Investigation: # 02MI090
Journeyman Pipefitter Killed When Struck in Head by Grooved End Cap under Pressure
|
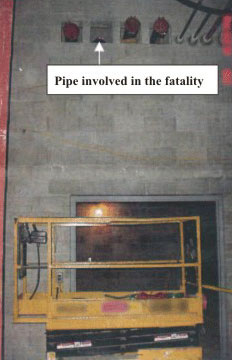
| Figure 1. Pipes and Scissors Lift |
Another co-worker who heard the noise came to assist and found the victim bleeding
from the face and having difficulty breathing. EMS arrived shortly, treated
the victim, and transported him to the emergency room of a local hospital. He
died in the hospital eighteen hours later.
RECOMMENDATIONS
INTRODUCTION
On Tuesday, October 29, 2002, a 49-year old journeyman pipefitter
was struck in the head by a 6-inch diameter grooved cap he was removing from
the end of a pipe. He died in the hospital 18 hours later. On October 30, 2002,
MIFACE investigators were informed by the Michigan Occupational Safety and Health
Act (MIOSHA) personnel who had received a report on their 24 hour-a-day hotline
that a work-related fatal injury had occurred. On February 28, 2003, the MIFACE
researcher interviewed the president of the company that employed the pipefitter.
He described the events on the day of the fatality as they had been told to
him by the pipefitter’s co-worker. He accompanied the researcher into
the plant, showed her various parts used for blanking pipes and described their
functions, and allowed her to photograph them. The company president also provided
the author with photographs of the site where the fatality occurred, copies
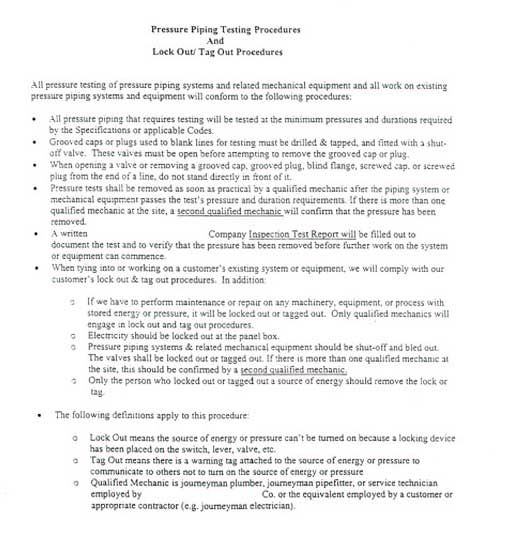
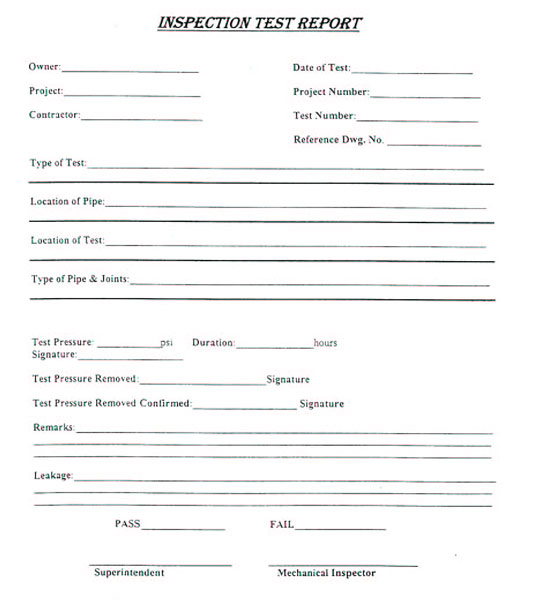
of the company’s newly developed pressure piping testing and lock out/tag
out procedures, and copies of several pages of commercially available welded
fittings, flanges, flange adapters, and couplings. During the course of writing
the report, the medical examiner’s report, the autopsy, the responding
police department’s report and photographs, and the MIOSHA citations were
obtained.
The company for whom the pipefitter worked was a mechanical
contracting company that installed systems that convey fluids. It had approximately
60 employees, 30 of whom had the same job title as the victim, journeyman pipefitter.
The company had been in business for 53 years. The pipefitters were represented
by a union. The company was subcontracted to do the work at the site of the
fatality. They had been working there approximately six months.
The victim had been a pipefitter for 20 years. He was 49 years old. He had been working for this company for four years. He had not received specific training from his employer for the task he was doing at the time of the incident. His shift started at 7:00 a.m. and ended at 3:30 p.m. He had not been working overtime. The incident occurred at approximately 3:00 p.m. This employer had never had a fatality occur.
The vice-president of the company had primary responsibility
for safety, and he reported to the president. He delegated safety responsibilities
to the foreman at the jobsite. The vice-president and the site foremen had been
trained in various aspects of safety including confined space entry and fall
protection. Their training was gained through seminars, conferences, classes
and on-the-job. The company had a written safety training program and held weekly
safety meetings. Training was provided by the company, the manufacturers of
the products they used, and consultants. They used toolbox talks from the Mechanical
Contractors Association of America for portions of their training.
The MIOSHA investigation resulted in two violations being issued to the company: one Serious violation for failing to develop, maintain, and coordinate an accident prevention program that included a procedure for the task involved in the fatality; and one Other violation for failing to provide the operator of an aerial work platform with an aerial work platform permit.
INVESTIGATION
On Tuesday, October 29, 2002, at approximately 3:00 p.m., a 49 year-old journeyman pipefitter and his co-worker were standing side by side on a scissors lift preparing to remove 6-inch Victualic grooved end caps from two pipes in preparation for fitting an elbow between the two. They were not wearing fall arrest protection nor were they tied off, because of the type of scissors lift they were working from. The stability of the 30-inch wide scissors lift could have been compromised in the case of a shock load such as could occur with an arrested fall.
The pipes had been pressurized previously with air to 100 psi to test for leaks by the pipefitter. To pressurize the pipes, a test header apparatus was connected to a valve in each of the pipes. The apparatus consisted of a pressure gauge attached between lines connected to the valve on each pipe and a compressed air cylinder. The pipes were pressurized in a separate room approximately 50 feet from where the workers were working. After pressurizing the pipes to the desired psi, the valves were closed and the apparatus removed. Figure 2 shows the pipe valves in the closed position.
Figure 2. Closed Pressure Relief Valves
Figure 3. Coupling (left) and retrofitted grooved cap.
The victim would have been the person to depressurize them. As the pipefitter loosened the bolts on the coupling in front of him in preparation for removing the end cap, the 5-pound, 6-inch diameter cap exploded from the end of the pipe. It struck him in the face with sufficient force to push him over the rail of the scissors lift. He fell 14 feet to the concrete floor below onto his head. When his co-worker heard the noise, he turned to look, but the victim was already on the floor below the lift. Another worker heard the noise, came to investigate and found the victim bleeding profusely from the face and having difficulty breathing. EMS personnel arrived shortly, treated the victim at the site and transported him to a local hospital where emergency treatment was continued. He died eighteen hours later in the hospital.
Figure 1 is a photograph of the pipes on which the men were working with the scissors lift (shown in the retracted position) below. The second pipe from the left is the pipe involved in the fatality. It was recessed into the wall opening from the force of the end cap exploding off of it.
Part of the victim’s responsibility would have included bleeding the air from the pipes before he and his partner removed the caps. The usual practice was to bleed the air from the pipes after 24 hours. These pipes had been pressurized longer than 24 hours before the incident, but there was some question regarding when he had originally pressurized them. These pipes may have been pressurized for three weeks.
The cap that was used to blank the pipes was referred to by several names. It was called a grooved cap, or Vic cap, or grooved plug. These names describe a method of blanking a pipe that consists of bolting a coupling with a gasket in which the cap or plug is seated onto the end of the pipe. The two pipes on the right in Figure 1 are shown with an end cap attached. Figure 3 shows a coupling and a grooved cap retrofitted with a pressure relieving valve. The caps used at the time of the incident did not have pressure relieving valves.
The following safety changes were made before the MIFACE investigation:
CAUSE OF DEATH
The cause of death as stated on the autopsy summary was “head injuries received at approximately 2:45 p.m. on October 20, 2002, when he was struck by the suddenly released cap of a steam pipe from which he had removed the securing bolts, followed by a fall from an aerial lift platform to a concrete floor. There were numerous facial fractures and left-sided brain injuries. He survived approximately 18 hours in the hospital. No other serious injuries nor any sign of disease contributing to death were present either during hospitalization or a postmortem examination.” His heart, right lung, and kidneys were removed for organ donation.
RECOMMENDATIONS/DISCUSSION
In this case the employer did have an accident prevention plan, but the plan did not include a procedure for ensuring that the pipe had been depressurized. At a construction site where it is not possible nor appropriate to observe skilled tradesmen constantly, an accident prevention program that identifies and describes the potential hazards to be encountered during the work serves to highlight and reinforce information that the workers bring to the job. Why the pressure had not been bled off will never be known, but a reminder regarding the procedure at the beginning of the project as part of the accident prevention plan, however elementary it might have seemed to the workers, might have prevented this incident.
Attachment 1 of this report is an example of the type of standard operating procedure developed for this task. Apparently it is not unusual for an air test to be left on for several days. Because the air test apparatus was removed, it would have been appropriate to tag the lines as a reminder that they were pressurized. A red tag on the lines would have been a reminder to the crew that the lines were still under pressure.
The employer’s retrofit of the grooved caps the company now uses was one way to ensure a cap would not be allowed to explode from the end of a pressurized pipe. There are other fittings such as blind flanges that can be purchased to blank a line that stay attached to the pipe until the pressure is bled off as they are being removed. Whichever method is used to guard against a cap exploding from the end of a pressurized line, the most important control is to make every effort and plan to ensure the line is depressurized first.
According to a journeyman pipefitter, apprentice and journeymen pipefitters are taught always to walk down a piping system and open any drains or vents to ensure the line they are penetrating has no pressure on it. Familiarity with a task often leads to a lax attitude regarding the steps to be followed to perform a job safely. Reinforcement of safety training serves to remind experienced workers that they can never become complacent. Appropriate consideration given to the type and value of the training can also indicate to the workers that working safely is viewed as an important element of the job and safety is not simply being given lip service.
REFERENCES
MIFACE (Michigan Fatality and Control Evaluation), Michigan State University (MSU) Occupational & Environmental Medicine, 117 West Fee Hall, East Lansing, Michigan 48824-1315. This information is for educational purposes only. This MIFACE report becomes public property upon publication and may be printed verbatim with credit to MSU. The author of this report is affiliated with Wayne State University. Reprinting cannot be used to endorse or advertise a commercial product or company. All rights reserved. MSU is an affirmative-action, equal opportunity employer. 10/6/03
To contact Michigan State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
APPENDIX 1
OSHA JOB SAFETY ANALYSIS
| To improve the quality of the MIFACE program and our investigation reports, we would like to ask you a few questions regarding this report. | |||
| Please rate the following on a scale of: | |||
| Excellent | Good | Fair | Poor |
| 1 | 2 | 3 | 4 |
| What was your general impression of this MIFACE investigation report? | |||
| Excellent | Good | Fair | Poor |
| 1 | 2 | 3 | 4 |
| Was the report… | Excellent | Good | Fair | Poor |
| Objective? | 1 | 2 | 3 | 4 |
| Clearly written? | 1 | 2 | 3 | 4 |
| Useful? | 1 | 2 | 3 | 4 |
| Were the recommendations … | Excellent | Good | Fair | Poor |
| Clearly written? | 1 | 2 | 3 | 4 |
| Practical? | 1 | 2 | 3 | 4 |
| Useful? | 1 | 2 | 3 | 4 |
| How will you use this report? (Check all that apply) | |
| O | Distribute to employees and/or family members |
| O | Post on bulletin board |
| O | Use in employee training |
| O | File for future reference |
| O | Will not use it |
| O | Other (specify) __________________________________________ |
Thank You!
Please Return To:
MIFACE
Michigan State University
117 West Fee Hall
East Lansing, MI 48824
FAX: 517-432-3606
Comments:
| If you would like to receive e-mail notifications of future MIFACE work-related fatality investigation report summaries, please complete the information below. | |
| Name: __________________________________________ | |
| e-mail address: ___________________________________ | |
| I would like to receive summaries for reports involving: | |
| ___ Construction | ___ Agriculture |
| ___ Manufacturing | ___ All |

![]()

