Publications and Information Products
Information Sheet
October 2008
NCHS Data on Racial and Ethnic Disparities
PDF version 101 KB
Page Content
About NCHS
Data on Racial and Ethnic Disparities
Examples of NCHS Data
Race and Ethnicity Data Sources
Challenges and Future Opportunities
About NCHS
The CDC's National Center for Health Statistics (NCHS) is the nation's principal health statistics agency, providing data to identify and address health issues. NCHS compiles statistical information to help guide public health and health policy decisions.
Collaborating with other public and private health partners, NCHS employs a variety of data collection mechanisms to obtain accurate information from multiple sources. This process provides a broad perspective to help us understand the populations' health, influences on health, and health outcomes.
Data on Racial and Ethnic Disparities
Improving the health of racial and ethnic minorities in the United States continues to be a public health priority. Despite decades of effort, disparities persist, and changes in the racial and ethnic composition of the population have important consequences for the Nation's health. NCHS has long been a resource for data that document racial and ethnic disparities in health status, health insurance, access to care, and other aspects of health. Virtually every major report and initiative on racial and ethnic health disparities draws heavily on NCHS' core data systems.
Examples of NCHS Data
Life expectancy is a summary measure often used to gauge the overall health of a population. Life expectancy in 2005 remained the same as in 2004; life expectancy at birth was 77.8 years for all races. White females had the highest life expectancy (80.8 years) followed by black females (76.5 years), white males (75.7 years) and black males (69.5 years). Between 2004 and 2005, the only gain in life expectancy among the four race/sex groups was for black women (0.2 years).
There are large disparities in infant mortality rates. The higher rate for non-Hispanic black infants is of particular concern. In 2005 the U.S. infant mortality rate was 6.86 infant deaths per 1,000 live births, statistically unchanged from 2004. The rates ranged from 4.89 deaths per 1,000 live births for Asian or Pacific Islander mothers to 13.63 for non-Hispanic black mothers.
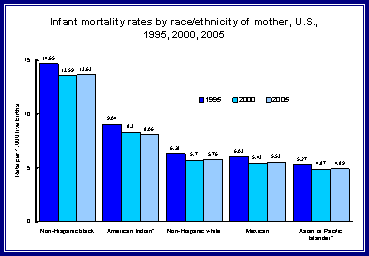
*Includes persons of Hispanic and
non-Hispanic origin.
Source: National Vital Statistics Reports, Infant Mortality Statistics from
the 2005 Period Linked Birth/Infant Death Data Set. Vol 57, Number 2.
Health insurance is an important determinant of access to health care. Access to health care, which includes having a usual source of care, is important for preventive care and prompt treatment of illness and injury.
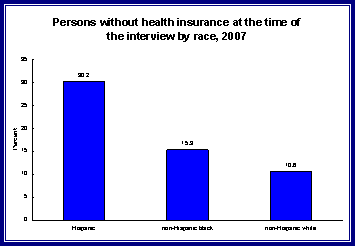
Source: National Health Interview Survey,
2007
Data from 2007 show that Hispanics (30.2 percent) and non-Hispanic blacks (15.3 percent), were more likely to lack health insurance at the time of the interview than non-Hispanic whites (10.6 percent).
NCHS data on utilization of health care services show that in 2006 visit rates per 100 persons differed by race:
- The visit rate to office-based physicians was higher for whites (323.9 visits per 100 persons) than for Asians (295.5 visits per 100 persons), and blacks (235.4 visits per 100 persons).
- The visit rate to hospital outpatient departments for blacks (63.5 visits per 100 persons) was more than double the rate for whites (31.3 visits per 100 persons) and Asians (20.4 visits per 100 persons).
- The emergency department visit rate for blacks (79.9 visits per 100 persons) was more than double the rate for whites (36.1 visits per 100 persons). The visit rate for Asians (18.2 visits per 100 persons) was considerably lower than other racial groups.
Black patients visit the emergency department within 7 days of discharge from the hospital more often than whites (124.3 visits per 1,000 discharges among blacks compared with 84.4 visits per 1,000 discharges among whites). This higher rate might indicate differences in inpatient care or follow-up care among black and white patients.
Overweight and obesity are associated with increased risk of a number of conditions, including diabetes, cardiovascular disease, hypertension, and certain cancers, and with an increased risk of disability. Obesity is associated with a modestly elevated risk of all-cause mortality.
Recent data show racial and ethnic obesity disparities continue for women but not for men. Among women 60 years of age and older, 61 percent of non-Hispanic black were obese compared with 32 percent of non-Hispanic white women and 37 percent of Mexican American women.
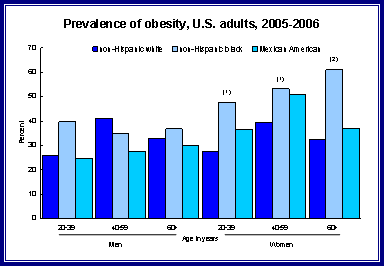
(1) significantly different from the
non-Hispanic white population
(2) significantly different from the non-Hispanic white and Mexican-American
population.
NOTE: obesity is defined as body mass index > 30
Source: National Health and Nutrition Examination Survey, 2005-2006
Race and Ethnicity Data Sources
NCHS employs a variety of data collection mechanisms to obtain accurate information from multiple sources. They include:
- National Vital Statistics System - collects information from birth and death certificates in all 50 states and the District of Columbia, including detailed race/ethnicity characteristics. Because all births and deaths are included in this database, it provides the detail needed for research on disparities. (http://www.cdc.gov/nchs/nvss.htm)
- National Health Interview Survey (NHIS) - obtains information on the nation's health status through confidential household interviews that measure: health status and disability, selected conditions, insurance coverage, access to care, use of health services, immunizations, health behaviors, injury, and the ability to perform daily activities. (http://www.cdc.gov/nchs/nhis.htm)
- National Health Care Surveys - a family of health care provider surveys, obtaining information about the facilities that supply health care, the services rendered, and the characteristics of the patients served. NHCS surveys hospitals, office-based physician practices, emergency and outpatient departments, ambulatory surgery centers, nursing homes, and home health and hospice agencies. These surveys provide a picture of how the delivery system works, and provide an opportunity to learn about patients, their illnesses, and treatments. (http://www.cdc.gov/nchs/nhcs.htm)
- National Health and Nutrition Examination Survey - collects information about the health and diet of people in the U.S. NHANES is unique in that it combines a home interview with physical examinations and laboratory tests conducted in a Mobile Examination Center. NHANES can directly measure conditions and provide reliable information on health conditions regardless of whether the survey respondent is aware of them. (http://www.cdc.gov/nchs/nhanes.htm)
Challenges and Future Opportunities
- Improve "real-time" availability of vital statistics data by encouraging states to fully automate their birth, death and fetal death reporting systems and by re-engineeering the national vital statistics to promote timely and relevant reporting on disparities in mortality and natality.
- Improve usefulness and accessibility of NHIS data by continuous improvements in data quality, relevance, reporting, and timeliness. Major projects include enhanced Web access for both current and historic NHIS data. The NHIS is the nation's largest national household health survey, providing a rich resource for analysis of racial and ethnic populations.
- Expand sample sizes in the health care surveys to include more patients from among priority populations such as racial and ethnic minorities and rural communities. This would permit more accurate assessment of disparities in health care, including those related to source of payment.
- Expand the ability to assess the health of racial and ethnic populations through the Community Health and Nutrition Examination Survey, a smaller model of the National Health and Nutrition Examination Survey. This effort is an efficient mechanism for targeted studies of specific sub-populations, allowing us to systematically fill gaps in knowledge through examination studies.
Page Last Modified: November 20, 2008
Data Source: CDC/National Center for Health Statistics
National Center for Health
Statistics
3311 Toledo Road
Hyattsville, MD 20782
Phone:
1-800-232-4636
nchsquery@cdc.gov
Centers for Disease Control and Prevention, 1600 Clifton Rd, Atlanta, GA 30333, U.S.A
Tel: (404) 639-3311 / Public Inquiries: (404) 639-3534 / (800) 311-3435