Fatality Assessment and Control Evaluation (FACE) Program |
|
Construction Worker Struck by Falling Steel Roof Beam |
| |||||||||||
SummaryA 41-year-old male construction laborer was killed when he was struck by a falling steel roof beam. The victim was helping two others use a forklift to move single-piece steel roof beams to a staging area, then attaching x-bracing to join two beams together for future placement onto a new gymnasium. The forklift operator was lowering the steel roof beam to the ground when the victim darted underneath the corner of the beam being lowered. The beam slipped off of the forklift tines and struck the victim in the head. The victim’s co-workers and other site personnel called emergency personnel, who responded within a few minutes. The victim was transported to a nearby hospital where he was pronounced dead. The Nebraska Workforce Development, Department of Labor’s Investigator concluded that to help prevent future similar occurrences, employers should:
Program ObjectiveThe goal of the Fatality Assessment and Control Evaluation (FACE) workplace investigation is to prevent future work-related deaths or injuries, by a study of the working environment, the worker, the task the worker was performing, the tools the worker was using, and the role of management in controlling how these factors interact. This report is generated and distributed solely for the purpose of providing current, relevant education to employers, their employees and the community on methods to prevent occupational fatalities and injuries. IntroductionOn June 15, 2005, at approximately 1:45 p.m., a 41-year-old male construction laborer died after being struck in the head and back by a steel roof beam that fell from a forklift’s tines. The Nebraska Department of Labor was notified of the fatality the same day by the County Sheriff’s office. The Nebraska FACE Investigator met with the investigating OSHA Compliance Officer (COSHA) and the victim’s management, lawyers and insurance personnel on June 16 & 17, 2005 at the mishap location. The victim’s employer builds commercial facilities, such as concrete buildings, gymnasiums, auditoriums, etc. The company has been in business since 1982. At the time of the accident the company employed 20 employees including the victim. The company operated at three locations. The company did not have a written safety program. Training given to employees normally consisted of weekly “tailgate talks”. The employer had no previous history of fatalities. Back to TopInvestigationPersonnel: Victim: The victim was a 41-year-old male. He had been employed by this company for 3 years, and previously with another construction company for 10 years as a carpenter. Worker #2: He worked for the company for approximately 13 years, mostly as a mason. He had received some formal safety training to include forklift operation through a previous employer, but none through this current employer, but no documentation was provided to the investigator. Forklift Operator (FO): The operator was also a co-owner of the company and the “General Superintendent”. Wet weather had delayed construction and he was acting as the job superintendent for this project. He was involved in construction since 1962, and operating forklifts of various types since 1965. In 1982 he helped form the current company. He had not received any formal forklift training or certification. Training: The company did not have a completed safety & health program, although they started drafting one approximately 3 months before the incident. Employees were trained “on-the-job” for their various duties. Weekly “tailgate talks” were held covering different appropriate topics. No formal forklift training had been conducted for any of the employees, although several operated forklifts during the course of their daily duties. Equipment: Forklift: The forklift used at the time of the incident was a CAT 920 loader. It has been owned by the company for more than 15 years. It was equipped with a Balderson fork attachment that was manufactured for CAT equipment. Each forklift tine was rated with a lifting capacity of 10,000 pounds by the manufacturer. Each tine has had a hole “burned” through them with a cutting torch towards the end of the tine. It was not known when this occurred but it was after the company purchased the forklift. The manufacturer was not contacted to gain permission for this alteration. There were no known mechanical defects at the time of the accident that may have contributed to the mishap. Beam: Each steel beam was 84 feet long and 44 inches tall in the middle, tapering off slightly towards the ends. They were shipped to the construction site three beams to a bundle. Each bundle weighed 4.96 tons (9,920 pounds). After unloading, the bundles were broken down to single beams which weighed 1.65 tons (3,306 pounds) each. Each single beam would be moved to a staging area where it was paired up with another similar beam and joined together with steel x-bracing material, to await erection. Back to TopAnalysis/SynopsisThe day before the incident, the victim and FO worked together moving and joining together six single steel roof beams. The FO picked up a single beam at the northwest corner of the construction site, backed up and turned around, then proceed approximately 300 feet to the northeast corner of the site. The victim would walk beside and slightly behind the beam, ensuring there were no obstacles in their path. Upon arrival at the assembly area, the beam was lowered to the ground, but still held upright on the forklift’s tines. The victim would have previously placed a single piece of wooden 4x4 where the north end of the beam was to be set, and two pieces of 4x4 on top of one another on the south end, approximately three feet from the end of the beam. The two pieces on top of one another were necessary due to a slight drop in the ground’s contour on the south side of the construction site. Two pieces of wooden 2x4s were placed at approximately the center point of the beam to brace it upright until the next beam was delivered. Once the first beam was supported by the 2x4s, the FO and victim got another beam and repeat the path of travel. The second beam was lowered onto the 4x4s and steel x-bracing was attached between both beams to secure them together. Three sets of two beams each were put together. On the morning of the incident, the FO, victim and worker #2 started work at approximately 6:15 a.m., working mainly with concrete being poured. At approximately 12:00, just prior to lunch break, the victim and worker #2 took some of the wooden 4x4s to the beam assembly area to position them for the next steel beam. Worker #2 placed the north 4x4 down, and then went to the south side. The victim laid a 4x4 down, and worker #2 placed another 4x4 on top of that it. After lunch the victim, worker #2 and the FO started to move another beam, but had to wait several minutes while a truck containing cement blocks was off-loaded on the side of their path of travel. Once the truck departed, the FO placed the tines under the beam, raised it off the ground, backed up, and proceeded towards the assembly area. Both the victim and worker #2 were walking slightly behind and opposite sides of the beam. As they approached the pile of cement blocks, the FO realized the beam would not clear them. He raised the beam as high as he could, but the bottom of the beam was not high enough to clear the blocks. The victim and worker #2 removed the top layer of blocks. This allowed the beam to clear the blocks. After passing the blocks, the FO lowered the beam so the bottom was approximately 4’ above the ground and proceeded to the assembly area. The FO pulled into position for lowering the beam and stopped. He looked both left (worker #2’s direction) and right (victim’s direction), saw that both men were clear (still a few feet behind and to the side), and proceeded to start lowering the beam. When the bottom of the beam was approximately three feet off the ground, the FO saw the victim start to dart under the end of the beam. At this same instant, he saw the beam slip off the end of the tines. Both he and worker #2 yelled “Look out”. The victim was in a crouched position, and the beam struck him in the head and back. The beam then struck the adjacent set of beams and fell over backwards. Worker #2 ran to the victim while the FO exited the forklift. Other workers nearby heard the noise and ran to the scene to assist. 911 was called and local emergency responders were at the site within minutes. Although the victim was not trapped between the two beams, several employees lifted the single beam and slid it approximately one foot away from the victim to allow easier access for emergency personnel. The victim was transported to a nearby hospital where he was declared dead. Back to TopConclusionIt will never be known why the victim darted under the beam. The victim
was known as a It also is not known why the beam slipped/fell from the forklift tines. The FO stated that he did not remember tilting the forks for any reason after clearing the cement blocks. Several days after the accident the investigating COSHA witnessed the operation of the forklift performing the same lift that was involved during the accident. There were no apparent mechanical defects noted on the forklift at that time. Cause of DeathAccording to the death certificate, the cause of death was: Massive head injury due to, or as a consequence of falling metal beam. Back to TopRecommendations/DiscussionRecommendation #1: Use a crane to lift loads that cannot be safely lifted with a forklift.Discussion: Before moving the beams from their storage location to the beam assembly area , many factors such as their weight, length, terrain, etc. must be taken into consideration to ensure a safe operation. If any single factor or combination thereof may deem the move unsafe, then another alternative method must be used, i.e. a crane, larger forklift with a wider span between the tines, etc.
| ||||||||||||
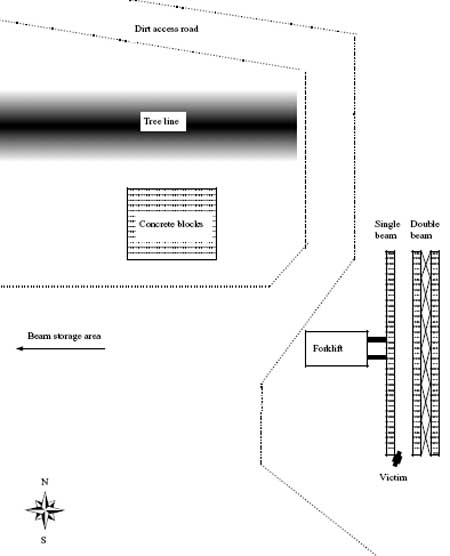 |
Attachment 1. Site diagram
(Diagram not to scale) |
 |
Attachment 2. Picture
of incident steel roof beam showing victim’s position and
location of 4x4s. |
This picture was taken the day after the incident looking north. This is the single beam that fell from the forklift tines. The black oval indicates the approximate location of the victim’s body after being struck by the beam, which was in a crouched position. The black arrow points to the two 4x4s that this end of the beam was to rest on. It is believed that the top 4x4 was not centered properly and the victim darted underneath the raised beam end to align the boards. The victim was struck by the beam, but was not trapped between the single beam and the paired beam to the right.
 |
Attachment 3. Incident forklift
showing forks in maximum raised position next to concrete block
pile. |
 |
Attachment 4. Incident forklift
tines with arrows indicating holes cut into them. |
To contact Nebraska
State FACE program personnel regarding State-based FACE reports, please
use information listed on the Contact Sheet on the NIOSH FACE web site
Please contact In-house
FACE program personnel regarding In-house FACE reports and to gain
assistance when State-FACE program personnel cannot be reached.
