Fatality Assessment and Control Evaluation (FACE) Program |
|
Hispanic Carpenter Killed When Struck by Piece of Concrete That Fell From Rigging Device During Hoist in Highway Work Zone |
| |||||||||||||||||
SummaryA 51-year-old Hispanic male carpenter was killed when struck by a 2000
pound piece of The Nebraska Workforce Development, Department of Labor’s Investigator
concluded
Program ObjectiveThe goal of the Fatality Assessment and Control Evaluation (FACE) workplace investigation is to prevent future work-related deaths or injuries, by a study of the working environment, the worker, the task the worker was performing, the tools the worker was using, and the role of management in controlling how these factors interact. This report is generated and distributed solely for the purpose of providing current, relevant education to employers, their employees and the community on methods to prevent occupational fatalities and injuries. IntroductionOn December 12, 2005, at approximately 9:30 a.m., a 51-year-old male
carpenter died The victim’s employer is a steel fabrication/bridge building (SIC
Code 1622) company. Back to TopInvestigationPersonnel: Victim: The victim was a 51-year-old Hispanic
male. He had been employed by Job Superintendent: He had been employed by
this company for several years. Crane Operator: He was a Hispanic male who
had operated cranes for this
Crane: American model 5299 Man lift: Mark Lift model 62C 4x4 Back to TopAnalysis/SynopsisThe victim (worker #1) was part of a seven-person crew working on a new bridge project. On the day of the accident the crew was installing concrete “cap” on top of a 30 foot high interlocking concrete retaining wall below a new bridge. Worker #2 was operating the crane. Workers #3, a mechanic & #4, a rigger were on the ground connecting the pre-cast concrete “cap” to the crane’s rigging. Workers #5 & #6 were on top of the concrete wall, waiting on the “cap” to be hoisted in place so they could shim it level. The victim and the job superintendent (worker #7) were in a man lift which was at ground level. Once the “cap” was in place, they would raise themselves up to the “cap” to grout and finish the installation process. The concrete “caps” were manufactured according to contract specifications by the victim’s company. They were approximately 10 feet in length, 2 feet high, and 16 inches thick, weighing approximately 2,000 pounds each. As each “cap” was poured, a commercially produced steel threaded insert was recessed its entire length plus approximately ½” into each end of the concrete form. A piece of rebar was then inserted through the loop at the bottom of the insert to firmly secure the insert inside of the “cap”. Under normal circumstances, to lift the “cap” a steel eye-bolt was threaded into the insert. A double-leg chain sling was attached to both ends, which was attached to a chain hooked onto the crane’s hook. The “cap” was lifted into place and secured. The eyebolts were unscrewed and used again to lift more “cap”. Work had to be delayed several days due to a severe snowstorm in the area. After the crew returned to the work site they could not locate the eye bolts. After discussion, the Job Superintendent (worker #7) decided they could take two pieces of 3”x3” angle iron approximately 6” long and use a cutting torch to make a hole in each side (one for the bolt, one for the sling), attach them to the “cap” with square-headed straight-bolts of the same diameter as the eye bolts and continue to lift “cap” into place. This procedure, using square-headed straight-bolts instead of the regular eye-bolts had never been used before. After fabricating the angle iron pieces, the new straight bolts were installed and used to move four pieces of “cap” without incident. Workers #2 & #4 screwed the bolts into the threaded insert and tightened them snug. Worker #2 raised the “cap” into the air and swung it toward the retaining wall, causing it to be swung over worker #4. It stopped above the victim and worker #7 in the man lift basket. As the “cap” was being raised (somewhere between 10 and 30 feet high) one of the bolts pulled out of the threaded insert. This caused the “cap” to swing towards the opposite side. The weight and pressure applied to the remaining bolt caused it to fail, and it pulled out of the threaded insert. The “cap” fell, striking the victim on his hard hat and body. The “cap” hit the man lift basket with sufficient force to cause it to jerk sideways with enough force into worker #7’s body, breaking several ribs. Back to ToCause of DeathAccording to the death certificate, the cause of death was: Blunt force trauma to the body. Back to TopRecommendations/DiscussionRecommendation #1: Ensure rigging and other equipment being used is suitable for the intended load.Discussion: The “tried & approved” method for lifting the “cap” could not be used due to the loss of the eye bolts. A decision was made by the Job Superintendent to use fabricated pieces of angle iron and substitute bolts to secure the “cap” to the crane’s sling. For unknown reasons, one of the straight bolts pulled out of the threaded insert. This allowed the pre-cast “cap” to swing away to the opposite side, placing all of the weight on the remaining bolt, causing it to also fail and pull out of the threaded insert. This allowed the “cap” to fall, striking the victim, leading to his death. Reference: 29 CFR Part 1926.251(a)(1), Occupational Safety and Health Standards for the Construction Industry, February 1, 2004: Rigging equipment for material handling shall be inspected prior to use on each shift and as necessary during its use to ensure that it is safe. Defective rigging equipment shall be removed from service. Reference: 29 CFR Part 1926.251(b)(3), Occupational Safety and Health Standards for the Construction Industry, February 1, 2004: Job or shop hooks and links, or makeshift fasteners, formed from bolts, rods, etc., or other such attachments, shall not be used. Reference: 29 CFR Part 1926.704(c), Occupational Safety and Health Standards for the Construction Industry, February 1, 2004: Lifting inserts which are embedded or otherwise attached to pre-cast concrete members, other than the tiltup members, shall be capable of supporting at least four times the maximum intended load applied or transmitted to them.
| ||||||||||||||||||
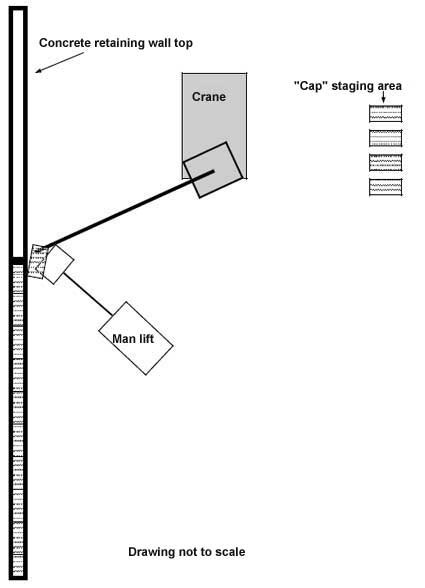 |
| Attachment 1.
Site diagram (Diagram not to scale) |
 |
| Attachment 2. Top of the concrete interlocking retaining
wall
|
 |
| Attachment 3. Man lift personnel basket with concrete “cap”
|
 |
| Attachment 4. Job-site manufactured lifting devices that
|
 |
| Attachment 5. Bolts that were screwed into threaded inserts
|
 |
Attachment 6. New threaded insert with bolt involved in accident.
|
 |
Attachment 7.
New threaded insert with bolt attached to lifting device. Bolt & angle iron piece are from accident. |
To contact Nebraska
State FACE program personnel regarding State-based FACE reports, please
use information listed on the Contact Sheet on the NIOSH FACE web site
Please contact In-house
FACE program personnel regarding In-house FACE reports and to gain
assistance when State-FACE program personnel cannot be reached.