Fatality Assessment and Control Evaluation (FACE) Program |
|
Laborer Died After 2000-pound Flexible Tote Bag Falls on Him |
| |||||||||||||||
Summary
Recommendations:
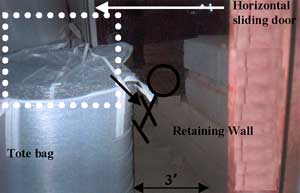
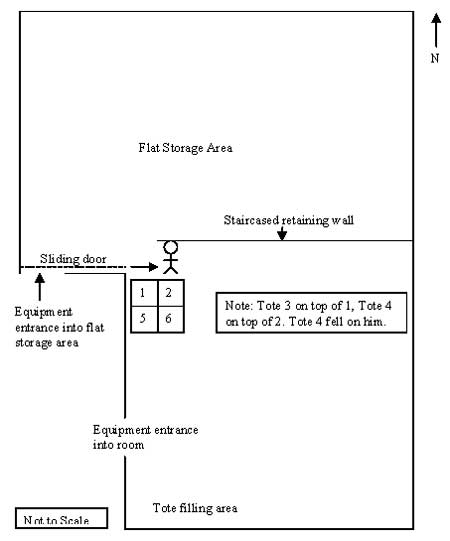
IntroductionOn November 11, 2003, a 60-year-old general laborer who worked at a grain elevator was suffocated when a 2,000-pound bag containing split black beans fell on him. On November 12, 2003, the Michigan Occupational Safety and Health Administration personnel who had received a report on their 24-hour-a-day hotline that a work-related fatal injury had occurred on November 11, 2003, notified MIFACE investigators of the fatality. MIFACE interviewed the health and safety manager for the company owning the facility by telephone on August 9, 2004. MIFACE conducted a site visit on August 27, 2004 and interviewed the manager of the grain elevator at the site. Both described the events on the day of the fatality. The facility manager accompanied the researcher to the grain elevator facility to observe the tote bag filling, transporting and storing operations and to visit the site of the fatality. During the writing of the report, the medical examiner's report, the police report and photographs, and the MIOSHA file and citations were reviewed. Police pictures taken at the scene are Figures 1, 2, 3. To protect confidentiality, Figure 1 has been altered by MIFACE so as not to show the deceased’s body. A member of the MIFACE Advisory Board provided the picture used in Figure 6. The grain elevator where the victim worked employed four people. The company traded and processed edible, whole beans and made split beans as a byproduct. The victim had worked for this company approximately 18 years, but had processed beans at another facility for one year, thus giving him 19 years of work experience processing beans. He was a full-time, hourly employee. His job title was general laborer. Company employees usually worked 8-hour days except during harvest season, when extended work hours were common. His shift started at approximately 8:00 a.m. and ended at 4:30 p.m. The grain elevator has a written Health & Safety Program. The facility manager discusses health and safety topics with the employees using a leader guide at mandatory employee attended monthly safety meetings. An outside consultant supplies the health and safety training topics, the leader guide and the material and handouts given to the employees. To ensure understanding, employees are tested on the material covered in the health and safety training sessions. Correct answers are given and the reasoning for the correct answers discussed in a question and answer session directly following the testing. The facility manager is required to document and report to the parent company the attendance of the individuals at the training sessions. The grain elevator is audited every two years by the parent company to ensure their compliance with company policy for training documentation as well as conducting safety and health training. At the time of the incident, the grain elevator did not have a specific procedure in their Health and Safety Program for filling and stacking bean totes. The MIOSHA investigation resulted in one serious violation being issued to the grain elevator: General Provisions, Part 1, Rule 15(1) addressed the hazard presented by the unstable stacking of the tote bags. Back to TopInvestigationThe flexible, duffle-top style polyethylene tote bags were approximately 4’ x 4’ x 4’ when filled with product. The tote bags had safety warning labels that indicated how to carry the bags but did not have information concerning how full to fill the bags, how to secure the opening top of the bags, or how to stack the filled bags. The MIFACE researcher observed the tote bag filling, transport, and storage process. At the time the MIFACE researcher was observing, the tote bags were being stored in a single layer, not double-stacked. A worker placed an empty tote bag on a scale under a spout where product was dispensed into the tote bag from a grain elevator. The tote bag was filled to a pre-determined weight. After the tote bag was filled, the operator would gather the bag’s duffle material at the top of the bag and tie it closed. Then he lifted the tote bag by its handles as directed by the manufacturer from the scale using a forklift. This procedure helped to flatten out the base of the bag so that it would sit “squarely” on the floor. The tote bag was then transported to a storage area. The forklift operator ensured that each filled tote bag was placed so it was in direct contact with a previously placed tote bag. The MIFACE researcher observed that the newly placed tote bag contents shifted toward the tote bag it was being placed next to as it was being placed in direct contact with the previously placed tote bag. The MIFACE researcher also observed that there was a slight tilt to all of the totes bags on the floor in the direction of transport movement after being placed on the floor. The totes involved in this incident were stacked one on top of the other in two rows as shown in Figure 2. Although no written procedure existed, double-stacking the tote bags was accomplished in the following manner: tote bag 1 was placed in position, tote bag 2 was set next to tote bag 1, tote bag 3 was placed directly on top of tote bag 1, tote bag 4 was placed directly on top of tote bag 2, tote bag 5 was placed against the wall and “snugly” against tote bag 1, tote bag 6 was placed snugly against tote bag 2, tote bag 7 was placed on top of tote bag 5, etc. Tote bag 4 was the tote bag that fell on the deceased.
The victim had followed the above procedure when he stacked the tote bags involved in the incident. Based on police pictures taken at the scene, the bags were filled above the seam where the handles were sewn. The tote bags were not secured in position nor were they secured or tied at the top to prevent the beans from falling out of the bag. See Figure 3.
On the day of the incident, the deceased had been filling totes with split black beans. The facility manager indicated that split beans are “bulkier” compared to whole beans and thus take up more space in the tote bag. Two thousand pounds of split beans in the tote bag filled the bag to a higher level than an equivalent weight of whole beans. The tote bags the victim had filled contained approximately 2,000 pounds of split beans. The victim placed the odd-numbered tote bags against the west wall of the room where he was filling the tote bags. There was a discrepancy concerning when the bean tote bags had been filled. One interviewee stated that the victim had filled and stacked the totes three to four days prior to the incident, and another interviewee stated that the victim had filled and stacked the totes the day of the incident. The victim did not tie the tote bags shut. See Figure 4 at the end of this report for a schematic drawing of the victim’s work area. On the north side of the bean tote bags was a three-foot wide passageway. On the north side of the passageway was a retaining wall that was located in an area called the flat storage warehouse. The retaining wall had been used to separate the tote-filling area from the flat storage area. The retaining wall construction was “staircased.” The lowest level of the retaining wall was approximately 25” tall. The second “stair” was set back from the first and was 48” tall.
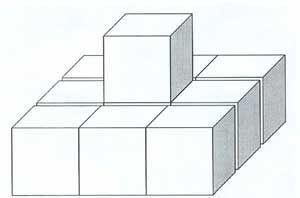
A 13’10” horizontal sliding bay door provided entry for both mobile equipment and company personnel into the flat storage warehouse from outside the building. It is thought that the victim walked around the stacked tote bags to access the sliding door via the passageway between the totes and the retaining wall. To assist in moving the sliding door along its track, a squeeze-type vice-grip “C” clamp was attached to the door. Due to a previous farming injury, the victim was missing his right hand. It appears that he had grasped the “C” clamp with his left hand, and with his back to the tote bags, was in the process of opening the sliding door to allow a piece of mobile equipment to enter the flat storage warehouse when the tote bag began to tip and beans began to spill out of the bag. The beans would have started to spill out of the tote bag slowly, but because his back was toward the totes, he was apparently unaware of the problem. The facility manager stated that the victim did not have a hearing problem that could have affected his ability to hear beans falling on the ground. Because the beans continued to spill out of the tote bag, the bag’s center of gravity shifted causing the tote bag to fall. The tote bag fell on top of him, striking him in the back and pinning him against the retaining wall. He was found on the lower level of the retaining wall near the second level with his head against the rise to the second level at approximately the location of the tote bag #4. A co-worker found the victim after looking for him because he had not been seen all morning. The co-worker ran to the manager’s office. The manager called 9-1-1 and went to the location of the victim. As he was removing beans from the victim, the co-worker who found the victim used a forklift to the raise the tote from the victim’s back. Approximately one-half of the product was left in the bag. There were many factors that may have played a role in this fatality. These factors include overfilling of the tote bags, not tying the tote bags closed, double-stacking of the tote bags without supporting the outside edges, the victim using an unauthorized passageway to travel from one area to another, and the victim pulling the door closed with his back to the tote bags instead of facing them. After the incident the company addressed these factors by developing a tote bag filling and stacking policy and constructing a permanent wall separating the bean tote bag filling/storage area and the flat storage area. The company has developed a written standard operating procedure stating that tote bags are not to be filled above the level of the uppermost seam and that the tote bags must be tied shut. The preferred method of tote bags storage is in single rows placed on the floor in storage areas. If double-stacking is necessary, there must be a single tote bag perimeter around the double-stacked tote bags. This policy was in effect at the time of the MIFACE visit. See Figure 5 for an example of the new tote bag stacking procedure. To eliminate the possibility of employees walking between the tote bags and the retaining wall, the company built a permanent wall to separate the area where the tote bags are filled and stored from the flat storage area.
Back to TopCause of DeathThe cause of death as stated on the death certificate was suffocation. No alcohol or drugs of abuse were found in the victim’s blood or urine. Recommendations/DiscussionEmployers should ensure that flexible storage container filling, stacking and storage are performed in a manner that minimizes the possibility of containers falling.Unstable stacking of the tote bags was a major factor in this incident. Overfilling of the tote bags caused the bags to be “rounded” on the top and did not allow for the tote bags placed on top of them to sit “flat.” Double stacking requires that the bottom tote bag provide a sturdy foundation for the tote bag placed on top of it. The lack of a stable foundation caused the tote bags that were double-stacked to be misaligned on the tote bags they were stacked upon. Complicating the stacking issue was fact that the tote bags were not tied shut and thus beans could escape from the double-stacked tote bags and cause the tote bags to tip when placed on an uneven surface. The double-stacked tote bags were in open storage, unsecured, and could fall on employees. As stated previously, the company has developed and implemented a new standard operating procedure to address the hazards of untied totes and unstable stacking. An alternate storage method that would also be acceptable is to place totes on pallets in storage racks and stabilize/secure the sides of the tote bags to prevent tipping. Stabilizing or securing could be accomplished by strapping, wrapping in plastic, or other effective means. Figure 6 is an example of plastic-wrapped double-stacked tote bags on pallets that were shipped to and received at a greenhouse. The greenhouse stores the bags in their warehouse in the wrapped, double-stacked condition until required for use in their operation.
Identify and appropriately mark aisle ways and passageways and require employees moving from one work area to another use these marked aisle ways and passageways.MIOSHA Part 1, General Provisions defines an aisle as a designed path of travel for mobile equipment and employees. Aisle clearances shall be provided and maintained to assure safe passage for the equipment and the employee. MIOSHA does not specify how wide an aisle must be to assure safe passage except in two instances, Part 6 and Part 75. MIOSHA Part 6, Fire Exits specify that emergency exit access must be at least 28 inches wide. MIOSHA Part 75, Flammable and Combustible Liquids specifies that in every inside storage room containing flammable and combustible liquids there shall be maintained one clear aisle at least three feet wide. A passageway is defined as a path of travel for an employee only. MIOSHA requires that both aisles and passageways be marked or otherwise identified. When totes were filled in the area where the victim was working, they were routinely stacked and stored in the same location. Two options existed for opening the sliding door: exiting the building or using the passageway between the totes and the retaining wall. Employees routinely used this passageway to open the door instead of going outside. This passageway was not marked as a passageway, and due to the location of the tote bags, should not have been used as a passageway. MIFACE recommends that companies survey their facilities to identify employee paths of travel and to appropriately mark the paths. Employers should require employees to use the “approved” paths of travel and not “short-cuts.” Back to TopReferencesMIOSHA Standards cited in this report can be directly accessed from the Michigan Department of Labor and Economic Growth, MIOSHA web site http://www.michigan.gov/dleg/0,1607,7-154-11407_15368---,00.html (Link updated 12/11/2007). The Standards can also be obtained for a fee by writing to the following address: Michigan Department of Labor and Economic Growth, MIOSHA, MIOSHA Standards Section, P.O. Box 30643, Lansing, Michigan, 48909-8143. MIOSHA Standard Section phone number is (517) 322-1845. MIOSHA General Industry Safety Standard, Part 1. General Provisions MIOSHA General Industry Safety Standard, Part 6. Fire Exits MIOSHA General Industry Safety Standard, Part 75. Flammable and Combustible Liquids (Federal Revocations) Michigan FACE ProgramMIFACE (Michigan Fatality Assessment and Control Evaluation), Michigan State University (MSU) Occupational & Environmental Medicine, 117 West Fee Hall, East Lansing, Michigan 48824-1315. This information is for educational purposes only. This MIFACE report becomes public property upon publication and may be printed verbatim with credit to MSU. Reprinting cannot be used to endorse or advertise a commercial product or company. All rights reserved. MSU is an affirmative-action, equal opportunity employer. 4/13/05 MIFACE Investigation Report # 03MI160 Evaluation (see page 9 of report) To contact Michigan State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
| ||||||||||||||||