Fatality Assessment and Control Evaluation (FACE) Program |
|
Car Carrier Truck Driver Dies When Crushed By Ramp of Car Carrier |
| |||||||||||
SummaryOn July 26, 2005, a 59-year-old truck driver (the victim) was fatally crushed while loading used cars onto the auto transport truck carrier. The victim was working alone when he unknowingly activated the hydraulic controls to the ramp for one of the carriers causing it to move forward and downward (Figure 1). The movement caught the victim and pinned and crushed the victim into the hood and windshield of a car positioned on the ramp. Two employees from another auto transport company who were picking up vehicles found the victim pinned under the car carrier ramp. The employees of the other auto transport company contacted the auto auction security personnel who called 911 Emergency Medical Services (EMS) at 4:34 p.m. EMS arrived at the scene at 4:39 p.m. The medical helicopter was contacted at 4:38 p.m. At 4:42 p.m., EMS stated there was no way to attempt resuscitation, so at 4:46 p.m. the request for the helicopter was cancelled. The medical examiner arrived on the scene and the victim was pronounced dead at 5:30 p.m. The FACE investigator concluded that to help prevent similar occurrences, employers should:
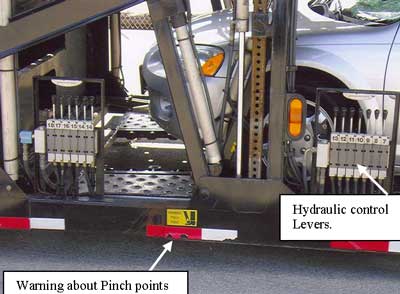
IntroductionOn July 26, 2005, a 59-year-old truck driver (the victim) was fatally crushed while loading used cars onto the auto transport truck carrier. The FACE investigator learned about the incident from the death certificate. The FACE investigator reviewed official reports and sent a letter to the company requesting an interview and followed up with a telephone call to the company. They declined an interview. The content of this report is based on the information from evidence presented in the official reports. The company was a small over-the-road car carrier company that had been hauling cars since 1974. The company purchased the truck and car carrier as one unit. The car carrier was a black Boydstun car carrier manufactured in 2005. The truck involved in the incident was fairly new, a 2005 vehicle with 83,000 miles on it. The company employed five employees, three were truck drivers. The company owned three trucks. The victim was the trainer of new drivers and a driver for the car carrier firm for the past six years. The victim went to the used car auto auction to pick up cars. The victim received initial training on the car carrier, but the company had no formal written procedures in place that governed loading and unloading the car/truck carrier. Back to TopInvestigationThe victim was driving a 2005 Freightliner Classic Series Truck with a 2005 Boydstun car hauler model 9178S. This particular car hauler had a capacity for hauling 10 vehicles. Platform ramps onto which the vehicles were loaded were operated by hydraulic cylinders which were activated from a bank of sectional hydraulic control valves. The lever for each ramp controls movement backward and forward. The control levers are located along the side of the hauler and are attached to the frame of the car carrier. The hydraulic control levers were easily accessible and only protected by steel plate that covered the top of the levers. The car hauler had warning decals attached, “Warning Pinch Points.” When the victim was found, his knee was still pushing two of the hydraulic levers (Figure 2).
At the time of the incident, the victim was checking the tie down chains from the front of one of the ramps. During this activity, the victim came into contact with the hydraulic levers for two of the ramps. This caused the upper ramp to move down, pinching and crushing the victim between the bottom of the ramp and the car located on the bottom belly ramp. The victim worked inside of the car carrier trailer frame when securing cars on the top ramp. Management indicated that employees were trained never to place themselves inside the trailer frame to work unless the racks and ramps were pinned in place. The pinning of the racks and ramps ensured that the ramps and racks were in a secure position and prevented downward movement. According to records, the victim received an updated handbook regarding safety on July 13, 2004. The hydraulic controls had a steel bar installed over the controls as a method of guarding the controls. The manufacturer of the car carrier trailer indicated that the steel bar was over the control levers to prevent a driver from falling onto or contacting the hydraulic control levers in the event that the driver was incapacitated for any reason. The hydraulic control levers were not protected from the inside of the car carrier and inadvertent operation of the levers from the inside was possible. Back to TopCause of DeathThe official cause of death was compression asphyxia. Recommendations/DiscussionRecommendation #1: Ensure that employers utilize retaining pins to prevent unintentional movement or collapses of the ramps when employees are loading cars on the trailers.Discussion: Proper insertion of the pins would prevent downward movement of the ramps or racks on the car hauler trailer. The metal pins were designed and strong enough to withstand the pressures of a loaded car on the ramps and racks.
| ||||||||||||