Fatality Assessment and Control Evaluation (FACE) Program |
|
Maintenance Supervisor Crushed Under a Falling Gantry Crane |
| ||||||||||||
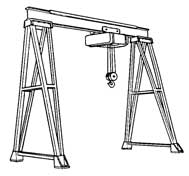
SummaryOn August 24, 2004, a 67-year-old male maintenance supervisor was killed when a small gantry crane fell over as it was being moved with a forklift truck. The incident occurred at a plant that manufactured industrial electrical transformers. The plant used a number of gantry cranes for moving heavy materials. This crane was comprised of a horizontal steel I-beam mounted on two vertical A-frame supports bolted to the concrete floor. A maintenance crew was assigned to move the 10-foot-high, 28-foot-long, 1,058-pound crane a short distance to a new location. The crew unbolted the crane and set one end on a wheeled dolly. A forklift truck supported the opposite end. The victim had planned to control the dolly as the forklift pushed the crane. As the forklift truck started to move, the top-heavy crane toppled over, striking the victim who apparently tried to stop its fall. NJ FACE investigators recommend following these safety guidelines to prevent similar incidents:
IntroductionOn August 25, 2004, NJ FACE staff received a newspaper article about a factory worker who was killed after being struck by a steel beam. A NJ FACE investigator conferred with the investigating OSHA Compliance Officer and arranged to conduct a concurrent investigation. On August 30, 2004, FACE investigators viewed and photographed the incident site and the equipment involved. Investigators also interviewed two coworkers who witnessed the incident. Additional information was obtained from the police report, the medical examiner’s report, and the OSHA investigation file. The victim’s employer was a company that manufactured large industrial electrical transformers (SIC 3612, NAICS 335331). The company had been in business since 1918, and had been at this location since 1979. The company employed 120 non-union workers, 95 of whom were working at the time of the incident. Company training was mostly on-the-job, supplemented with classroom training on hazard communication and safety. Safety infractions and incidents were discussed in quarterly meetings, and management conducted a monthly safety inspection. Safety issues were also discussed during the plant’s weekly supervisors meeting. The victim was a 67-year-old white male maintenance supervisor who had worked for the company for 32 years. He reportedly had 20 years of experience with a roller bearing company before this job. He was survived by his wife and two children. Back to TopInvestigationThe victim’s employer was a large electrical transformer manufacturing company. The company was housed in a 75,000 square-foot, single-story industrial building located in a suburban industrial area. The industrial transformers were individually manufactured to order, and ranged in size from “utility pole” transformers to much larger transformers that weighed thousands of pounds. These transformers were generally made by first making a steel “core” out of steel plates. Electrical wires were wrapped around the core to create the primary winding, which is the winding first energized by electricity. A secondary winding of wire was also wrapped around the steel core, next to the primary winding. The electromagnetic field created by the primary winding travels along the core and induces an electrical current in the secondary winding. This induced voltage is determined by the ratio of the number of wire wraps of the two windings. Once the transformer is made, the core and windings may be sealed with a coating and baked in a curing oven. It is then mounted in a heavy metal case, which may be filled with oil to help cool the unit. The completed transformer is then tested before being shipped to the customer.
Much of the work at the plant was done manually, including the handling and stacking of hundreds of steel plates to make the cores. Due to the weight of the materials and products, the plant utilized a number of small gantry cranes to move these materials at the workstations. The gantry crane involved in the incident was made up of an electric hoist that moved along the length of a horizontal steel I-beam. Steel posts supported the ends of the I-beam, with each post terminating in an A-frame mounting that was secured to the concrete floor. The crane used an electric hoist with a 1,000-pound rating that was operated with a pendulum controller. The cranes dimensions were 10 feet high by 28 feet long, with a 62-inch base. The OSHA Compliance Officer calculated that the crane weighted 1,058 pounds, and the hoist weighted 150 pounds. Plant management decided to move this crane about 40 feet to a new location in the plant and assigned the task to the victim, the plant’s maintenance supervisor. The day before the incident, the victim discussed with management where to place the crane, concerned about its proximity to an electrical bus bar. After solving this problem, the victim and another worker disassembled a smaller version of the same type of crane. This took them approximately 4.5 hours to complete, and the crane was removed from the building and stored outside. Reportedly, one of the victim’s two-person maintenance staff was on vacation, and the victim was concerned about moving the larger crane without his full staff. He spoke to the company human resources officer, who told him to see a manager and not to do the job if he felt it was unsafe, but the victim reportedly did not express any further concern. The incident occurred on Tuesday, August 24, 2004. After arriving for work in the morning, the victim met with his maintenance worker, who was to operate the forklift truck. A young laborer who had worked at the plant for six weeks was assigned to assist them. Under the victim’s direction, they planned to move the crane with a forklift and a wheeled dolly. First, they secured the 150-pound hoist with beam clamps to prevent it from moving on the I-beam. After unbolting the crane from the floor, they used a small, walk-behind forklift to raise one end of the crane. This was done by positioning the forks between the crane’s A-frame, using pieces of 4-by-4 inch wood blocks (cribbing) to fill the space between the forks and the frame. Once raised, the frame was lowered onto an industrial wheeled dolly, and the forklift was removed. The crew then took the forklift to the other end of the crane, planning to lift it in the same manner. As the crew was placing the cribbing into the crane’s A-frame, the plant’s safety manager stopped the operation to make a correction to the blocks in order to make them more stable. The crew immediately made the change, and lifted the end of the crane up about five inches with the forklift. At 10:20 a.m., the forklift (which was positioned in the inside of the crane under the horizontal beam) was moved forward, and the victim and laborer stood at either side of the A-frame supported by the dolly. As the forklift slowly started to make a turn to the left, the crane became unbalanced on the forks and started to tip to the right. The victim moved in and tried to grab the steel support at his end, apparently in an attempt to right the crane or to keep it from striking the laborer who was helping him. His effort failed, and the crane continued to topple over, striking the victim across his back. The other two workers were under the falling crane, which passed over their heads as it fell. The laborer received minor injuries when the crane caught and ripped his pants, the forklift operator was not injured. The production supervisor and several other employees went to the victim, who was pinned in a squatting position under the frame of the crane. They manually lifted the crane off the victim, who was unconscious. They placed him on the floor as another employee came over to give first aid. The production supervisor gave an order to call 911, and to get the first aid kit, oxygen unit, and automatic external defibrillator (AED). CPR was started after they lost his pulse. EMS arrived and transported the victim to the local hospital where he was pronounced dead at 11:01 a.m.
OSHA immediately dispatched a compliance officer to investigate after the police notified them of the incident. The company stopped operations for a day, and crisis counselors were called in for the next two days to talk with the employees. Back to TopRecommendations/DiscussionRecommendation #1: Employers should service cranes and other equipment as per manufacturers’ directions.Discussion: In this case, it appears that a number of improvisations and shortcuts were used to move this crane. These include not disassembling the unit, not removing the hoist, and using the forklift and dolly to move the crane in one piece. NJ FACE recommends following the manufacturers instructions for safely servicing and moving the cranes. If the directions are not available or clear, the manufacturer should be called for advice. Following the incident, the company developed and implemented a procedure for moving heavy production equipment. This procedure included examining and planning unusual jobs, and obtaining a contractor if a safe method for moving equipment could not be done in-house.
| |||||||||||||
 |