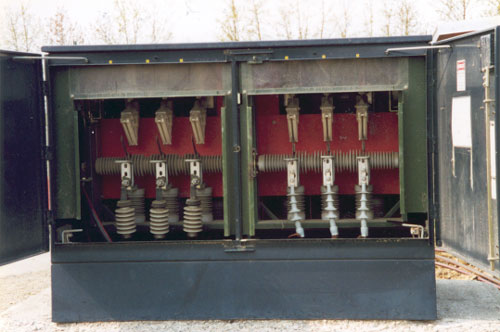
Figure 1. View of open switch cabinet

Figure 2. View of trench and cables leading
under foundation
under foundation
FACE 00-AK-011
Lineman Killed After Contacting Charged Switch
SUMMARY
A lineman (the victim) was killed after contacting a 17,400-volt charged switch. The victim was part of a three-man crew replacing cables under a switch cabinet. At the time of the accident, the crew was feeding a new cable under the concrete foundation pad below the cabinet. As one worker pushed the cable under the foundation, the victim looped the cable inside the foundation under the cabinet. The victim was using a hot stick to loop the cable but was not wearing his hardhat when his head came either in close proximity to or contacted the charged switch. Crewmembers saw a flash and came around the switch cabinet to where the victim was located. He was found slumped partially in the cabinet. A crewmember used a hot stick to move the victim away from the cabinet and then began CPR. Emergency Medical Services transported the victim to a nearby hospital where he was declared dead from injuries associated with high-voltage electrocution.
Based on the findings of the investigation, to prevent similar occurrences, employers should:
INTRODUCTION
At 12:15 PM on May 10, 2000, a 40-year-old lineman was killed while working on an energized switch cabinet. On May 10, 2000, Alaska Department of Labor and Workforce Development (AKDOLWD) notified the Alaska Division of Public Health, Section of Epidemiology. An investigation involving an injury prevention specialist for the Alaska Department of Health and Social Services, Section of Epidemiology ensued on May 11, 2000. The incident was reviewed with AKDOLWD officials. Police Department, Fire Department, Medical Examiner, and AKDOLWD reports were requested. An inspection of the site was completed on May 14, 2000.
The company in this incident was a privately owned electrical contracting company and had been in business for 25 years. The company employed a minimum of 70 workers; employment increased during summer months to approximately 150 employees. The majority of electrical workers were well experienced (journeyman level). The company also participated in an approved state apprenticeship program. The company acknowledged journeyman and foreman level linemen as industry-competent, requiring little to no training after initial hire orientation. The company had employed the victim as a journeyman lineman for 3 years.
The company had a comprehensive safety program and conducted weekly toolbox safety meetings. Topics included tool safety, electrical hazard, prevention of slips and falls, and near-miss reviews. Apprenticeship linemen assigned to the company received safety and health training from the state electrical apprenticeship program. Apprentices also received on-the-job training and instruction appropriate to their work experience level and knowledge.
INVESTIGATION
The incident occurred at a privately owned recreation site. Prior to opening for their season, the site administrators had contracted the company to locate, excavate, and replace buried electrical cables connecting transformers throughout the site. A crew was assigned and was comprised of three linemen: a foreman, a journeyman (the victim), and an apprentice. The two days prior to the incident, the crew located the buried cables to be replaced and began excavation, initially using a backhoe and then manual digging to expose the cables. The trenches averaged 2 feet wide and 3 to 3½ feet deep.
On the day of the incident, the crew completed excavation of a trench that ran between two transformers. After removing and laying new cable, the crew stopped work and left for lunch. The crew intended to complete the installation of the cable into the switch cabinet that afternoon.
The switch cabinet involved in this incident was a pad-mounted cabinet with a metal exterior. The cabinet was approximately 6½ feet wide, 4 feet deep and approximately 3½ feet tall. The cabinet contained six switches aligned side by side along the 6½-foot length of the cabinet. On the opposite side of the cabinet were six fuses aligned in the same arrangement as the switches. On each side of the 6½-foot length of the cabinet were two access doors (four doors in total). Three switches or fuses were behind each door. (Figure 1)
The cabinet was open at the bottom and rested on a pre-formed concrete foundation or vault. The vault was approximately 3 feet deep--1 foot above and 2 feet below ground. Normally, several feet of cable were looped around the interior perimeter of the vault. This is a normal industry practice.
The crew had discussed the cable installation prior to proceeding with the afternoon activities. The left side of the switch cabinet was de-energized by opening the switches and removing the existing fuses on the opposing side. The right side of the box remained energized, allowing the administrative offices to continue to have power and not experience any power outages during the installation process. The crew foreman was on the fuse side of the box in the trench. He was feeding the cable underneath the vault into the open interior area within the vault under the box. (Figure 2) However, the trench led to the still energized side of the switch cabinet. The victim was on the switch side of the box wearing insulated gloves and using a hot stick to loop the cable inside the bottom of the vault. During this time, the victim was wearing a cloth cap not his electrical industry-approved hardhat.
All four doors to the cabinet were opened to view the area inside the vault. In addition, the insulated safety barrier was removed on the energized portion of the cabinet in front of the switches to provide better visibility and access to the cable. The victim using a hot stick had already looped several feet of cable within the vault, and the apprentice was observing his actions. The victim’s head and upper body were within the hot zone (24 inches or less) of the energized switches. He requested that the apprentice move away from the hot zone of the box, and the apprentice walked around to the opposite side of the cabinet near the foreman and was asked to retrieve a tool from the truck. The victim continued to guide the cable around the interior of the box. It is not known if his head came in contact with the energized post below the energized switches or if the close proximity of his body to the energized post conducted an electrical arc between his head and the energized post.
The apprentice and the foreman heard a noise and saw a bright flash. The victim was found slumped partially inside the right-hand door. Using a hot stick, the foreman moved the victim away from the cabinet. The two coworkers started CPR.
Power to the administration offices went out. Employees in the offices had heard a loud “bang” then yelling outside. They went out to investigate and saw the victim on the ground. One employee ran back to the office to call 911, but found the phone did not work due to the power outage. The employee then ran to another building on the site to call 911. A second 911 call was placed using a cell phone. Police and Emergency Medical Service (EMS) personnel were dispatched at 12:20, approximately 5 minutes after the incident, and arrived at the site 3-5 minutes later. EMS personnel continued CPR approximately 30 minutes at the site and then transported the victim to a local hospital. The victim was declared dead.
CAUSE OF DEATH
The medical examiner's report listed the cause of death as high-voltage electrocution. Toxicology laboratory results indicated 9 ng/ml THC and 15 ng/ml carboxy-THC in the victim's blood at the time of death.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Employers should ensure that workers use personal protective equipment and enforce its use.
Discussion: In this incident, the victim was not wearing his hardhat while working in close proximity to the energized unit. This part of an electrical lineman's personal protective equipment is essential and could have prevented physical contact with the energized components of the cabinet. The non-conductive material of the hardhat, specifically approved for electrical industry practices, may have also acted as a barrier.
The purpose of a comprehensive safety program is to identify, reduce or eliminate exposure to hazardous situations; and control worker risk to an unavoidable hazard by providing appropriate personal protective equipment and training. Employers need to enforce all aspects of their safety program. Employers should also regularly inspect work sites, observe worker practices, and review job tasks to determine the extent and significance of actual and potential hazards and modify safety precautions to promote safe work practices.
Recommendation #2: Employers should ensure workers are capable of recognizing
and avoiding hazardous situations.
Discussion: In this incident, the victim recognized the potential hazard to his apprentice, who was observing the installation process. However, the victim failed to recognize his own risk to the electrical hazard. While employees may regularly complete tasks with a high risk of injury or hazard, the probability of injury to the employee remains the same. Employees should be counseled on issues leading to complacency.
While employees have the right to question the safety of any task, they are responsible for following the practices outlined by their employer’s safety program. In addition to specific safe practices, steps should be outlined and discussed with employees for noncompliance with an established safety program practice and how to participate in job safety analysis for the continuous assessment and improvement of safe work practices.
Recommendation #3: Employers should emphasize de-energizing, isolating,
or cover energized areas whenever personnel need to work within high voltage
danger zones.
Discussion: Foreman and journeyman level electricians and lineman are among the most experienced and knowledgeable workers within the electrical contracting industry, receiving extensive training in electrical safety. However, NIOSH and state-based FACE programs investigated 224 electrocutions (from November 1982 to December 1994) that resulted in 244 worker deaths. Utility linemen had the highest number of fatal injury of which 55% were due to failure to use required protective equipment (gloves, mats, blankets, etc.) While certain conditions may require work to be performed on high voltage equipment, work space around the equipment must be carefully assessed. Line workers should always consider de-energizing, isolating, or covering energized areas when working on or in close proximity (24 inches or closer) to energized high voltage equipment.
Employers should consider providing additional specialized electrical safety training for workers and management personnel to increase understanding and awareness of high voltage electrical energy hazards and the need to endorse safe work practices for the completion of individual tasks and construction projects in total.
|
Figure 1. View of open switch cabinet |
|
Figure 2. View of trench and cables leading
under foundation |
REFERENCES
Fatality Assessment and Control Evaluation (FACE) Project
The Alaska Division of Public Health, Section of Community Health and Emergency Medical Services performs Fatality Assessment and Control Evaluation (FACE) investigations through a cooperative agreement with the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR). The goal of these evaluations is to prevent fatal work injuries in the future by studying the working environment, the worker, the task the worker was performing, the tools the worker was using, the energy exchange resulting in fatal injury, and the role of management in controlling how these factors interact.
To contact Alaska State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
![]()