|
|||
|
|
Fatality Assessment and Control Evaluation (FACE) Program |
|
18-year-old Dies After Being Entangled in a Portable Mortar Mixer - South Carolina |
| |||||||||||||||||||||
SummaryOn May 15, 2003, an 18-year-old laborer (the victim) died after becoming entangled in a portable mortar mixer. The victim was cleaning the mixer at the end of his shift at a residential construction site to prepare it for the following day while a co-worker was brushing down the recently laid brick wall nearby. A painter working near the victim heard yells for help and saw the victim’s arm stuck in the machine and his body being pulled into the rotating mixer paddles. He ran to the mixer and attempted to turn it off but could not disengage the gears so he yelled for help. The co-worker heard the commotion, ran to the machine, and shut it off. Emergency Medical Services was called and responded within minutes. Rescue workers dismantled the drive mechanism to reverse the mixing paddles and extricated the victim. The victim was pronounced dead at the scene. NIOSH investigators concluded that, to help prevent similar occurrences, employers should:
Additionally, manufacturers should:
IntroductionOn May 15, 2003, an 18-year-old laborer (the victim) for a brick laying company died after becoming entangled in the rotating mixing paddles of a portable mortar mixer. On May 21, 2003, the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR), was notified of the incident by the South Carolina Department of Labor, Licensing and Regulation, Office of Occupational Safety and Health Administration (SCOSHA). On June 18, the Team Leader for the Fatality Assessment and Control Evaluation (FACE) program met with a compliance officer at the SCOSHA to review the case. On June 29, 2003, the Chief of the DSR Trauma Investigations Section and an Associate Service Fellow met with the owners of the company, and inspected and photographed the mixer. The case was discussed with the county coroner and local police and photos taken by the agencies were reviewed. The case was discussed via phone with the Vice President of Engineering at the mixer’s manufacturing facility and the operator’s manual was reviewed. The brick and masonry contracting business had been in operation for over 20 years. The company employs seven persons—five laborers and two brick masons who were co-owners of the business. The company specializes in residential construction and this was the company’s first workplace fatality. The machine, an 8-cubic-foot portable mortar mixer with a gasoline powered 8-hp engine was purchased new by the company in 1998 (Photo 1). It is equipped with an automatic guard lifter which lifts the drum guard as the drum is emptied to prevent mortar from being poured through the guard and causing build up. In normal operation, lifting the drum guard gives about eight inches clearance for the mortar to pour through. Photo 2 shows the mixer drum in an upright position with the guard in place. The mixing paddles in the drum are engaged by moving the clutch lever [located on the vertical support on the right side of the drum] to the right (downward) (Photo 3). An upright (disengaged) lever position is shown in Photo 4. Moving the clutch lever downward engages the paddles regardless of the drum position. A drum latch (Photo 2) in the downward position secures the drum upright while the rubber tipped paddles rotate between 33 and 35 revolutions per minute to mix the mortar. The machine was in fair condition and had the manufacturer’s installed guarding at the time of the site visit. It had been repainted and a gear replaced since the incident. Upon hire, the company owners give training on specific tasks related to the job. In this case, demonstrations on the use of the portable mixer were provided to the victim by one of the company owners. All training is hands-on and no documentation of training is completed. Certification or licensing of the machine or operator is not required. Routine checks of the machine are conducted by the owners to assure proper operation. Operator proficiency is evaluated by the owners through demonstration and follow-up observation The company lacks a comprehensive written safety training program or related policies. Tailgate safety meetings are held as needed by the company owner. One owner reported that three days prior to the incident, the mixer was the primary topic of the tailgate safety meeting. The victim worked for the company as a laborer for 4 months, 40 hours per week. His primary responsibilities included mixing mortar, hauling it to the brick layer in a wheelbarrow, and transporting bricks from a pallet to the brick mason work area.Back to TopInvestigationThe day of the incident, the victim, one mason and one site foreman, who was not a co-owner, were at a private residence bricking a pool house. Work began at 7:00 am in 70 degree warm and dry conditions. The victim mixed mortar, carried brick, and prepared the site for the brick mason. At the time of the incident, a painter, not employed by the brick and masonry contractor, was in the area and a lawn crew was mowing the yard and doing landscape maintenance. The mixer was set up on a driveway adjacent to a pile of sand. The crew had been at this site about 40 days prior to the incident and was nearly done with the project. The foreman left the site about 3:00 pm to check on another job. At approximately 3:20 pm, the victim was told by the mason to clean out the mixer in preparation for the next day. This was a routine procedure done at the end of each day to prevent the mortar from curing or setting up on the mixing paddles or the sides of the mixing drum. The mason then went to another part of the job site to brush the brick wall he had just laid. The victim had turned the drum so the opening was directed toward the ground allowing water to drain out. Using a garden hose in his right hand, the victim sprayed the paddles and inside of the drum loosening the mortar and allowing the residue to drain out. During this procedure the engine was running, mixing blades rotating, guard lifter disconnected and drum guard fully open. The victim then rotated the drum upright and continued spraying water into it. The painter reported that he heard a scream, saw the victim’s arm get caught, and ran to the mixer attempting to shut it off. He could not shut the engine off so he called for others to help. By this time the victim had been pulled into the machine. A crew of Spanish-speaking lawn maintenance workers ran to the scene after hearing the painter yell for help. This commotion caused the brick layer to take notice and run toward the mixer from around the far side of the pool house. Seeing the victim’s leg protruding from the top of the mixer and hearing the engine running, the brick layer disengaged the mixing paddles by moving the clutch lever upward. He then turned the engine off. A neighbor called 911 and the rescue squad and police arrived within minutes. The rescue squad personnel removed the belt to disengage the blades so they could be rotated in reverse to free the victim. The victim was pronounced dead at the scene. Cause of DeathThe coroner determined the cause of death to be asphyxia due to compression of neck structures by concrete mixing device. Back to TopRecommendations/DiscussionRecommendation #1: Employers should develop, implement and enforce a written safety program which includes, but is not limited to, task-specific hazard identification, avoidance and abatement.Discussion: Employers should evaluate all tasks performed by workers; identify all potential hazards; and then develop, implement, and enforce written safe work procedures addressing these tasks. The safety program should include at a minimum how workers can protect themselves from injury. In this case, no written safety program or procedures were available. A written program offers consistency in safety procedures and could have informed the worker of the dangers related to cleaning the mixer. The safety program should emphasize the link between unsafe behavior and the potential for injury. Written task-specific procedures should be a part of the safety program and regular structured safety meetings should be held and documented.
| ||||||||||||||||||||||
 |
|
 |
 |
Photo 3. Clutch in the ‘on’ position, paddles rotating. |
Photo 4. Guard off, clutch in the
‘off position. |
 |
|
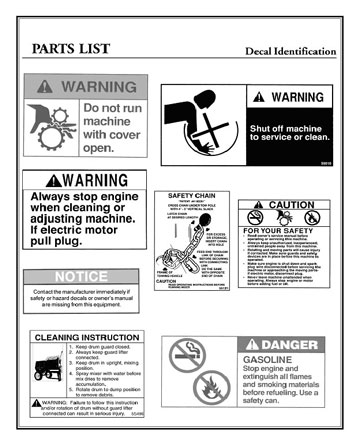
Figure
1. Manufacturer’s Warning labels. |
|
 |
|

