Fatality Assessment and Control Evaluation (FACE) Program |
|
A County Employee Died When He Was Crushed Between Two Heavy Equipment Compaction Vehicles |
| |||||||||||
SummaryOn May 20, 2004, a 63-year-old heavy equipment operator was crushed between two compaction vehicles in a road construction work zone. Prior to the incident, the decedent and his co-workers were in the process of laying an open stretch of county road and were preparing for the compaction of materials from a chipper and oil dispersion unit. After positioning their compaction units to begin the operation, the decedent and two other compactor drivers dismounted their parked vehicles. While waiting for road oil, the decedent walked between two of the parked compactors in search of a secluded area to use the restroom. While the victim was between the two vehicles, a dump truck was backing up into position. The dump truck driver, who was only using the driver’s side rear view mirror, hit one of the compactors, pushing it into the other compactor and crushing the victim. The parking brake was not functioning on the compactor that was struck. Seeing and hearing the compactors hit, the decedent’s co-workers immediately freed the victim and called for emergency help. The victim was transported to the nearest medical facility where he was pronounced dead on arrival. Oklahoma Fatality Assessment and Control Evaluation (OKFACE) investigators concluded that to help prevent similar occurrences, employers should:
IntroductionOn May 20, 2004, a county employee was crushed between two heavy equipment
compaction vehicles during a road resurfacing project. OKFACE investigators
reviewed the death certificate, Medical Examiner’s report, and Public
Employee Occupational Safety and Health report. An interview with county
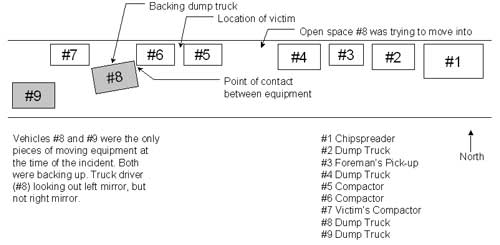
officials was conducted on August 2, 2004. Victim: The 63-year-old male victim had been working for the county in road construction and maintenance for almost 11 years, primarily as a truck driver and heavy equipment operator. On the day of the incident, he was operating a compaction unit, which he had operated many times before. He had been trained on the hazards associated with the equipment and with the work zone in general. The victim was wearing a retro-reflective vest and used ear protection if needed. Training: Safety meetings were conducted at least monthly by the safety officer, and training was provided on-the-job to employees. Trainings covered specific topics as required by state and federal regulations, while other task-specific trainings were conducted as needs arose. Training involved the use of lecture, demonstration, testing, hands-on experience, and videos. Documentation of all trainings and safety meetings was kept on file and maintained by the county. Special training was not required for the operation of the compaction unit. Employees were trained on the hazards of working around heavy equipment and to not enter areas that would place them between pieces of machinery. Written procedure called for the use of a spotter in situations involving the backing of a vehicle in limited spaces with limited site distance. Incident Scene: The incident occurred along a straight stretch of 2-lane rural county road. The road maintenance crew was preparing to begin work and was in the process of positioning vehicles and equipment. One lane was closed for the work zone and was marked with detour signs and channelizing devices. The posted speed limit outside the work zone was 45 miles per hour, with a posted speed limit of 20 miles per hour inside the work zone. The roadway had a line of sight over one mile. Ground conditions were firm and dry. Weather Conditions: On the day of the incident, the weather conditions were excellent. The temperature was in the low 70 degrees Fahrenheit with a clear sky and slight breeze. Back to TopInvestigationOn the day of the incident, the victim had begun work at the site around 7:30 a.m. In preparation for paving, equipment, including dump trucks and compactors (“packers”), was being positioned in the work zone. The victim, an experienced heavy equipment operator, was operating one of the compactors. He and two other compactor drivers had parked their vehicles and were waiting for road oil before continuing their work. They had dismounted their vehicles and were standing in the work zone area. Vehicles and equipment were inspected daily; however, one of the compactors (#6 on Figure 1) did not have a functioning parking brake, yet it remained in service. All three compactors were not running at the time of the incident. While waiting, the victim needed to use the restroom, and since this was a moving operation, there were no restrooms available (although the mobile crew should have had prompt access to nearby facilities as specified by OSHA standards). Attempting to find a secluded area, the decedent walked between the first two compactors (#5 and #6 on Figure 1), blocking his view from co-workers. At the time of the incident, 8:35 a.m., there were two moving vehicles (#8 and #9 on Figure 1) within the work zone. There was no intrusion from outside of the work zone. While the decedent was between the compactors, one of the dump truck drivers attempted to position his dump truck in line by maneuvering in a narrow space around the line of compactors. As the dump truck driver backed into position, only the driver’s side rear-view mirror was used, not the one on the passenger’s side. As a result, the rear end of the dump truck hit one of the compactors, pushing it into the compactor behind it. The dump truck was equipped with a backup alarm, but it was not functioning on the day of the incident. It was later determined that the alarm had been connected to the reverse lights’ electrical wires. When the lights came on, so did the alarm. At the time of the incident, one of the lights was burned out, which disabled the backup alarm as well. Even though the speed of the dump truck was extremely slow, the massive weight of the vehicle and the lack of a set parking brake on the compactor caused the compactor to move. The compactor rolled straight into the other compactor and crushed the victim. The second truck driver (#9 on Figure 1) saw the collision about to occur and tried to radio to the driver to stop, but there was not enough time. Another worker on the ground was yelling for the truck to stop, but the driver did not hear. The truck driver was not aware of making contact with the compactor. Co-workers immediately responded to the pinned victim, with one worker starting and moving the compactor, while another lowered the victim to the ground. Emergency medical services responded and transported the victim to a local hospital where he was pronounced dead on arrival. Cause of DeathThe Medical Examiner’s report listed the cause of death as crushing abdominal trauma.
Back to TopRecommendations/DiscussionRecommendation # 1: Employers should develop and implement written, standardized procedures for backing and maneuvering in work zones, particularly where sight distance is limited, adequate maneuvering space is restricted, or pedestrian traffic is present.Discussion: A written and enforced procedure for maneuvering any vehicle or equipment in a work zone or restricted area is critical to protecting employees and pedestrians. While work zone planning and layout should involve the development of a traffic control plan to ensure the safety of motorists traveling through the work zone, employers should also develop an internal traffic control plan (ITCP). This plan coordinates the flow of construction vehicles and equipment within the work zone area, details safe operating procedures, and ensures the safety of workers on foot and those operating the machinery. Depending on the scope of the project and the length of time at the work site, the ITCP could be a checklist or a complete detailed document. The plan and procedures should detail site-specific hazards and means of control, as well as a communication plan and a means for pedestrian workers to talk with equipment operators. It should also specify that operators be trained to use the equipment they are working with and be oriented to the work site In this incident, an ITCP may have helped improve the movement of heavy equipment through the narrow work zone and provided for a better means of communicating with the truck driver.
| ||||||||||||