Introduction
What Is Melanoma?
The Skin
Melanocytes and Moles
Understanding Cancer
Melanoma
Melanoma: Who’s at Risk?
Signs and Symptoms
Dysplastic Nevi
Diagnosis
Staging
Stages of Melanoma
Treatment
Getting a Second Opinion
Preparing for Treatment
Methods of Treatment
Surgery
Chemotherapy
Biological Therapy
Radiation Therapy
Treatment Choices by Stage
Recurrent Melanoma
Side Effects of Treatment
Surgery
Chemotherapy
Biological Therapy
Radiation Therapy
Nutrition
Followup Care
Support for People with Melanoma
The Promise of Cancer Research
How To Do a Skin Self-Exam
National Cancer Institute Booklets
National Cancer Institute Information Resources
Introduction
Melanoma* is the most serious type of cancer of
the skin. Each year in the United
States, more than 53,600 people learn they have melanoma.
In some parts of the world, especially
among Western countries, melanoma is becoming more common every year. In the United States, for example, the
percentage of people who develop melanoma has more than doubled in the past 30
years.
The National Cancer Institute (NCI) has written this booklet (NIH Publication No. 02-1563) to help people
with melanoma and their families and friends better understand this disease.
We hope others will read it as well to learn more about melanoma. This booklet
discusses risks and prevention, symptoms, diagnosis, treatment, and followup
care. It also has information about resources and sources of support to help
patients cope with melanoma.
|
This booklet is about melanoma of the
skin. Melanomas arising in areas
other than the skin (such as intraocular melanoma, which is melanoma
arising in the eye) are not discussed here. Also, two more common and less serious types of skin cancer
(squamous cell and basal cell cancer) are discussed in another NCI booklet,
What You Need To Know About™ Skin Cancer 1.
For other sources of information on intraocular melanoma and
skin cancer, see the “National Cancer Institute Information Resources 2.”
|
Research continues to teach us more about
melanoma. Scientists are learning more
about its causes. They are exploring
new ways to prevent, find, and treat this disease. Because of research, people with melanoma can look forward to a
better quality of life and less chance of dying from this disease.
Information specialists at the NCI's
Cancer Information Service 3
at 1-800-4-CANCER can answer questions about
melanoma and can send NCI materials. They can also send up-to-date
treatment information from NCI’s
PDQ® 4
database. In addition, many NCI publications and fact sheets are
on the Internet at http://www.cancer.gov/publications. People in the United States and its
territories may use this Web site to order publications. This Web site also explains how people
outside the United States can mail or fax their requests for NCI publications.
*Words that may be new to readers appear in italics. The
Dictionary 5 section explains these
terms. Some words in the Dictionary have a
"sounds-like" spelling to show how to pronounce them.
What Is Melanoma?
Melanoma is a type of skin cancer. It begins in cells
in the skin called melanocytes. To understand melanoma, it is helpful to
know about the skin and about melanocytes—what they do, how they grow, and what
happens when they become cancerous.
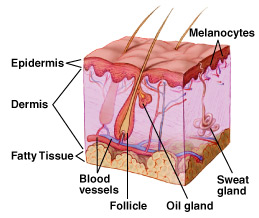
The Skin
The skin is the body’s largest organ.
It protects against heat, sunlight, injury, and infection. It helps regulate body temperature, stores
water and fat, and produces vitamin D.
The skin has two main layers: the outer epidermis
and the inner dermis.
The epidermis is mostly made
up of flat, scalelike cells called squamous
cells. Round cells called basal cells lie under the squamous
cells in the epidermis. The lower part
of the epidermis also contains melanocytes.
The dermis contains blood vessels,
lymph vessels,
hair follicles, and
glands.
Some of these glands produce sweat, which helps regulate body
temperature. Other glands produce sebum,
an oily substance that helps keep the skin from drying out. Sweat and sebum
reach the skin’s surface through tiny openings called pores.
Melanocytes and Moles
Melanocytes produce melanin,
the pigment that gives skin its natural color.
When skin is exposed to the sun, melanocytes produce more pigment,
causing the skin to tan, or darken.
Sometimes, clusters of melanocytes and surrounding
tissue
form noncancerous growths called
moles.
(Doctors also call a mole a nevus;
the plural is nevi.) Moles are very
common. Most people have between 10 and
40 moles. Moles may be pink, tan,
brown, or a color that is very close to the person’s normal skin tone. People who have dark skin tend to have dark
moles. Moles can be flat or
raised. They are usually round or oval
and smaller than a pencil eraser. They
may be present at birth or may appear later on—usually before age 40. They tend to fade away in older people. When moles are surgically removed, they normally
do not return.
Understanding Cancer
Cancer begins in cells, the building blocks that make up
tissues. Tissues make up the organs of the body. Normally, cells grow and divide to form new
cells as the body needs them. When
cells grow old, they die, and new cells take their place.
Sometimes this orderly process goes wrong. New cells form when the body does not need
them, and old cells do not die when they should. These extra cells can form a mass of tissue called a growth or tumor. Not
all tumors are cancer.
Tumors can be benign or
malignant:
Melanoma
Melanoma occurs when
melanocytes (pigment cells) become malignant.
Most pigment cells are in the skin; when melanoma starts in the skin,
the disease is called cutaneous melanoma. Melanoma may also occur in the eye
(ocular melanoma or
intraocular melanoma).
Rarely, melanoma may arise in the meninges,
the digestive tract,
lymph nodes, or other areas
where melanocytes are found. Melanomas that begin in areas other than the
skin are not discussed in this booklet. The Cancer Information Service
(1-800-4-CANCER) can provide information about these types
of melanoma.
Melanoma
is one of the most common cancers. The
chance of developing it increases with age, but this disease affects people of
all ages. It can occur on any skin
surface. In men, melanoma is often
found on the trunk (the area between the shoulders and the hips) or the head
and neck. In women, it often develops
on the lower legs. Melanoma is rare in
black people and others with dark skin.
When it does develop in dark-skinned people, it tends to occur under the
fingernails or toenails, or on the palms or soles.
When melanoma
spreads, cancer cells may show up in nearby lymph nodes. Groups
of lymph nodes are found throughout the body.
Lymph nodes trap bacteria,
cancer cells, or other harmful
substances that may be in the lymphatic system. If the cancer has reached the
lymph nodes, it may mean that cancer cells have spread to other parts of the
body such as the liver, lungs, or brain.
In such cases, the cancer cells in the new tumor are still melanoma
cells, and the disease is called metastatic melanoma, not liver, lung, or brain
cancer.
Melanoma: Who’s at Risk?
No one knows the exact causes of melanoma. Doctors can seldom explain why one
person gets melanoma and another does not.
However, research has shown that people with certain
risk factors are more likely than
others to develop melanoma. A risk factor is anything that increases a
person’s chance of developing a disease. Still, many who do get this
disease have no known risk factors.
Studies have found the following risk factors for melanoma:
-
Dysplastic nevi: Dysplastic
nevi are more likely than ordinary moles to become cancerous. Dysplastic nevi
are common, and many people have a few of these abnormal moles. The risk of
melanoma is greatest for people who have a large number of dysplastic nevi. The
risk is especially high for people with a family history of both dysplastic
nevi and melanoma.
-
Many (more than 50) ordinary moles: Having many moles increases the risk
of developing melanoma.
-
Fair skin: Melanoma occurs more frequently in people who have fair skin
that burns or freckles easily (these people also usually have red or blond hair
and blue eyes) than in people with dark skin. White people get melanoma far
more often than do black people, probably because light skin is more easily
damaged by the sun.
-
Personal history of melanoma or skin cancer: People who have been
treated for melanoma have a high risk of a second melanoma. Some people develop
more than two melanomas. People who had one or more of the common skin cancers
(basal
cell carcinoma or
squamous cell carcinoma) are at
increased risk of melanoma.
-
Family history of melanoma: Melanoma sometimes runs in families. Having
two or more close relatives who have had this disease is a risk factor. About
10 percent of all patients with melanoma have a family member with this
disease. When melanoma runs in a family, all family members should be checked
regularly by a doctor.
-
Weakened
immune system: People whose
immune system is weakened by certain cancers, by drugs given following organ
transplantation, or by
HIV are at increased risk of
developing melanoma.
-
Severe, blistering sunburns: People who have had at least one severe,
blistering sunburn as a child or teenager are at increased risk of melanoma.
Because of this, doctors advise that parents protect children’s skin from
the sun. Such protection may reduce the risk of melanoma later in life.
Sunburns in adulthood are also a risk factor for melanoma.
-
Ultraviolet (UV) radiation:
Experts believe that much of the worldwide increase in melanoma is related to
an increase in the amount of time people spend in the sun. This disease is also
more common in people who live in areas that get large amounts of UV radiation
from the sun. In the United States, for example, melanoma is more common in
Texas than in Minnesota, where the sun is not as strong. UV radiation from the
sun causes premature aging of the skin and skin damage that can lead to
melanoma. Artificial sources of UV radiation, such as sunlamps and tanning
booths, also can cause skin damage and increase the risk of melanoma. Doctors
encourage people to limit their exposure to natural UV radiation and to avoid
artificial sources.
|
Doctors recommend that people take steps to help prevent and reduce the risk of
melanoma caused by UV radiation:
-
Avoid exposure to the midday sun (from 10 a.m. to 4 p.m.) whenever possible.
When your shadow is shorter than you are, remember to protect yourself from the
sun.
-
If you must be outside, wear long sleeves, long pants, and a hat with a wide
brim.
-
Protect yourself from UV radiation that can penetrate light clothing,
windshields, and windows.
-
Protect yourself from UV radiation reflected by sand, water, snow, and ice.
-
Help protect your skin by using a lotion, cream, or gel that contains
sunscreen. Many doctors believe
sunscreens may help prevent melanoma, especially sunscreens that reflect,
absorb, and/or scatter both types of ultraviolet radiation. These sunscreen
products will be labeled with “broad-spectrum coverage.” Sunscreens
are rated in strength according to a sun protection factor (SPF). The higher
the SPF, the more sunburn protection is provided. Sunscreens with an SPF value
of 2 to 11 provide minimal protection against sunburns. Sunscreens with an SPF
of 12 to 29 provide moderate protection. Those with an SPF of 30 or higher
provide the most protection against sunburn.
-
Wear sunglasses that have UV-absorbing lenses. The label should specify that
the lenses block at least 99 percent of
UVA and
UVB radiation. Sunglasses can
protect both the eyes and the skin around the eyes.
|
People who are concerned about developing melanoma should talk with their doctor
about the disease, the symptoms to watch for, and an appropriate schedule for
checkups. The doctor’s advice will be based on the person’s
personal and family history, medical history, and other risk factors.
Signs and Symptoms
Often,
the first sign of melanoma is a change in the size, shape, color, or feel of an
existing mole. Most melanomas have a
black or blue-black area. Melanoma also
may appear as a new mole. It may be
black, abnormal, or “ugly looking.”
If you have a question or concern about something on your skin, see
your doctor. Do not use the following pictures to try to diagnose it
yourself. Pictures are useful examples, but they cannot take the place of
a doctor’s examination.
Thinking of “ABCD” can help you remember what to watch for:
Asymmetry—The shape
of one half does not match the other.
Border—The edges are often ragged, notched, blurred, or
irregular in outline; the pigment may spread into the surrounding skin.
Color—The color is uneven.
Shades of black, brown, and tan may be present. Areas of white, grey, red, pink, or blue
also may be seen.
Diameter—There is a change in size, usually an
increase. Melanomas are usually larger
than the eraser of a pencil (1/4 inch or 5 millimeters).
Melanomas can vary greatly in how
they look. Many show all of the ABCD
features. However, some may show
changes or abnormalities in only one or two of the ABCD features.
Melanomas in an early stage may be found when an existing mole
changes slightly, for example, when a new black area forms. Newly formed fine scales and itching in a
mole also are common symptoms of early melanoma. In more advanced melanoma, the texture of the mole may
change. For example, it may become hard
or lumpy. Melanomas may feel different
from regular moles. More advanced
tumors may itch, ooze, or bleed. But
melanomas usually do not cause pain.
A skin examination is often part of a routine checkup by a
health care provider. People also can
check their own skin for new growths or other changes. (The
“How To Do a Skin Self-Exam 6” section
has a simple guide on how to do this skin self-exam.) Changes in the skin,
such as a change in a mole, should be reported to the health care provider
right away. The person may be referred to a
dermatologist,
a doctor who specializes in diseases of the skin.
Melanoma
can be cured if it is diagnosed and treated when the tumor is thin and has not
deeply invaded the skin. However, if a
melanoma is not removed at its early stages, cancer cells may grow downward
from the skin surface and invade healthy tissue. When a melanoma becomes thick and deep, the disease often spreads
to other parts of the body and is difficult to control.
People who have had melanoma have
a high risk of developing a new melanoma.
People at risk for any reason should check their skin regularly and have
regular skin exams by a health care provider.
Dysplastic Nevi
Some people have certain abnormal-looking moles (called dysplastic
nevi or atypical moles) that are more likely than normal moles to
develop into melanoma. Most people with dysplastic nevi have just a
few of these abnormal moles; some people have many. People with
dysplastic nevi and their health care provider should examine these
moles regularly to watch for changes. (Additional information about
moles and dysplastic nevi and melanoma risk is available in the NCI booklet
What You Need To Know About™ Moles and Dysplastic Nevi 7.)
Dysplastic nevi often look very much like melanoma. Doctors with
special training in skin diseases are in the best position to decide whether an
abnormal-looking mole should be closely watched or removed and checked for
cancer.
In some families, many members
have a large number of dysplastic nevi, and some have had melanoma. Members of these families have a very high
risk of melanoma. Doctors often recommend
that they have frequent checkups (every 3 to 6 months) so that any problems can
be detected early. The doctor may take
pictures of a person’s skin to help show when changes occur.
Diagnosis
If the doctor suspects that a spot on the skin is melanoma, the patient
will need to have a biopsy. A biopsy is the only way to make a
definite diagnosis. In this procedure,
the doctor tries to remove all of the suspicious-looking growth. This is an excisional biopsy. If the growth is too large to be removed
entirely, the doctor removes a sample of the tissue. The doctor will never "shave off" or cauterize a growth that might be
melanoma.
A biopsy can usually be done in the doctor’s office using
local anesthesia. A
pathologist
then examines the tissue under a microscope to check for cancer cells. Sometimes it is helpful for more than one
pathologist to check the tissue for cancer cells.
|
A person who needs a biopsy may want to ask the doctor
the following questions:
Why do I need a biopsy?
How long will it take? Will it hurt?
Will the entire tumor be removed?
What side effects can I expect?
How soon will I know the results?
If I do have cancer, who will talk to me about
treatment? When?
|
Staging
If the
diagnosis is melanoma, the doctor needs to learn the extent, or stage, of the
disease before planning treatment. Staging is a careful attempt to learn how
thick the tumor is, how deeply the melanoma has invaded the skin, and whether
melanoma cells have spread to nearby lymph nodes or other parts of the
body. The doctor may remove nearby
lymph nodes to check for cancer cells.
(Such surgery may be
considered part of the treatment because removing cancerous lymph nodes may
help control the disease.) The doctor
also does a careful physical exam and, if the tumor is thick, may order chest x-rays, blood tests, and scans of the liver,
bones, and brain.
Stages of Melanoma
The following stages are used for melanoma:
Stage 0: In stage 0,
the melanoma cells are found only in the outer layer of skin cells and have not
invaded deeper tissues.
Stage I: Melanoma in stage I is thin:
The tumor is no more than 1
millimeter (1/25 inch) thick. The outer
layer (epidermis) of skin may appear scraped.
(This is called an ulceration).
Or, the tumor is between 1 and 2
millimeters (1/12 inch) thick. There is
no ulceration.
The melanoma cells have not spread to nearby lymph
nodes.
Stage II: The tumor is at least 1
millimeter thick:
The tumor is between 1 and 2
millimeters thick. There is ulceration.
Or, the thickness of the tumor is
more than 2 millimeters. There may be
ulceration.
The melanoma cells have not spread to nearby lymph
nodes.
Stage III: The melanoma cells have
spread to nearby tissues:
The
melanoma cells have spread to one or more nearby lymph nodes.
Or, the
melanoma cells have spread to tissues just outside the original tumor but not
to any lymph nodes.
Stage IV: The melanoma cells have
spread to other organs, to lymph nodes, or to skin areas far away from the
original tumor.
Recurrent: Recurrent disease means
that the cancer has come back (recurred) after it has been treated. It may
have come back in the original site or in another part of the body.
 |
Treatment
The doctor can describe treatment choices and discuss the
results expected with each treatment option.
The doctor and patient can work together to develop a treatment plan
that fits the patient’s needs. Treatment
for melanoma depends on the extent of the disease, the patient’s age and
general health, and other factors.
People with melanoma are often
treated by a team of specialists. The
team may include a dermatologist,
surgeon,
medical oncologist,
radiation oncologist, and
plastic surgeon.
Getting a Second Opinion
Before starting treatment, the patient
might want a second opinion about the diagnosis and the treatment plan. Some insurance companies require a second
opinion; others may cover a second opinion if the patient or doctor requests
it.
There are a number of ways to find a
doctor for a second opinion:
The patient’s doctor may
refer the patient to one or more specialists.
At cancer centers, several specialists often work together as a team.
The Cancer Information Service, at 1-800-4-CANCER, can
tell callers about nearby treatment centers.
A local or state medical society, a
nearby hospital, or a medical school can usually provide the names of
specialists.
The American Board of Medical Specialties (ABMS) has a list of doctors who have met certain education and training requirements and have passed specialty examinations. The Official ABMS Directory of Board Certified Medical Specialists lists doctors' names along with their specialty and their educational background. The directory is available in most public libraries. Also, ABMS offers this information on the Internet at http://www.abms.org. (Click on "Who's Certified.")
Preparing for Treatment
People with melanoma often want to take an active part in making decisions
about their medical care. They want to learn all they can about their disease
and their treatment choices. However, shock and stress after a diagnosis of a
melanoma can make it hard to think of everything to ask the doctor. It often
helps to make a list of questions before an appointment. To help remember
what the doctor says, patients may take notes or ask whether they may use a
tape recorder. Some also want to have a family member or friend with them
when they talk to the doctor—to take part in the discussion, to take
notes, or just to listen.
|
These
are some questions a person may want to ask the doctor before treatment
begins:
What is
my diagnosis?
What is the stage of my
disease?
What
are my treatment choices? Which do
you recommend for me? Why?
What
are the benefits of each kind of treatment?
What
are the risks and possible
side effects
of each treatment?
How
will I feel after surgery?
If I
have pain, how will it be controlled?
Will I
need more treatment after surgery?
Will there be a scar? Will I need a
skin graft or
plastic surgery?
What is the treatment likely to cost?
Will treatment affect my normal activities?
If so, for how long?
How often will I need checkups?
Would a
clinical trial (research study)
be appropriate for me? Can you help
me find one?
|
People do not need to ask all of their questions or understand all of the
answers at one time. They will have other chances to ask the doctor to explain
things that are not clear and to ask for more information.
Methods of Treatment
People with melanoma may have surgery,
chemotherapy,
biological therapy, or
radiation therapy.
Patients may have a combination of treatments.
At any stage of disease, people with melanoma may have
treatment to control pain and other symptoms of the cancer, to relieve
the side effects of therapy, and to ease emotional and practical problems.
This kind of treatment is called
symptom management,
supportive care, or
palliative care.
The doctor is the best person to describe the treatment
choices and discuss the expected results.
A patient may want to talk to the doctor
about taking part in a clinical trial, a research study of new treatment
methods. The section on
“The Promise of Cancer Research 8”
has more information about clinical trials.
Surgery
Surgery is the usual
treatment for melanoma. The surgeon
removes the tumor and some normal tissue around it. This procedure reduces the chance that cancer cells will be left
in the area. The width and depth of
surrounding skin that needs to be removed depends on the thickness of the
melanoma and how deeply it has invaded the skin:
The doctor may be able to completely remove a very thin
melanoma during the biopsy. Further
surgery may not be necessary.
If the melanoma was not completely removed during the
biopsy, the doctor takes out the remaining tumor. In most cases, additional surgery is performed to remove
normal-looking tissue around the tumor (called the
margin) to make sure
all melanoma cells are removed. This is often necessary, even
for thin melanomas. If the melanoma is
thick, the doctor may need to remove a larger margin of tissue.
If a large
area of tissue is removed, the surgeon may do a skin graft. For this procedure, the doctor uses skin
from another part of the body to replace the skin that was removed.
Lymph nodes
near the tumor may be removed because cancer can spread through the lymphatic
system. If the pathologist finds cancer
cells in the lymph nodes, it may mean that the disease has also spread to other
parts of the body. Two procedures are
used to remove the lymph nodes:
Sentinel
lymph node biopsy—The sentinel lymph node biopsy is done after the
biopsy of the melanoma but before the wider excision
of the tumor. A radioactive substance
is injected near the melanoma. The
surgeon follows the movement of the substance on a computer screen. The first lymph node(s) to take up the
substance is called the sentinel
lymph node(s). (The imaging
study is called lymphoscintigraphy. The procedure to identify the sentinel
node(s) is called sentinel
lymph node mapping.) The
surgeon removes the sentinel node(s) to check for cancer cells.
If a
sentinel node contains cancer cells, the surgeon removes the rest of the lymph
nodes in the area. However, if a
sentinel node does not contain cancer cells, no additional lymph nodes are
removed.
Lymph node dissection—The
surgeon removes all the lymph nodes in the area of the melanoma.
Therapy may be given after surgery to kill cancer cells that remain in
the body. This treatment is called
adjuvant therapy. The
patient may receive biological therapy.
Surgery is
generally not effective in controlling melanoma that has spread to other parts
of the body. In such cases, doctors may
use other methods of treatment, such as chemotherapy, biological therapy,
radiation therapy, or a combination of these methods.
Chemotherapy
Chemotherapy,
the use of drugs to kill cancer cells, is sometimes used to treat
melanoma. The drugs are usually given
in cycles: a treatment period followed
by a recovery period, then another treatment period, and so on. Usually a patient has chemotherapy as an
outpatient (at the hospital, at the doctor’s office, or at home). However, depending on which drugs are given
and the patient’s general health, a short hospital stay may be needed.
People with melanoma may receive chemotherapy in one of the
following ways:
By mouth or injection—Either way, the
drugs enter the bloodstream and travel throughout the body.
Isolated limb perfusion
(also called isolated arterial perfusion)—For melanoma on an arm or leg,
chemotherapy drugs are put directly into the bloodstream of that limb. The flow
of blood to and from the limb is stopped for a while. This allows most of the
drug to reach the tumor directly. Most of the chemotherapy remains in that
limb.
The drugs may be heated before injection. This type of chemotherapy is called
hyperthermic perfusion.
Biological Therapy
Biological therapy (also called
immunotherapy) is a form of treatment that uses the body’s immune system,
either directly or indirectly, to fight cancer or to reduce side effects caused
by some cancer treatments. Biological
therapy for melanoma uses substances called cytokines. The body normally produces cytokines in
small amounts in response to infections and other diseases. Using modern laboratory techniques,
scientists can produce cytokines in large amounts. In some cases, biological therapy given after surgery can help
prevent melanoma from recurring. For
patients with metastatic melanoma or a high risk of recurrence, interferon
alpha and interleukin-2 (also called IL-2 or aldesleukin) may be recommended
after surgery.
Radiation Therapy
Radiation therapy
(also called radiotherapy) uses high-energy rays to kill cancer cells. A large machine directs radiation at the
body. The patient usually has treatment at a hospital
or clinic, five days a week for several weeks.
Radiation therapy may be used to help control melanoma that has spread
to the brain, bones, and other parts of the body. It may shrink the tumor and relieve symptoms.
Treatment Choices by Stage
The following are brief descriptions of the
treatments most often used for each stage.
(Other treatments may sometimes be appropriate.)
Stage 0
People
with Stage 0 melanoma may have minor surgery to remove the tumor and some of
the surrounding tissue.
Stage I
People
with Stage I melanoma may have surgery to remove the tumor. The surgeon may also remove as much as 2
centimeters (3/4 inch) of tissue around the tumor. To cover the wound, the patient may have skin grafting.
Stage II or Stage III
People
with Stage II or Stage III melanoma may have surgery to remove the tumor. The surgeon may also remove as much as 3
centimeters (1 1/4 inches) of nearby tissue.
Skin grafting may be done to cover the wound. Sometimes the surgeon removes nearby lymph nodes.
Stage IV
People with Stage IV melanoma often
receive palliative care. The goal of
palliative care is to help the patient feel better—physically and
emotionally. This type of treatment is
intended to control pain and other symptoms and to relieve the side effects of
therapy (such as nausea), rather than to extend life.
The patient may have one of the following:
Surgery
to remove lymph nodes that contain cancer cells or to remove tumors that have
spread to other areas of the body
Radiation therapy, biological therapy, or
chemotherapy to relieve symptoms
People with advanced melanoma can find
helpful information in the National Cancer Institute booklet Pain Control: A Guide for People with Cancer and Their Families 9.
Recurrent Melanoma
Treatment
for recurrent melanoma depends on where the cancer came back, which treatments
the patient has already received, and other factors. As with Stage IV melanoma, treatment usually cannot cure melanoma
that recurs. Palliative care is often
an important part of the treatment plan.
Many patients have palliative care to ease their symptoms while they are
getting anticancer treatments to slow the progress of the disease. Some receive only palliative care to improve
their quality of life by
easing pain, nausea, and other symptoms.
The patient may have one of the
following:
Surgery
to remove the tumor
Radiation
therapy, biological therapy, or chemotherapy to relieve symptoms
Heated
chemotherapy drugs injected directly into the tumor
Side Effects of Treatment
Because treatment may damage healthy cells and tissues,
unwanted side effects sometimes occur.
These side effects depend on many factors, including the location of the
tumor and the type and extent of the treatment. Side effects may not be the same for each person, and they may
even change from one treatment session to the next. Before treatment starts, the health care team will explain possible
side effects and suggest ways to help the patient manage them.
The NCI provides helpful booklets about cancer treatments
and coping with side effects, such as
Radiation Therapy and You 10,
Chemotherapy and You 11,
and Eating Hints for Cancer Patients 12. See the sections
“National Cancer Institute Information Resources 2”
and “National Cancer Institute Booklets 13”
for other sources of information about side effects.
Surgery
The side effects of surgery depend mainly
on the size and location of the tumor and the extent of the operation. Although patients may have some pain during
the first few days after surgery, this pain can be controlled with
medicine. People should feel free to
discuss pain relief with the doctor or nurse.
It is also common for patients to feel tired or weak for a while. The length of time it takes to recover from
an operation varies for each patient.
Scarring may also be a concern for some
patients. To avoid causing large scars,
doctors remove as little tissue as they can (while still protecting against
recurrence). In general, the scar from
surgery to remove an early stage melanoma is a small line (often 1 to 2 inches
long), and it fades with time. How
noticeable the scar is depends on where the melanoma was, how well the person
heals, and whether the person develops raised scars called
keloids.
When a tumor is large and thick, the doctor must remove more surrounding
skin and other tissue (including muscle).
Although skin grafts reduce scarring caused by the removal of large
growths, these scars will still be quite noticeable.
Surgery to remove the lymph nodes from the underarm or groin may damage
the lymphatic system and slow the flow of
lymphatic fluid in the
arm or leg. Lymphatic fluid may build up in a limb and cause swelling
(lymphedema). The doctor
or nurse can suggest exercises or other ways to reduce swelling if it
becomes a problem. Also, it is harder for the body to fight
infection in a limb after nearby lymph nodes have been removed, so the patient
will need to protect the arm or leg from cuts, scratches, bruises, insect
bites, or burns that may lead to infection.
If an infection does develop, the patient should see the doctor right
away.
Chemotherapy
The side effects of chemotherapy depend mainly on the specific drugs
and the dose. In general, anticancer drugs affect cells
that divide rapidly, especially:
Blood cells:
These cells fight infection, help the blood to clot, and carry oxygen to
all parts of the body. When drugs
affect blood cells, patients are more likely to get infections, may bruise or
bleed easily, and may feel very weak and tired.
Cells in hair roots: Chemotherapy can lead to hair loss. The hair grows back, but the new hair may be somewhat different
in color and texture.
Cells that line the digestive tract: Chemotherapy can cause poor appetite, nausea
and vomiting, diarrhea, or mouth and lip sores. Many of these side effects can be controlled with drugs.
Biological Therapy
The side
effects of biological therapy vary with the type of treatment. These treatments may cause flu-like
symptoms, such as chills, fever, muscle aches, weakness, loss of appetite,
nausea, vomiting, and diarrhea. Patients
may also get a skin rash. These
problems can be severe, but they go away after treatment stops.
Radiation Therapy
The side effects of radiation
therapy depend on the amount of radiation given and the area being
treated. Side effects that may occur in
the treated area include red or dry skin and hair loss. Radiation therapy also may cause
fatigue. Although the side effects of
radiation therapy can be unpleasant, the doctor can usually treat or control
them. It also helps to know that, in most
cases, side effects are not permanent.
Nutrition
People with melanoma may not feel like eating, especially if
they are uncomfortable or tired. Also,
the side effects of treatment, such as poor appetite, nausea, or vomiting, can
be a problem. Foods may taste
different. Nevertheless, patients
should try to eat well during cancer therapy.
They need enough calories to maintain a good weight and protein to keep
up strength. Good nutrition often helps
people with cancer feel better and have more energy.
The doctor, dietitian, or other health care provider can suggest ways
to maintain a healthy diet. Patients and their families may want to read
the National Cancer Institute booklet
Eating Hints for Cancer Patients 12,
which contains many useful ideas and recipes. The
“National Cancer Institute Booklets 13”
section tells how to get this publication.
Followup Care
Melanoma patients have a high risk of developing new melanomas. Some
also are at risk of a recurrence of the original melanoma in nearby skin
or in other parts of the body.
To increase the chance of detecting a new or recurrent melanoma as
early as possible, patients should follow their doctor’s schedule
for regular checkups. It is especially important for patients who have
dysplastic nevi and a family history of melanoma to have frequent
checkups. Patients also should examine their skin monthly (keeping in mind
the “ABCD” guidelines in the
“Signs and Symptoms 14”
section, and the skin self-exam described in
“How To Do a Skin Self-Exam 6”).
They should follow their doctor’s advice about how to reduce their
chance of developing another melanoma. General information about reducing
the risk of melanoma is described in the
“Melanoma: Who’s at Risk? 15” section.
The chance of recurrence is greater for patients whose melanoma was
thick or had spread to nearby tissue than for patients with very thin
melanomas. Followup care for those who have a high risk of recurrence
may include x-rays, blood tests, and scans of the chest, liver, bones,
and brain.
The NCI has prepared a booklet for people who have completed their
treatment to help answer questions about followup care and other concerns.
Facing Forward Series: Life After Cancer Treatment 16
provides tips for getting the most out of medical visits. It describes the
kinds of help people may need.
|
A person who has been treated for melanoma may want to
ask the doctor the following questions:
How
often should I have checkups?
What
special precautions should I take to avoid sun exposure?
Are
my family members at risk of melanoma?
Should they schedule an appointment with their doctor for an
examination?
|
Support for People with Melanoma
Living with a serious disease such as melanoma is not
easy. Some people find they need help
coping with the emotional and practical aspects of their disease. Support groups can help. In these groups, patients or their family
members get together to share what they have learned about coping with the
disease and the effects of treatment.
Patients may want to talk with a member of their health care team about
finding a support group. Groups may
offer support in person, over the telephone, or on the Internet.
People living with melanoma may worry about caring for their
families, keeping their jobs, or continuing daily activities. Concerns about treatments and managing side
effects, hospital stays, and medical bills also are common. Doctors, nurses, and other members of the
health care team can answer questions about treatment, working, or other
activities. Meeting with a social worker,
counselor, or member of the clergy can be helpful to those who want to talk about
their feelings or discuss their concerns.
Often, a social worker can suggest resources for financial aid,
transportation, home care, or emotional support.
The Cancer Information Service at 1-800-4-CANCER can send publications and provide information to help
patients and their families locate programs and services.
The Promise of Cancer Research
Doctors all over the country are
conducting many types of clinical trials. These are research studies in which
people take part voluntarily. Studies include
new ways to treat melanomas. Research
already has led to advances, and researchers continue to search for more
effective approaches.
Patients who join these studies
have the first chance to benefit from treatments that have shown promise in
earlier research. They also make an
important contribution to medical science by helping doctors learn more about
the disease. Although clinical trials
may pose some risks, researchers take very careful steps to protect their
patients.
Researchers are testing new anticancer drugs. They are looking at combining
chemotherapy with radiation therapy. Other studies are combining chemotherapy
with biological therapy. Scientists also are studying several cancer
vaccines and a type of
gene therapy designed to help
the immune system kill cancer cells.
Patients who are interested in being part of a clinical
trial should talk with their doctor. They may want to read the NCI booklet Taking Part in Cancer Treatment Research Studies 17. It explains how clinical trials are carried out and explains their possible benefits and risks. NCI’s Web site
includes a section on clinical trials at
http://www.cancer.gov/clinicaltrials.
This section of the Web site provides
general information about clinical trials.
It also offers detailed information about ongoing studies of melanoma
treatment by linking to PDQ®, a cancer information database developed
by the NCI. The Cancer Information Service at
1-800-4-CANCER can answer questions and provide information
from the PDQ database.
How To Do a Skin Self-Exam
Your doctor or nurse may recommend that you do a regular
skin self-exam. If your doctor has taken
photos of your skin, comparing your skin to the photos can help you check for
changes.
The best time to do a skin self-exam is after a shower or
bath. You should check your skin in a
well-lighted room using a full-length mirror and a hand-held mirror. It’s best to begin by learning where your
birthmarks, moles, and blemishes are and what they usually look and feel
like.
Check for anything new:
A new mole (that looks abnormal)
A change in the size, shape, color, or texture of a
mole
A sore that does not heal
Check yourself from head to toe. Don’t forget to check all areas of the skin, including the back,
the scalp, between the buttocks, and the genital area.
Look at your face, neck, ears, and scalp. You may want to use a comb or a blow dryer to move your hair so that you can see better. You also may want to have a relative or friend check through your hair because this is difficult to do yourself. Look at the front and back of your body in the mirror, then raise your arms and look at your left and right sides. Bend your elbows and look carefully at your fingernails, palms, forearms (including the undersides), and upper arms. Examine the back, front, and sides of your legs. Also look between your buttocks and around your genital area. Sit and closely examine your feet, including the toenails, the soles, and the spaces between the toes.
By checking your skin regularly, you will become familiar
with what is normal for you. It may be
helpful to record the dates of your skin exams and to write notes about the way
your skin looks. If you find anything
unusual, see your doctor right away.
National Cancer Institute Booklets
National
Cancer Institute (NCI) publications can be ordered by writing to the address
below, and some can be viewed and downloaded from
http://www.cancer.gov/publications
on the Internet.
Publications Ordering Service
National Cancer Institute
Suite 3036A
6116 Executive Boulevard, MSC 8322
Bethesda, MD 20892-8322
In addition, people in the United States and its territories may order
these and other NCI booklets by calling the Cancer Information Service at
1-800-4-CANCER. They may also order many NCI publications
on-line at http://www.cancer.gov/publications.
See the complete index of What You Need To Know About™ Cancer 18 publications.
Booklets About Skin Conditions
What You Need To Know About™ Moles and Dysplastic Nevi 7
What You Need To Know About™ Skin Cancer 1
Booklets About Cancer Treatment
Booklets About Living With Cancer
Booklets About Cancer Research
National Cancer Institute Information Resources
You may want more information for yourself, your family, and your doctor. The following National Cancer Institute (NCI) services are available to help you.
Cancer Information Service 3 (CIS)
Provides accurate, up-to-date information on cancer to patients and their families, health professionals, and the general public. Information specialists translate the latest scientific information into understandable language and respond in English, Spanish, or on TTY equipment.
Toll-free: 1-800-4-CANCER (1-800-422-6237)
TTY (for deaf and hard of hearing callers): 1-800-332-8615
The NCI's Cancer.gov™ Web site provides information from numerous
NCI sources. It offers current information on cancer prevention, screening,
diagnosis, treatment, genetics, supportive care, and ongoing clinical trials.
It also provides information about NCI's research programs and funding
opportunities, cancer statistics, and the Institute itself. Cancer.gov can be accessed at
http://www.cancer.gov on the Internet.
Cancer.gov also provides live, online assistance through LiveHelp.
Information specialists are available Monday through Friday from 9:00 AM
to 10:00 PM Eastern Time. LiveHelp is at
http://www.cancer.gov on the Internet.
|