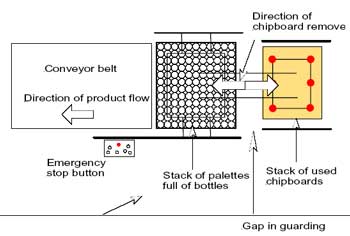
Figure 2. Plan view of depalletizing
operation. |
Back to Top
Washington FACE Program/SHARP
To contact Washington
State FACE program personnel regarding State-based FACE reports, please
use information listed on the Contact Sheet on the NIOSH FACE web site
Please contact In-house
FACE program personnel regarding In-house FACE reports and to gain
assistance when State-FACE program personnel cannot be reached.
|