Fatality Assessment and Control Evaluation (FACE) Program |
|
Department Store Employee Crushed In a Baling Machine |
| |||||||||||
SummaryOn March 10th, 2004 a 32-year-old male department store employee sustained fatal injuries as a result of being crushed by the hydraulic ram of a cardboard baling machine. On the morning of the incident, the victim was operating the baler in the processing area of the store. At approximately 8:45 a.m., the victim added some cardboard pieces into the baling chamber to start another bale. He did not pull down and shut the safety gate before he pushed the “down” button to start baling. As the ram, a hydraulically-driven flat plate that exerted pressure on the material to be baled, started its down stroke, the victim suddenly climbed on the lower chamber door and extended his entire body into the baling chamber. He was crushed by the ram. Two associates working in the area stopped the baler and called 911. The EMS crew arrived at the site within minutes. The victim was transported to a local hospital where he died later the same day. The post-incident baler examination found that the safety interlock had been bypassed, allowing the machine to operate with the safety gate open. New York State Fatality Assessment and Control Evaluation (NY FACE) investigators concluded that to help prevent similar incidents from occurring in the future, employers should:
Additionally, the baling machine manufacturer should:
IntroductionOn March 10th, 2004, at approximately 8:50 a.m., a 32-year-old male department store employee sustained fatal injuries as a result of being crushed by the hydraulic ram of a baling machine. NY FACE staff learned of the incident on March 11th from a newspaper article. On March 23rd, 2004 a NY FACE investigator conducted an on-site investigation. During the site visit, the NY FACE investigator met with the retail company’s corporate safety director and the store’s operations manager, reviewed the department store’s written safety and health programs and employee training records, and observed the incident site. The baling machine that was involved in the incident was not available for observation at the time of the site visit; the company offered another baling machine that was the same model as the one in the incident for the FACE investigator to observe and photograph. A department store’s surveillance video camera recorded the activities that occurred on the morning of the incident, including the incident itself. The sequence of events leading to this fatality was determined based upon the contents of the videotape. NY FACE staff also received information from the Occupational Safety and Health Administration (OSHA) area office that investigated the fatality. Additional information was obtained from the city police investigator and the medical examiner’s office. The department store that employed the victim is part of a nation-wide retail company. The store employs approximately 500 employees (associates) working in sales, receiving, processing, housekeeping, maintenance, and administrative departments. There was a storewide safety committee that had both management representatives and associates. The committee held monthly meetings and conducted storewide safety inspections twice a month. The company also had a contractor perform periodic safety audits in the store. Reportedly, the audit conducted prior to the incident did not identify any deficiencies in the baler that was involved in the incident. The store safety audit records were not available at the time of this investigation. The store had two baling machines, one in the housekeeping department and the other in the processing department where the victim worked. Both balers were used for baling cardboard boxes for disposal and recycling. According to the store management, four associates, including the victim, were authorized to operate the balers. Baler repair and maintenance were to be done by a contractor. The company’s written lockout/tagout program did not address lockout/tagout issues related to the baler, such as how to clear a jam during normal baler operation. The specific interlock safety feature of the baler and the proper operating procedures for clearing a jam were not discussed during the employee training. The victim had worked for the department store for two years and five months. At the time of the incident, the victim’s job title was Processing Manager and he supervised approximately seven associates. This was the department store’s first fatality. Back to TopInvestigationThe department store was housed in a three-story building consisting of a lower level, the main floor and the second floor. The processing department (Figure 1) was on the second floor. Merchandise (clothing) in cardboard boxes was brought up to the processing department through a freight elevator. The processing associates were responsible for removing the clothing from the boxes, placing sensor pins on the clothing, and hanging them on the racks to be taken onto the store floor. After the merchandise was removed, the cardboard boxes were stacked to be baled. The baling machine in the processing department was identical to the one in the housekeeping department. Both were purchased new in the fall of 2001. The balers were ordered through an equipment dealer and delivered to the store by the manufacturer. At the time of the investigation, the store did not have any records on who received and installed the two pieces of equipment. According to the baler manufacturer, a training videotape and a baler operating manual were delivered along with the balers to the store. However, the store management could not locate the videotape or the training manual at the time of the investigation.
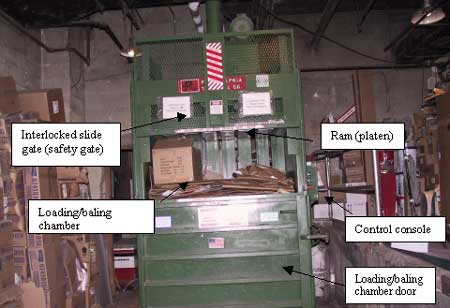
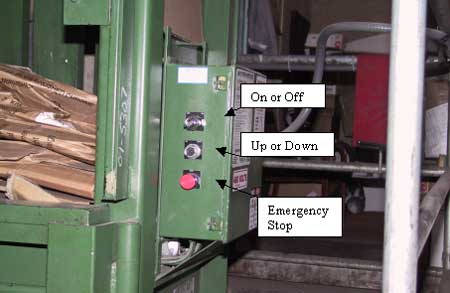
The baling machine was a vertical down-stroke baler (Figure 2), consisting of a ram (platen), an interlocked slide gate (safety gate), a loading/baling chamber, and a control console. The baler utilized hydraulic pressure generated by a 10-horsepower electric motor and a hydraulic pump to compress materials. The completed bales, measuring 60 by 30 by 48 inches, weighed between 850 and 1100 pounds. The control console (Figure 3), located at the right side of the baling machine, had a key switch for turning the machine on or off, a push button for moving the ram up or down, and an emergency stop button. The baler was equipped with safety devices designed to meet the American National Standards Institute’s (ANSI Z245.5) requirements for Baling Equipment-Safety. Specifically, the machine was equipped with a safety proximity switch located in the middle of the lower side of the vertical sliding safety gate. The safety switch was interlocked with the power to the motor and hydraulic pump so that when the gate was fully down and shut, the interlock would engage allowing operating power to the motor and the hydraulic pump. When the door was up and open, the interlock switch cut the power to the motor and the hydraulic pump which immediately stopped the ram from moving.
According to the baler operation video (obtained by the FACE investigator from the baling machine manufacturer during the course of the investigation), a safety check was to be performed before operating the baler. The safety check included lifting the safety gate while the baler was in baling mode. If the baler continued to run when the gate was lifted or the gate was not fully closed, the operator was to discontinue operating the baler and have the safety switches repaired or replaced immediately. However, the written baler operation manual did not address the safety check. It instructed the operator not to operate the baler unless the gate was fully closed, and not to attempt to defeat or override the safety switch or interlock. The victim and three other associates were authorized by the store to operate the balers. The employer required that operators wear safety goggles when operating the balers. The victim reportedly ran the baler approximately three to four times a day, for 30 minutes each time. Store management did not have any records of dates and methods for training authorized employees on operation of the balers. According to the post-incident investigation, none of the three authorized operators knew about the function of the safety interlock. According to the OSHA investigation, numerous store associates had witnessed the baler compacting with the safety gate open. An OSHA compliance officer observed a broken key in the baler’s “On or Off” key switch on the day of the incident. A post-incident baler examination found that the electrical wiring had been altered to bypass the “On or Off” switch, and the gate safety switch had been short-circuited by a piece of two-inch wire. By doing so, power was always supplied to the machine and the baler could operate with the safety gate up. It could not be determined during this evaluation who modified the baler’s electrical circuit, when these alterations were made, and what the intent was.
On the morning of the incident, the victim and another associate arrived at work at 5:30 a.m. to set up and prepare for receiving and processing merchandise for the day. The other workers came in around 7:30 a.m. At the time of the incident, there were five associates working in the processing area. At approximately 8:45 a.m., the victim ejected a completed bale from the baling chamber. After he wheeled the bale away on a pallet, he returned to the baler and shut the baling chamber door. He picked up a few cardboard pieces and dropped them into the baling chamber to start another bale. The victim then pushed the “Down” button and the ram started coming down. During all of this, the safety gate was up. While the ram continued its down stroke, the victim suddenly climbed on the chamber door and put his entire body into the baling chamber. He was crushed by the ram. Two female workers in the area heard the victim and ran to the baler to help. They pushed the emergency stop button to stop the machine and called 911. An emergency medical service crew was dispatched and arrived within minutes. The victim was transported to a local hospital where he died later the same day. The reason that the victim climbed into the baler could not be determined from the videotape or other information obtained during the investigation. Back to TopCause of DeathThe cause of death as listed by the Medical Examiner as blunt force injuries to the torso with a crushed liver, lacerations of large vessels, and hemorrhage. Recommendations/DiscussionRecommendation #1: Employers should inspect all baling and compacting machines periodically to ensure that all safety features are functioning properly.Discussion: Although the company conducted storewide safety inspections twice a month, the inspections did not identify the bypassed safety devices on the baling machine. The safety switches and interlocks on baling machines are designed to protect operators from being injured by the movement of the ram. Bypassing these safety devices increases the potential risk for severe injuries such as crushing or amputation, and in this case, resulted in a fatality. To help ensure operator safety, employers should inspect all baling and compacting machines periodically to ensure safety features are working properly. A baler inspection checklist with specific instructions on how to perform safety device checks should be developed. The results of each inspection should be documented and the records maintained. Balers with malfunctioning safety devices should be removed from service immediately until repairs are completed.
| ||||||||||||