Investigation: # 03MI018
Manager of After-Market Truck Bed Liner Store Dies of Asthmatic Attack after Spraying Van with Isocyanate-based Truck Bed Liner
|
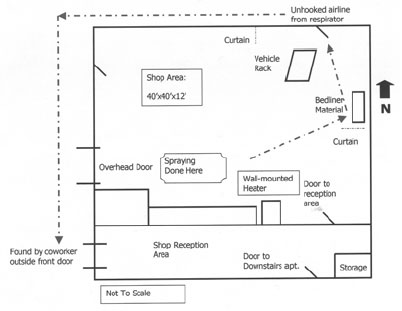
| Figure 1. Exit Route of Victim. |
RECOMMENDATIONS
When spraying isocyanate-containing material, employers should:
INTRODUCTION
On February 20, 2003, a 45-year-old vehicle detailing company manager died after spraying an isocyanate-based truck bed liner inside a van. On February 21, 2003, MIFACE investigators were notified of the fatality by a call from the county medical examiner. On February 27, 2003, MIFACE was informed by the Michigan Occupational Safety and Health Act (MIOSHA) personnel, who had received a report on their 24 hour-a-day hotline, that a work-related fatal injury had occurred on February 20, 2003. On May 23, 2003, the MIFACE researcher interviewed the owner of the vehicle detailing company at his primary business location. The company owner and MIFACE researcher traveled to the site of the closed vehicle detailing facility. At this time, the MIFACE researcher was able to obtain the Material Safety Data Sheets for the components of the isocyanate-based truck bed liner, take pictures of the facility and of the types of personal protective equipment the victim wore during application of the spray-on liner. During the course of writing the report, the autopsy results, death certificate, MSDSs, and the MIOSHA citations were obtained. Figure 5 and Figure 7 are pictures taken by the MIOSHA compliance officer at the time of the MIOSHA investigation of the fatal incident. To preserve anonymity, MIFACE removed the company’s name from the wall in Figure 5.
MIFACE visited two additional companies as part of the incident investigation to learn about the process of spray-on truck bed liners and to compare work practices. These companies are identified as Company A and Company B in the Discussion/Recommendation section.
The company was issued 6 alleged serious citations and 5 alleged other citations. Four serious citations issued to the company concerned Part 451, Respiratory Protection; the company was cited for failure to: (1) develop and implement a written respiratory protection program with worksite-specific procedures for employees who are required to wear respiratory protection, (2) provide a medical evaluation that follow procedures outlined in subsections (e)(2) through (e)(7) of 1910.134, (3) provide an employee fit test using an OSHA accepted QLFT or QNFT protocol which is contained in Appendix A of 1910.134, and (4) provide and document employee training regarding respiratory protection prior to using a respirator in the workplace. An alleged serious citation was also issued regarding Hazard Communication, Part 430, for failure to develop, implement and maintain a hazard communication program. An alleged serious citation was issued regarding Medical Services and First Aid, Part 472, for failure to provide suitable facility for quick flushing of the eyes within the work area for immediate emergency use where the eyes of an employee may be exposed to injurious corrosive materials. MIOSHA issued the following “Other” citations: The employer did not report orally or in writing to the Department of Consumer and Industry Services within 8 hours after the occurrence of an employment accident or illness which was fatal to 1 or more employees (Michigan Occupational Safety and Health Act, Act 154, Public Acts of 1974, as amended, Sec. 61(1), the employer did not post the Michigan Occupational Safety and Health Act (MIOSHA) Notice poster in each establishment in a central and conspicuous location (Inspections and Investigations, Citations and Proposed Penalties, Part 13, Rule 1311(1), the employer did not provide spray booths or spray rooms to enclose or confine all spray finishing operations (Spray Finishing Operations, Part 528, Rule 3235(3). The employer received two Other citations for violations of the Personal Protective Equipment, Part 433; (1) the employer did not verify through a written certification that a workplace hazard assessment had been conducted and (2) the employer did not verify that each affected employee had received and understood the required training through a written certification that contained all of the following information: the name of each employee trained, the date of training and the subject of certification.
The company owner had purchased the building and the detailing business a little over a year prior to the incident. The company performed vehicle detailing, applied rustproofing and spray-on truck bed liners. The owner had purchased the franchise rights to apply this spray-on truck bed liner product. The victim was hired as the shop supervisor approximately one year prior to his death. The victim had worked at the detailing business for approximately 11 months as manager of the shop. There were a total of four employees on site; a receptionist who worked in the customer reception area, the victim, and two other employee who performed other prep work for the spray-on liner application as well as other accessorizing activities. The employer did not have a written safety program. The employee had received training concerning application of the spray-on liner by the manufacturer of the truck bed liner; the owner did not know if the training included the health and safety aspects related to the isocyanate component of the liner. The company did have the material safety data sheets (MSDSs) for the two-part bedliner product, polyol and isocyanate.
INVESTIGATION
Spray-on polyurethane coatings have many product applications due to their high tensile strength, abrasion, chemical and corrosion resistance, waterproof nature, and in some cases, skid-resistance surface. Spray-on coatings are used in many industrial, construction, architectural, and agricultural settings.
The spray-on polyurethane coating application in this incident was a spray-on truck bed liner. The truck bed liner was a 2-component system; 4,4-methylene bisphenyl isocyanate (MDI) and polyether polyol. The isocyanate and polyol were delivered in 55-gallon drums. The polyol and black dye were added to the square container. (See Figure 2) Both materials were pumped via separate hoses to a spray gun where it was mixed and applied to the truck bed under low pressure. When properly mixed at the spray gun, polyurethane was formed.
 |
Figure 2. Truck Bed Liner Mixer. |
Generally, application of a spray-on truck bed liner involves many preparatory steps, including cleaning the application area, taping/masking to prevent product overspray on the vehicle, hand and power sanding to ensure product adhesion, final clean, and then spraying the product. The company paid the employees by the job for applying the truck bed liner. The victim was usually the individual who applied the liner; one time previously another employee did apply the product to the bed of a truck. The other employees assisted in truck preparation activities, such as sanding, cleaning, etc.
After the liner has been applied the employee leaves the application area while the lining cures for approximately 15-30 minutes; the cure time depends upon temperature and humidity conditions. After the appropriate cure time, the employee re-enters the spray area to remove the tape and masking material from the vehicle. The liner continues to cure and harden. The liner is ready for customer use approximately 24 hours after application.
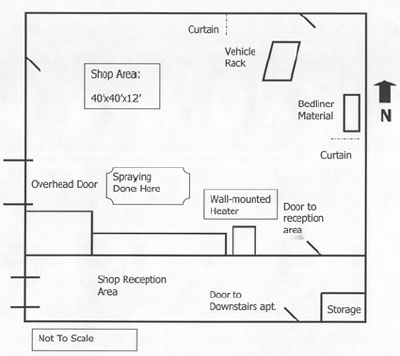
The building had two areas, the general shop area and a customer reception area. (See Figures 3, 4 and 5) A door in the customer reception area led to the basement where the victim lived. In the customer reception area was a storage room where the victim kept his personal protective equipment, both new and used. The shop area was approximately 40-feet-square and 12-feet-tall. On the west wall was an overhead door that provided shop access for the vehicles. On the north wall was a pedestrian door. Adjacent to this door was the undercoating and rustproofing area. This area had two curtains that could be pulled to enclose the area to limit product overspray into the general shop area. A natural gas heater was mounted high on the south wall to provide heat in the winter. The room did not have local exhaust ventilation. Room ventilation during the spray-on bedliner application was provided by leaving the overhead door raised a few feet and the door by the rustproofing area open and placing a box fan at this door to provide air circulation.
 |
|
Figure 3. Layout of Building. |
|
 |
 |
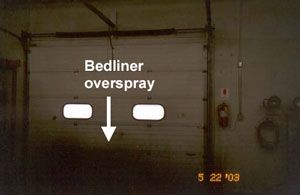
| Figure 4. Shop Overhead
Door. |
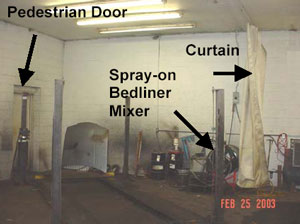
Figure 5. Rustproofing area including door, curtain, mixer. |
Figure 6 and Figure 7 show the personal protective equipment worn by the victim at the time of application of the spray-on liner. The owner also stated that the victim wore latex gloves. The ambient air pump supplying air to the ½ mask supplied air respirator had a high efficiency particulate air (HEPA) filter cartridge, which filters the air prior to being pumped to the respirator. The pump was designed for use with a 40-foot airhose.
 |
 |
|
Figure 6. Personal Protective Equipment. |
Figure 7. Personal Protective Equipment. |
Posted on the north wall was the daily startup procedure for the truck bed liner product detailing the steps that must be taken with the equipment prior to spraying the liner. The employer estimated that it takes approximately 20-30 minutes to apply the liner. The employee’s frequency of spray-on liner application depended upon the orders received; some weeks there may be several orders, but other weeks would have no orders.
The owner stated that the application of the spray-on truck bed liners occurred mostly outside of business hours due to the smell of the product. If the spraying is performed during business hours, the owner stated that the door to the reception area was kept closed and the victim would instruct other employees not to enter the shop area while he was spraying. Unknown to the owner, the isocyanate “smell” indicated that the exposure was probably above the MIOSHA permissible exposure limit and the victim may been overexposed.
The vehicle to be sprayed was a cargo van. This was the first time the company had applied the spray-on bedliner material to a cargo van. The van was prepped the day before. The spray-on liner was to be applied on the floor and partially up the sides of the cargo van. The victim with another co-worker arrived at approximately 6:30am. They set up the supplied air system for the respirator. According to the owner, he thought that the ambient air pump that supplied air to the respirator was usually placed outside of the overhead door in the parking lot. The overhead door was then lowered to a few feet above the ground. They opened the pedestrian door near the rustproofing area and placed a box fan in that door opening and prepared the spray machine. The victim donned the respiratory protection equipment, protective suit, knit cap and hood. The ambient air pump had an 80-foot airline that was connected to the ½ mask respirator facepiece assembly. The victim told the co-worker to leave the area and the coworker went to the victim’s basement apartment to wait for him to spray the van, which the victim thought would take about 20 minutes. The victim began the application of the spray-on truck bed liner at approximately 7:00am. It is unknown how the victim sprayed the inside of the van; whether he crawled in the rear and was in the confined area of the van for most of the spraying time or whether he sprayed most of the van interior while standing on the outside of the van on the shop floor. The confined area of the van interior would have a limited amount of ventilation and potentially increased the levels of isocyanate aerosols, thus increasing his exposure.
 |
Figure 8. Start Up Procedures. |
The victim completed the application of the liner inside of the van and turned off the spray machine. It is unknown where the victim disconnected his airline from his respirator at his hip; it was found near the rustproofing pedestrian door. It is unknown where the victim took off his respirator. It is thought that he exited the shop through the pedestrian northeast door by the rustproofing area. He walked outside around the north and west walls to the front door of the reception area. After waiting the 20 minutes as directed by the victim, his coworker came upstairs from the apartment and saw the victim outside of the front door of the reception area on his knees gasping for breath with the respirator hanging around his neck. The coworker drove the victim to a nearby urgent care medical clinic and the coworker went into the clinic to ask for assistance. When he returned to the vehicle, the victim was unconscious and not breathing. Emergency personnel were called and CPR was initiated. The victim was transported to the hospital by ambulance, where he was declared dead.
After the fatal incident occurred, employees informed the owner that the victim had previously experienced breathing problems after application of the truck bed liner product. Employees told the owner that the victim would cough, and go to a fresh air location. They noticed the victim sitting in a vehicle with the air blowing in his face to get “fresh air” or that the employee would take a walk after spraying the product. The employer was also told that the victim had used an inhaler in the past.
The employer did not know of any spills of the isocyanate material that could have contributed to the victim’s exposure to the chemical. The employer stated he was unaware of any rashes or breathing problems experienced by the victim prior to the incident.
SYNOPSIS
There were many factors that could have played a role in this work-related death. This was the company’s first application of the bedliner product inside of a cargo van. Spraying inside of the van provided confinement of the vapors/aerosols from the spraying and may have increased the victim’s potential exposure to the isocyanate as compared to spraying a truck bed in the open shop area. The van was placed in the general shop area and spraying occurred in absence of adequate ventilation. The respiratory protection provided to and worn by the victim may have been inadequate. The ambient air pump, designed for use with a 40-foot airline, was being used with an 80-foot airline. The employee was not properly fitted for the respirator or trained in its use and limitations of use. It is unknown if the employee conducted a user seal check for the respirator on the day of the incident. The employee did not have a medical evaluation to determine if he was medically able to wear the respirator and perform work. The employer’s knowledge of the health hazards of the isocyante component of the bedliner material was inadequate, the employer did not have a hazard communication program and did not provide employee training about the health hazards of isocyanates. It is unknown whether the employee was knowledgeable about the isocyanate sensitization properties. The victim did not alert his employer to his previous breathing problems, which may indicate he was unaware that his recurrent breathing problems after applying the bedliner were due to being exposed to the isocyanate component.
CAUSE OF DEATH
The cause of death as described by the medical examiner was acute respiratory failure. The medical examiner opinion was that he “died of acute asthmatic reaction due to inhalation of chemicals”. Toxicology results indicated that the blood contained pseudoephedrine, dipenhydramine, acetaminophen and caffeine, none of which were felt to contribute to his death. Toxicology results were negative for ethanol and all other screened drugs.
RECOMMENDATIONS/DISCUSSION
When spraying isocyanate-containing material, employers should:
Provide a ventilated spray booth or room and evaluate the effectiveness of the ventilation.
The victim was applying the isocyanate-based spray-on bedliner material in the open shop area of the facility; a spray room or spray booth was not provided. MIOSHA Occupational Health Standard, Part 528, Spray-Finishing Operations requires a spray booth or spray room to enclose or confine all spray finishing operations. Part 528 defines a spray booth as a “power-ventilated structure provided to enclose or accommodate a spraying operation to confine and limit the escape of spray, vapor, and residue, and to safely conduct or direct them to an exhaust system. A spray room is a “room in which spray-finishing operations not conducted in a spray booth are performed separately from other areas”. Part 528 provides specifications for the design and construction of both spray booths and spray rooms.
The effectiveness of the ventilation provided within the spray room or booth should also be evaluated. An employer should not make an assumption that just because a fan is within the spray room or booth that the room is being effectively ventilated and worker exposures controlled. This is especially important when spraying isocyanate-containing materials. Isocyanates are irritants to the mucus membranes of the eyes, respiratory system, and gastrointestinal tract. Isocyanates can be respiratory sensitizers, and workers can develop asthma and have other breathing problems, such as a dry cough, chest tightness and difficulty breathing. Employee exposure to isocyanates can be minimized if adequate and effective ventilation is supplied.
The MIOSHA Consultation, Education, and Training Division on-site self-help consultation program can assist an employer in conducting their own evaluation of hazardous exposures in their workplaces. This free service provides limited technical industrial hygiene guidance, air monitoring and measuring equipment, sample analyses and general information. The self-help program is designed to assist small employers, typically with 250 employees or less. MIFACE encourages employers to contact the MIOSHA CET Division at 517-322-1809 or an industrial hygienist to evaluate employee exposure and the effectiveness of ventilation within a spray room or booth. The MIOSHA CET division website can be accessed through the Michigan Department of Labor and Economic Growth website at www.michigan.gov/cis/ . Click on the MIOSHA link located in the box on the left side of the webpage, then click on the Consultation Education and Training link.
Part 528 also requires that a spray room be constructed of masonry, concrete or other noncombustible material; this includes the floor of the room and the entrance door. The spray room must also be adequately ventilated. When a spray room is used for production spray-finishing operations, it shall conform to the requirements for spray booths.
The spray room at Company A was an integral part of the building and constructed of masonry and had plastic sheeting hanging on the walls. When the plastic was dirty, the plastic was removed and replaced. The MIFACE researcher did not note the type of flooring in the spray room and the door construction.
 |
 |
Figure 9. Spray room at Company B. |
Figure 10. Spray room at Company B. |
Company B constructed their own spray room using wood framing covered in plastic and a wood door. (See Figures 9 and 10) Wood covered the cement floor and is replaced every six months. Company A and Company B had similar exhaust ventilation in their respective spray rooms by installing a fan in a wall. (See Figure 11) Company A and Company B did not perform air monitoring to determine employee exposure or to determine if the fans provided sufficient air movement (exhaust ventilation) to keep employee exposure levels below the MIOSHA standard of 0.02ppm ceiling.
MIOSHA has conducted one inspection at another spray-on bedliner company (Company C) and issued several citations as a result of that inspection. Company C used a different spray-on bedliner process (single line, heated process). Company C had a spray room, but the room did not have mechanical exhaust ventilation. MIOSHA determined through air sampling that the employees spraying the isocyanate-based material were exposed to isocyanates above permitted regulatory levels.
 |
Figure 11. Example of Wall Fan at Company
A and B. |
Often, companies that also do additional vehicle after market accessorizing, such as auto detailing and undercoating also apply spray-on bedliners. It should be noted that Part 528 allows an exemption from the requirements pertaining to spray-finishing operations for automobile undercoating spray operations in garages, conducted in areas having adequate natural or mechanical ventilation when the undercoating materials used are not more hazardous than kerosene (as listed by Underwriter’s Laboratories in respect to fire hazard rating 30-40) or undercoating materials using only solvents listed as having a flash point in excess of 100 degrees F. Undercoating spray operations not conforming to these provisions are subject to all requirements of this rule pertaining to spray-finishing operations.
Although the company owner required the employee to wear a ½ facepiece, supplied air respirator while applying the spray-on liner, the owner did not have a written respiratory program. The employer did not conduct an exposure assessment to evaluate the respiratory hazard and did not evaluate the respiratory hazard. The employer also did not provide a medical evaluation to determine the employee’s ability to wear a respirator. The employee, according to the medical examiner’s autopsy report, had chronic obstructive pulmonary disease with emphysema. The employee’s medical status may have prohibited him from wearing a respirator and thus performing the spray application. The employee did not have a fit test. Without a fit test, it is unknown whether a proper fit was achieved, i.e., a tight seal between victim’s face and the respirator facepiece.
The MIOSHA Occupational Health Standard, Part 451, Respiratory Protection requires that when a respirator is necessary, an employer have a worksite-specific written respirator program that includes workplace specific procedures addressing the elements of the program. This means that employers must select and provide an appropriate respirator based on the respiratory hazard(s) to which the worker is exposed as well as the workplace and user factors that affect respirator performance.
The MIOSHA standard requires that an employer, among other things:(1) Identify and evaluate the respiratory hazard(s) in the workplace.
Evaluation of a respiratory hazard must include a reasonable estimate of employee exposure to the hazard and an identification of the contaminant’s chemical state and physical form. The exposure assessment not only assists in determining the effectiveness of ventilation but also assists in selection the appropriate respiratory protection. If the employer cannot identify or reasonably estimate the employee exposure, the employer must consider the atmosphere to be immediately dangerous to life and health (IDLH). An IDLH atmosphere requires a full facepiece pressure demand SCBA or a combination full facepiece pressure demand supplied-air respirator with auxiliary self-contained air supply.
Full facepiece respirators, if properly fitted and the user properly trained provide a higher degree of respiratory protection than does a ½ mask respirator. Due to the sensitizing capability of isocyanates, MIFACE recommends that when spraying isocyanate materials, a supplied air full facepiece respirator be used to provide the best protection.
(2) Provide a medical evaluation and respirator fit test prior to employee wearing the respirator on the job if he/she is required to wear the respirator to perform the job.
Because using a respirator may place a physiological burden on the wearer depending on the type of respirator used, the employee’s job, the workplace conditions, and the wearer’s medical status, Part 451 requires that an employer provide a medical evaluation to determine the wearer’s ability to use a respirator before he/she is fit tested or required to use the respirator. The employee must be fit-tested with the same make, model, style and size of respirator that he/she will use. The fit test ensures that the proper respirator is selected for the employee so that there is a no leakage and that the respirator will provide adequate protection. Fit test protocols are located in Appendix A of Part 451.
(3) Provide annual training to an employee who is required to wear a respirator.
Part 451 requires employers to provide comprehensive, understandable respirator training and that the employee must be able to demonstrate that he/she has knowledge of the training elements. Employees must receive annual training. The training elements must include why the respirator is necessary and how improper fit, usage or maintenance can compromise the protective effect of the respirator, the limitations and capabilities of the respirator, how to use the respirator effectively in emergency situations, how to inspect, put on and remove, use and check the seals of the respirator, maintenance and storage procedures, recognition of the medical signs and symptoms that may limit or prevent the effective use of the respirator, and the training requirements under the Part 451.
(4) Establish and implement procedures for the proper use, storage, cleaning and inspection of respirators as part of the written.
The procedures should also include the pump supplying air to the respirator.
It is unknown when the ambient air pump’s HEPA filter cartridge was
checked and replaced. The ambient air pump the employer selected was designed
for use with a 40-foot airline. The victim was using an 80-foot airline. The
additional 40 feet of line may have impacted the amount of air that was supplied
to the facepiece, thus not providing the expected protection.
Proper use of a respirator is critical; if used improperly, adequate protection
will not be afforded to the wearer. Procedures for use should include conditions
that may interfere with the face-to-facepiece seal. It is unknown the amount
of facial hair the victim had on the day of his death and if facial hair interfered
with the face-to facepiece seal. The procedures should also include a requirement
that the employee not remove the respirator and/or respirator airline while
within the hazardous environment. The airline for the victim’s respirator
was found inside of the shop. It is unknown if the victim unhooked the airline
inside of the shop or if he unhooked the respirator outside of the shop and
placed the hose inside of the shop.
Neither Company A or Company B had a written respiratory program, evaluated the respiratory hazard(s) in the workplace, evaluated the spray room ventilation, had employees undergo a medical evaluation, fit-tested employees or had procedures for proper use, storage, cleaning and inspection of the respirator.
Company A required employees to wear the ½-mask airline respirator when reentering the spray room to remove the taping/masking from the vehicle. Company B wore a dust mask during the removal of the tape and masking material. MIFACE recommends that if the ventilation is not evaluated, that employees wear an air-supplied respirator when re-entering the room to remove the tape and masking materials from the vehicle to minimize potential exposure to unreacted isocyanate.
The employer did not have a written hazard communication program in place at the facility. He maintained copies of Material Safety Data Sheets (MSDSs) for the two bedliner components. The employer stated to the MIFACE researcher that prior to the incident he did not know that the MDI component of the spray-on bedliner was a known respiratory system sensitizer.
Chemicals can pose both health hazards (such as irritation, sensitization, and carcinogenicity) and physical hazards (such as flammability, corrosion, and reactivity). An employer’s hazard communication program should ensure that information about these hazards and the associated protective measures required is disseminated to employees. If an employer has hazardous chemicals in their workplace, then a written hazard communication program must be prepared and implemented. MIOSHA Occupational Health Standard, Part 430, Hazard Communication, 29 CFR 1910.1200(e) and the Michigan Right to Know Law requires employers to develop, implement and maintain at each workplace a written hazard communication program which addresses specific topics. The program must ensure that all containers are labeled, employees are provided access to MSDSs, and an effective training program is conducted for all potentially exposed employees.To assist employers recognize and control occupational chemical hazards, the National Institute for Occupational Safety and Health (NIOSH) has developed the “NIOSH Pocket Guide to Chemical Hazards” (NPG). The “NIOSH Pocket Guide to Chemical Hazards” can be downloaded or ordered as a CD-Rom or by printed version from the NIOSH website at www.cdc.gov/niosh/npg/ (Link updated 11/13/2006)
The goals of the hazard communication standard are two-fold: give employers the information they need to design and implement an effective protective program for employees potentially exposed to hazardous chemicals and provide workers with information about the health and physical hazards of the chemicals they work with so that they can effectively participate in their employers’ protective programs as well as take steps to protect themselves.
Although there is no legal requirement to perform medical surveillance on individuals who work with asthma causing agents (exception: formaldehyde), employers should establish a medical surveillance program for workers who are exposed to isocyanate materials. The dose that an individual inhales from both usual daily exposure and non-routine heavy exposures from spills is the best predictor of who will become symptomatic. The longer an individual remains exposed to an occupational allergen that he/she has become sensitized to, the more severe their symptoms will become and the more likely that he/she will have persistent breathing problems even after exposure has ended. Medical surveillance can be used as a screening tool to identify individuals who may be having breathing problems due to the materials they are working with, and before they develop symptoms that may result in a chronic disability, remove them from that exposure. None of the companies had instituted medical monitoring for their employees. The victim had had ongoing respiratory problems with spraying. A medical surveillance program would have identified his breathing problem and allowed intervention that potentially would have prevented his death.
An employer is required by MIOSHA Occupational Health Standard, Part 443, Personal Protective Equipment to assess the workplace to determine if hazards are present or are likely to be present that requires the use of personal protective equipment. The employer must verify, through a written certification that the hazard assessment has been performed.
MIOSHA CET Division has two consultation programs to assist employers in assessing their workplace for safety and health hazards. Occupational safety consultants or industrial hygienists in the CET on-site consultation section conduct these on-site consultations upon employer request. MIOSHA CET Division personnel will conduct a non-enforcement hazard survey of the employer's site (full or partial). The hazard survey is a training tool, which affords the employer and selected employees the opportunity to learn how to identify unsafe or unhealthy acts or conditions, and MIOSHA violations. The hazard survey results in formulating ways to correct any noted deficiencies. Employers may also request CET personnel to conduct a MIOSHA inspection of their workplace (full or partial) without the attachment of fines or penalties. Employers must agree, prior to the start of this inspection, to correct all serious violations found during the voluntary inspection. Currently, priority for participation in this program is given to manufacturing sector employers with less than 250 employees. Other requests are reviewed on a case-by-case basis.
The Alliance for the Polyurethanes Industry has two technical bulletins that specifically address MDI use. These technical bulletins can be found on the Alliance for the Polyurethanes Industry website at www.polyurethane.org/bookstore/. Click on Environmental Health and Safety and a list of API Technical Bulletins will be listed. One document is “Working with MDI and Polymeric MDI: What You Should Know”, Technical Bulletin #AX205. This document assists a user in identifying MDI, recognizing potential health hazards, protecting yourself from MDI overexposure, understanding potential reactivity hazards, handling, unloading and storing MDI and how to respond to emergencies. Another MDI-specific technical bulletin is “PMDI User Guidelines for Protective Clothing Selection”, Technical Bulletin #AX178. This document assists MDI users in selecting the appropriate personal protective equipment. Other API Technical Bulletins that may be of interest to spray-on bedliner applicators using polyol as one component of the bedliner may include Technical Bulletin AX228, “Polyol Resin Blends Safety and Handling Guidelines”.
The federal Occupational Safety and Health Administration (OSHA) also has a tool employers/employees can use to identify possible safety and health hazards in their workplace OSHA’s Hazard Awareness Advisor can be downloaded or used on-line. The Advisor’s Internet address is http://www.osha.gov/dts/osta/oshasoft/index.html#eTools. Although the Advisor directs users to the OSHA standards addressing identified hazards, Michigan employers must comply with applicable MIOSHA safety and health standards.
A workplace hazard assessment should also include safety hazards, such as sharp edges on vehicles, airlines from both the respirator and bedliner application equipment, flammable materials used in conjunction with the application of the bedliner materials, proper bonding and grounding of flammable liquids, locating space heating appliances (gas powered heater with pilot light) in a spray area where deposits of combustible residues may accumulate, etc. Company B, for example, soaked the applicator gun parts in a labeled coffee can filled with flammable solvents. A coffee can is not an approved container for flammable solvents. A “NO SMOKING” sign was not present in the vicinity of the flammable solvents. (See Figure 12)
for cleaning spray gun parts.
Small business owners often rely on the manufacturer or product distributor for health and safety information. When training on the product is given to end user workplaces, manufacturers/suppliers/distributors should ensure that the health and safety aspects are included in the training. All three worksites MIFACE visited did not know that an isocyanate is considered to be a sensitizing agent. They also did not know what a sensitizing agent was. Health and safety information given by the manufacturer allows the end user to implement safe work procedures so employees may safely use the material or process. The manufacturer/supplier/distributor should inform end users of the importance of medical surveillance when their products contain agents that are sensitizers or may cause asthma.
REFERENCES
MIOSHA Standards cited in this report can be directly accessed from the Michigan Department of Labor and Economic Growth, MIOSHA website www.michigan.gov/dleg/0,1607,7-154-11407_15368---,00.html.(Link updated 12/11/2007)
The Standards can also be obtained for a fee by writing to the following address: Department of Labor and Economic Growth, MIOSHA, Management and Technical Services Division, MIOSHA Standards Section, P.O. Box 30649, Lansing, MI 48909-8149. The Management and Technical Services Division phone number is (517) 322-1817.
MIFACE (Michigan Fatality and Control Evaluation), Michigan State University (MSU) Occupational & Environmental Medicine, 117 West Fee Hall, East Lansing, Michigan 48824-1315. This information is for educational purposes only. This MIFACE report becomes public property upon publication and may be printed verbatim with credit to MSU. Reprinting cannot be used to endorse or advertise a commercial product or company. All rights reserved. MSU is an affirmative-action, equal opportunity employer. 12/19/03
To contact Michigan State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
| To improve the quality of the MIFACE program and our investigation reports, we would like to ask you a few questions regarding this report. | |||
| Please rate the following on a scale of: | |||
| Excellent | Good | Fair | Poor |
| 1 | 2 | 3 | 4 |
| What was your general impression of this MIFACE investigation report? | |||
| Excellent | Good | Fair | Poor |
| 1 | 2 | 3 | 4 |
| Was the report… | Excellent | Good | Fair | Poor |
| Objective? | 1 | 2 | 3 | 4 |
| Clearly written? | 1 | 2 | 3 | 4 |
| Useful? | 1 | 2 | 3 | 4 |
| Were the recommendations … | Excellent | Good | Fair | Poor |
| Clearly written? | 1 | 2 | 3 | 4 |
| Practical? | 1 | 2 | 3 | 4 |
| Useful? | 1 | 2 | 3 | 4 |
| How will you use this report? (Check all that apply) | |
| O | Distribute to employees/family members |
| O | Post on bulletin board |
| O | Use in employee training |
| O | File for future reference |
| O | Will not use it |
| O | Other (specify) __________________________________________ |
Thank You!
Please Return To:
MIFACE
Michigan State University
117 West Fee Hall
East Lansing, MI 48824
FAX: 517-432-3606
Comments:
| If you would like to receive e-mail notifications of future MIFACE work-related fatality investigation report summaries, please complete the information below. | |
| Name: __________________________________________ | |
| e-mail address: ___________________________________ | |
| I would like to receive summaries for reports involving: | |
| ___ Construction | ___ Agriculture |
| ___ Manufacturing | ___ All |

![]()
