 |  |  |  |  | ||||
 | |||
| Setup Instructions |
| Rural
Mental Health in the WICHE West: Meeting Workforce Demands through
Regional Partnership
This publication
was supported through contract #:03H11630801D
APPENDICES Rural Mental Health in the WICHE West: The Western Interstate Commission for Higher Education (WICHE) comprises America's western most rural States, and the professional shortages faced in the frontier areas of the West create a critical barrier to effectively meeting the mental health care needs of the region. To share and gain perspectives on workforce shortages in the West, the WICHE Mental Health Program consulted with leaders in the mental health field and higher education, as well as legislators from WICHE member States. The product of these consultations and shared knowledge is a broader understanding of the national, regional, and State contexts regarding rural/frontier mental health workforce shortage issues and potential avenues for addressing them. Several of these important issues are:
One potential path for accomplishing these tasks is through partnerships with and programs in higher education, such as those currently offered by WICHE. WICHE is a Federally chartered Interstate Compact for higher education and serves a simple, straightforward mission: to provide the citizens of the member States with expanded access to high-quality postsecondary education, and to do so by promoting innovation, cooperation, resource sharing and sound public policy among our States and institutions. WICHE does so not for the sake of western higher education, but for the sake of the region's social, economic, and civic life, which will thrive only if we provide broad access to excellent higher education. Specific WICHE programs that may be of value to member States will be discussed in subsequent sections of this report. However, in addition to the educational side of WICHE is the Mental Health Program, which is a technical assistance (TA) and evaluation center, with nearly a half-century of expertise in responding to behavioral health issues, collaborating with experts in the field to identify and disseminate best practices in mental health and supporting public behavioral health systems in program evaluation, clinical performance measurement and data driven decision support. Mental Health Workforce Development - Throughout the past 50 years the WICHE Mental Health Program has been actively engaged in mental health workforce development activities for the West. The program was funded for over a decade to serve as the Human Resource Development Program for the Western States by the National Institute for Mental Health. Upon the creation of Substance Abuse and Mental Health Services Administration (SAMHSA) in the early 1990's, Federal support for the Human Resources Development programs was discontinued. However, the Mental Health Program has extensive expertise in regional planning, consensus-building, recovery-driven services, cultural competence, telemedicine/Web-based health and knowledge synthesis and dissemination. Additionally, WICHE facilitated a multi-year activity to identify core-competencies in behavioral health practice that have been adopted as national standards by SAMHSA. Most recently the program was selected to serve in a consultation role to the rural issues subcommittee of the President's New Freedom Commission on Mental Health, and provided the professional support for the preparation of the subcommittee report and recommendations. Frontier Mental Health - WICHE is a recognized leader in the areas of rural and frontier mental health, workforce development, and the Frontier Mental Health Resources Network for researching and reporting on practices, problems and solutions in service delivery. WICHE served as the technical assistance center for frontier mental health under contract with SAMHSA from 1995-1998, when program funding was eliminated. WICHE has maintained a capacity to provide technical assistance focused upon frontier mental health services, and a portion of its Web site is devoted to this area of focus. Thus, between WICHE's higher education and mental health programs, an infrastructure of interstate and regional collaboration has already been established. Helping member States address rural and frontier mental health workforce shortages is a logical role for WICHE. The remainder of this report will describe the multilevel contexts in which workforce shortages exist, the implications of these shortages and a description of the possible solutions generated by consultants. The President's New Freedom Commission on
Mental Health Final Report: Rural Mental Health Workforce Shortages The National Context: Mental Health Care in America For the first time since the Carter Administration, there is a Federal initiative to evaluate and reform America's mental health system. President Bush's New Freedom Commission on Mental Health recently released its final report, which identified significant barriers to mental health care in the country, including fragmentation and gaps in care for children and adults with serious mental illness, a lack of care for older adults with mental illness, a failure to make mental health and suicide prevention national priorities, as well as socioeconomic factors, such as high unemployment and costly disability. The report concluded that incremental reform of the mental health system is no longer a viable option; a fundamental transformation is needed.The Commission identified national goals and potential action steps to transform mental health care, including (see http://www.mentalhealthcommission.gov/):
The Rural Context: Mental Health Care in Rural and Frontier America The New Freedom Commission on Mental Health final report included a subcommittee report on unique problems Americans living in rural or frontier regions face in accessing mental health care. The committee identified several key issues with respect to mental health in rural America:
Where and what is rural America?
Different government agencies use different definitions, typically based on population density and/or socioeconomic factors. Rural America is often viewed and defined by what it lacks, which is important and telling when considering mental health services. For instance, more than 60 percent of rural Americans live in "mental health professional shortage areas" (MHPSAs). Over 90 percent of all psychologists and psychiatrists, and 80 percent of MSWs, work exclusively in metropolitan areas. More than 65 percent of rural Americans get their mental health care from their primary care provider.
Due to these facts, accessing mental health services is difficult in rural America. Additionally, rural Americans have to travel further to provide or receive services, are less likely to have insurance benefits for mental health care, and are less likely to recognize mental illnesses and understand their care options. As a result, rural Americans enter care later in the course of their disorders, with more advanced symptoms, and require more intensive and expensive interventions. Compounding the problem is that there are few programs training professionals to work competently in rural places. Stigma is associated with having mental illness, and there is some professional misunderstanding about rural America, as indicated by the prevalent assumption that urban models of treatment and practice will work in rural areas. In summary, rural America needs, but does not have, an appropriate supply of technically competent and skilled professionals who have demonstrated knowledge and experience in rural/remote practice. Workforce Shortages Although the data in this area are not as consistently
Designated Mental Health Professional monitored as in other areas
of health care (often due Shortage Areas 
These workforce shortages are worse for specialty areas (e.g., children's mental health, older adult mental health), and are so great it is identified as a "hole in the safety net" in a recent report to the Secretary of the U.S. Department of Health and Human Services (National Advisory Committee on Rural Health, 2002). The availability of rural mental health professionals is dependent upon several interrelated factors, including education, rural training opportunities, recruitment and retention activities and continuing education and support. Existing funding streams and training programs
do not mandate a set of skills that lead toward rural competency
(National Advisory Committee on Rural Health, 1994). Most specialty
mental health (psychiatry and psychology) care is available only
in larger regional trade centers or locally only via itinerant providers
(Wagenfeld et al., 1994). Over the past decade, many rural hospitals
have either closed or converted to Critical Access Hospitals (CAH);
thereby limiting the number of available specialty services. Some
modifications to the CAHs convertion program however, has improved
availability of psychiatric units in some areas. Closures and conversions,
have further eroded the basic rural health infrastructure. Furthermore,
for rural persons with emergent mental health needs, law enforcement
is often the emergency responder and transport out of the community
(Larson et al., 1993). This could be prevented with the availability
of competent professionals to direct triage and stabilization. The Regional Picture: On average, WICHE States will see a projected
18 percent increase in the number of people between the ages of
18 to 64 entering the workforce by 2025 (the range is a low of 1.4
percent for North Dakota and a high of 37.8 percent in Hawaii).
However, the projected average percent of persons 65 and older (i.e.,
retirement age) leaving the workforce in WICHE States is a staggering
122 percent (with a low of 72.6 percent in South Dakota and a high
of 159.7 percent in Utah).
As this translates into actual numbers of people, some WICHE States will have more citizens entering than leaving the workforce, while others will have more leaving than entering (see Table 1). For instance, California is projected to have an increase of 2,828,432 in their retirement age population, but will have an increase of 7,326,046 (i.e., a gain of 4,497,614) in their workforce age population by 2025. Arizona, on the other hand, is projected to have an increase of 700,290 in their retirement age population, but an increase in workforce of only 373,026 (i.e., a loss of 327,264). In all, only four WICHE States-Alaska, California, Hawaii and New Mexico-are projected to have actual numbers of people entering the workforce in excess of the numbers leaving. Table 1: Projections of the Working and
Retirement Age Populations from 2000 to 2025.
Source: http://www.higheredinfo.org/ The implications of these projections are grim. Not only will most WICHE States have fewer people entering the workforce than leaving, the retirement-aged or elderly population will grow substantially. Since elderly persons typically require more healthcare services than younger age groups, it appears that without significant workforce development, there will be fewer people to offer these services. As indicated in the New Freedom Commission on Mental Health report, services to elderly populations are already insufficient. The significant increase in persons entering this age group over the next 20 years, combined with the relatively low numbers entering the workforce, suggests very serious problems in providing care to those who will need it most. Mental health workforce, especially in highly rural WICHE States, faces many of the problems in their rural mental health systems identified in previous sections. However, unique issues can arise for a given area due to State-specific characteristics, which may include economics and State budgets, reimbursement systems, natural disasters or other factors. Describing State-specific problems highlights both the commonalities and differences in the WICHE West and facilitates discussion of what others have done to address or prevent similar problems or ways that the region can come together to find solutions. Consultants from Nevada, Alaska, South Dakota, Arizona and Washington described the State of the field in their respective areas.Nevada: Nevada was described as having a rural professional staff vacancy rate of 22 percent (9 out of 40 positions). Additionally, the rural turnover rate in the last 4 years has been 23 percent. The problem is so severe that an attempt was made in the most recent legislature to reclassify social work positions to mental health counselor positions, thus, allowing both Licensed Marriage and Family Therapists and Licensed Clinical Social Workers to fill positions. Furthermore, the turnover rate is thought to be related to problems of cultural and rural competence. Many times, young professionals come from schools that do not have an appropriate curricula regarding rural or cultural competence, yet these are the areas in which they must work.
Nevada would like to look at higher education to turn out students who are able to work in the rural/frontier area. At present, psychiatrists do not live and work in rural Nevada. Therefore, the psychiatrist positions were converted into contract services. Twelve psychiatrists are under contract at the present time, and many clients are still waiting over 14 days for services. Some clients wait as long as 5 months for outpatient and medication clinic services. As a partial remedy, the State is utilizing the Federal Loan Repayment program to entice professionals (non-medical) to work in rural areas. In addition, the State is exploring ways to reimburse interview and moving expenses. Finally, there is considerable pressure to make positions revenue - generators to help offset State general fund dollars. Alaska: Two main questions being asked in Alaska are: How do we get young people interested in the field, and what is the field going to look like 10 or more years from now? One frustration is getting young people fresh from school who are unprepared to work in the current clinical environment. It is hoped that there will be a regional "think-tank" that envisions what the system should look like 10 or more years from now and finds ways to prepare young professionals for the coming system. A major issue is retention of providers:
Most young professionals only work in Community Mental Health Centers
for about 2 years, perhaps slightly longer. A tremendous amount
of time, energy, and money is spent teaching them the basics of
service provision (e.g., through supervision, mentoring); however
after approximately 2 years, they decide to go into private practice
or move out of the area. Precious resources are lost when this occurs.
Therefore greater efforts toward retention are needed. Rural Alaska has over 250 indigenous cultures living beyond all road systems and maintaining traditional hunting/gathering lifestyles in villages of 150 to 800 people. The rates of suicide among young Alaskan Natives in these areas is among the highest in the world. Rural University of Alaska campuses have Minority Serving designations, which serve Native Alaskans. To improve training and retaining of clinicians, a career track within the community needs to be created. There is a need to show people a career track once they get in the school system. (Young professionals function as free agents, and there is an obligation to work with providers and the system with this understanding.) Alaska has the vision of a counselor in every village. They envision residents from the villages functioning as counselors and doing basic intervention, screening and assessment and referrals. There is a need to "grow your own" in the communities and give professionals the resources and capabilities to stay in those communities.
Alaska is in the middle of integrating mental health and substance abuse services into a Behavioral Health Division. They are looking at licensing and credentialing issues, as this is very important, particularly in rural areas. There is a lot of expectation that practitioners be licensed or that they meet certain standards to be able to practice. However, there is a concern that these expectations would severely restrict the number of clinicians available. Alaska is also looking at collaboration between mental health and substance abuse providers, as well as primary care providers. Current funding is not enough to pay for separate administrative infrastructures for mental health agencies, substance abuse agencies and community health centers. Ideally, there would be a way to combine these organizations, thereby saving administrative dollars and providing direct service. Other important issues include over-regulation, technology and information sharing, and retention of providers. South Dakota: South Dakota reported many of the same kinds of problems as Nevada and Alaska, such as recruitment and retention, shortages of psychiatrists and clinicians (in the top three for all States), and inadequate access to care, which can result in higher costs. In 2002, the State formulated a Task Force on Children's Mental Health, which involved stakeholders from many State departments, advocacy groups, families and other members of the community. They collaborated with the WICHE Mental Health Program to conduct needs assessments, facilitate the meetings and conduct core competency studies. The needs assessment indicated that 58 percent of children with mental health problems are not receiving services. The Task Force Report had a number of recommendations, including the development of an action plan to address relinquishment of custody problems, early identification through screening and a public education campaign. The State is also looking at using telemedicine technology to improve access to services. Arizona: Arizona identified a number of challenges in their State. An assessment of the State's mental health workforce indicated an attrition rate of 34 percent. One of the outcomes of this assessment was an interview with workers. The number one frustration reported was confusion about their roles as mental health workers, as well as excessive paperwork and redundancy. Reasons for leaving one's job included low salaries, conflicting relationships with supervisors or lack of supervision. Information was also obtained from administrators and directors, who reported that people are not applying for these jobs, particularly support jobs. Arizona has been reviewing and working on these issues from several different angles. First, they are looking at their process of assessment, who is doing the assessments and why there is so much paperwork/data. After examining all the data being collected, the conclusion was that the majority of it was unneeded and had the effect of "paralyzing" clinicians. This led to an assessment of the essential data needed to make decisions about the delivery system, which turned out to be basic information regarding safety issues and reason for seeking services. An effort is currently underway to take this idea out into the State and "sell" it, as well as train clinicians on the new assessment process. Another way Arizona has recently addressed workforce issues is by completing a Provider Manual, which contains centralized policies written in laymen's terms to reduce past frustrations/confusion and increase providers' understanding of the State requirements and expectations. They have also released an RFP that seeks to help develop the workforce. Arizona is looking at more ways to use telemedicine technology to improve access. On the education front, they are looking at creating a partnership between Behavioral Health and Higher Education, particularly in terms of influencing curriculums in the higher education arena. Washington: Similar to other States, Washington is having significant difficulty recruiting and retaining all types of mental health professionals. For instance, it is projected that there will be a 13 percent increase in the shortage of psychiatric nurses. However, the problem is not a lack of applicants but a lack of schools; for every three applicants there is only one school opening available. Furthermore, teaching salaries for nursing school faculty are only about $20-30,000, which is less than the salaries of nurses working in the field. Recruiting and retaining psychiatrists is difficult. Many psychiatrists provide itinerant services to rural areas and are paid more for doing so. However, costly travel expenses and the higher rate of pay adds to the expense of these services. Additionally, a factor that keeps some psychiatrists from living in rural areas is that they have professional spouses who cannot find work in their particular fields. Other mental health professionals may begin their careers in rural areas, but often move to urban areas after receiving required supervision for licensure. Finally, the most challenging group of professionals to recruit and retain are geriatric mental health specialists. Given the statistics indicated earlier in this report regarding the projected increase in the elderly population over the next 20 years, it is likely that many, if not most, States will face similar shortages of geriatric specialists. At present, a Washington Task Force is reviewing
workforce shortage issues and developing some initial recommendations.
These include increases in nursing enrollment slot funding, increases
in nursing faculty funding and the use of scholarship and loan repayment
programs as incentives.
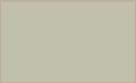
WICHE: Higher Education in the West, One potential avenue for decreasing the workforce shortage in mental health is through programs in higher education. A subsequent section will describe a number of existing higher education programs that might serve this purpose. This section will provide an overview of the current status of higher education regarding supply and demand, those who are or could be served in higher education, and the financial status of the WICHE West. Understanding the current and projected higher education environments will help administrators in mental health more clearly judge their options as they pursue opportunities. As a metaphor for the current and projected status of higher education, The Perfect Storm (David Longanecker, Director, WICHE) captures the idea that several "waves" of events and factors are occurring and need to be considered. In general, there are three primary waves: 1) an increasing demand and need for higher education by individuals and society in general, 2) a customer base that has been either difficult to serve or not served effectively, and 3) a limited pool of resources, at least in the public purses. Wave One - Rising Demand: The demand for college education is projected to rise 13 percent nationally (2002-2012) and the West's higher education enrollments will be the highest in the Nation. The graph below presents high, middle, and low projections of total enrollment in all degree-granting institutions over the next 8 years. Whether enrollment projections are actually at the low or high ends, it is expected that demand will significantly exceed supply. More specifically, it is anticipated that there will be a 25 percent growth in the 18- to 24-year-old population (2000-2015). The West's high school graduation rate is skyrocketing with expectations of a 12 percent increase (2002-2012), which is by far the biggest increase of any region (the South will see an 8 percent boost; the Northeast, 4 percent; North-central, .2 percent). In some States, such as California, these increases will likely be too great to be handled by the public education system. As a result, it is likely that parents will need to find ways to fund their children's education in the absence of government funding, which will create more strain for those families. Wave Two - Those We Serve will be Harder to Serve: Not only is the demand for higher education projected to exceed supply, but the diversity of students is expected to grow as well. An increasing share of higher education's population is coming from communities that higher education traditionally has not served well. For instance, communities of color will supply 54 percent of the West's high school graduates by 2012 (up from 41 percent in '02). Of course, this will differ from State to State (e.g., Hawaii = 87 percent, Nevada = 62 percent, Utah = just 8 percent). Another example is that Hispanic high school graduates will be 34 percent of the West's graduates (up from 23 percent in '02). The success rates for Hispanic students in school have not been high. For instance, in the United States, Hispanic students are 10.5 percent less likely to attend higher education. In 2000-01, Hispanics represented 24 percent of the population and 15 percent of full-time first-time freshmen. However, only 16 percent of those were awarded associate degrees, and 11 percent of those were awarded bachelor's degrees. 
Another group not historically served well in higher education is low-income students. For example, from 1999-2001 low-income student participation dropped from 27.5 to 23.1 percent. Additionally, 14 of the 15 WICHE States saw drops ranging from .2 to 8.4 percent. However, Hawaii was unique in the West, in that they saw an increase of 12.9 percent in low-income student participation (36.5 percent total). Some schools will be better equipped than others to accommodate this vast array of students, but others will struggle to gain the resources and professional staff that make it possible to provide a quality educational environment for all students. Nevertheless, there are some opportunities for mental health. For instance, since cultural and rural competence are considered important issues in transforming the mental health workforce, efforts can be made to attract students from diverse backgrounds into the field. Wave Three - Constrained Finances: As the two national maps below indicate, most States in the country are facing significant financial problems. All but five States faced or are facing budget shortfalls, 22 are in recession, 22 are near recession, and only six are expanding. The impact of September 11th on the Nation's and States' economies is well-documented, but there are other factors that contribute to State budget shortfalls. At the Federal level, a number of factors are indicated, including the general economy, tax cuts, funds being focused on homeland and international security, as well as the "No Child Left Behind" mandate. At the State level, many States have antiquated tax structures. For instance, States typically have sales taxes on goods, rather than services. Since ours is now a service-based economy, the current setup is misaligned.
To combat lost revenue and bring budgets into balance, States are taking a number of steps. One of the primary steps being taken is cuts in higher education, decrease in aid to localities, or across-the-board budget cuts. There have also been suspensions, such as with employer retirement contributions, construction projects, tax cut delays, or layoffs, furloughs, hiring freezes and early retirement. Finally, States have had to tap into other funds, such as "rainy-day" or tobacco settlement money, and many have had dramatic tuition increases.
WICHE Student Exchange Program/NEON: Higher Education Options A potential resource in addressing the rural mental health workforce gap is WICHE's three student exchange programs: Professional Student Exchange Program (PSEP), Western Undergraduate Exchange (WUE) and Western Regional Graduate Program (WRGP). Each of these will be briefly described. (Information is taken from and can be found at http://www.wiche.edu/SEP/WUE/index.asp.) The Professional Student Exchange Program (PSEP) PSEP enables students in 13 western States to enroll in selected out-of-State professional programs (e.g., dentistry, medicine, occupational therapy and optometry, to name just a few), usually because those fields of study are not available at public institutions in their home States. Exchange students receive preference in admission. They pay reduced levels of tuition, usually resident tuition in public institutions or reduced standard tuition at private schools. The home State pays a support fee to the admitting school to help cover the cost of students' education. State support and program participation affecting students are subject to change by legislative or administrative action. The number of students supported by each State is determined through State legislative appropriations. Traditionally, the PSEP program has supported the training of professionals in out-of-State programs because of three conditions: 1) the sending State identified the profession as critical; 2) the sending State's higher education institutions did not offer programs of study in the identified critical profession; and 3) receiving higher education institutions had capacity to accept students to their established programs. The conditions are different in the area of rural and frontier mental health.
Currently, no mental health disciplines are specifically identified as part of the PSEP program. For the most part, States have not identified mental health disciplines as critical. Additionally, most States have mental health professional training programs in nursing, psychology, social work, psychiatry and allied fields. However, they often do not have programs that specifically train mental health professionals to serve rural/frontier populations or other underserved populations (e.g., children, older adults, ethnic/racial minorities, etc.). As a result, the strategy employed to address professional development to meet the needs of underserved populations will need to develop a more refined process of discipline and training program identification. Finally, the current State revenue picture requires careful examination of funding strategies that could be used to support workforce development in this area. An array of existing fellowships, scholarships and loan repayment options exist at both Federal and State levels (e.g., National Health Service Corps Scholarship and Loan Repayment Program), and it may prove beneficial to create linkages between any WICHE regional activity and these programs. Students must meet requirements for certification and admission to the participating institution. Regarding certification, each State establishes its own requirements for certification through an application process and designates a State certifying officer. Certification is not a guarantee of support; only those students who are certified and funded through appropriations in each State can be supported via PSEP. In terms of admission, the student applies for admission to participating institutions through regular channels. The institution has full discretion regarding admission. Most States have some residency requirements, such as one year prior to application (AK, CO, ID, MT, NV, ND, OR, WA), or up to 5 years prior to application (AZ, HI, UT). There are also States that have a payback or other obligation once schooling is complete, such as repayment of all support fees (plus interest) or practicing in the "sending" State 1 year for each year of academic support received. The Western Undergraduate Exchange (WUE) Through WUE, students in western States may enroll in many 2 year and 4 year college programs at a reduced tuition level: 150 percent of the institution's regular resident tuition. WUE tuition is considerably less than nonresident tuition. Some receiving States will now accept students from all WICHE States, including California. Students do not need to demonstrate financial need to receive the WUE tuition benefit. Students who enroll in participating Western Undergraduate Exchange programs will qualify for the WUE tuition rate. Virtually all undergraduate fields are available to WUE students at the participating colleges and universities. Some institutions have opened their entire curriculum on a space-available or first-come, first-serve basis; others offer only designated programs. To be eligible for WUE, students must be a resident of one of the WICHE States. However, residents of California may only be accepted in some States in some institutions. Please refer to each State's listing to determine if this applies. Some colleges and universities also have additional criteria such as American College Testing (ACT)/Scholastic Aptitude Test (SAT) scores or high school Grade Point Average (GPA). Consult the WUE Bulletin for details. At present, more than 17,000 students participate in the WUE program. Through the WUE program, WICHE States have saved a combined total of $77.8 million. By State, the savings are:
The Western Regional Graduate Program (WRGP) WRGP makes high-quality, distinctive graduate programs available to students of the West at a reasonable cost. As part of the Student Exchange Program of WICHE, WRGP helps place students in a wide range of graduate programs, all designed around the educational, social and economic needs of the West. Through WRGP, residents of Alaska, Arizona, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, North Dakota, Oregon, South Dakota, Utah, Washington and Wyoming are eligible to enroll in available programs outside of their home State at resident tuition rates. Students need not meet financial aid criteria. To receive WRGP tuition status, students simply apply directly to the institutions of their choice and identify themselves as WICHE WRGP applicants. WGRP students must fulfill all the usual requirements of the institution concerned and meet all admission deadlines. WRGP is open to all residents of the 14 participating States. Normally, students should be a resident of one of these States for at least 1 year before applying for admission as a WRGP student. Determination of residency is usually made by the institution where the student is enrolling. If necessary, the WICHE certifying officer of the student's home State can assist the institution in making a determination of residency. The Northwest Educational Outreach Network (NEON) Project WICHE is partnering with NEON, a group of 32 higher education institutions and State governing and coordinating boards in 10 States, to develop new strategies to improve student access to various academic disciplines using technology-mediated education. Through institutional collaborations, NEON is working to extend the availability of degree programs in three disciplines to students via Web-based or electronically-delivered courses. The initial programs include: a Ph.D. in nursing; a graduate certificate in logistics and supply chain management; and online courses that lead to fulfilling the certification requirement for school librarians. This interstate project is funded by the U.S. Department of Education's Fund for the Improvement of Postsecondary Education (FIPSE). Over time, NEON's collaborations may be expanded to include other academic programs; allowing students to enroll in courses while remaining in their communities. In addition to current WICHE programs that may be useful to States in narrowing their workforce shortages, consultants from Nevada, Alaska, North Dakota and Idaho described programs in their respective States that have the same purpose. These are summarized in the table below. In terms of rural shortage, two general models exist, both of which are valuable. One was described as the "Brill Cream" model, in which some amount of rural focus will do and/or is better than nothing. On the other hand, the second model indicates that one must have, within an institution, departments that focus on rural from "A to Z," that is, a program fundamentally focused on rural issues and competency. One difficulty is that mental health programs are primarily in metropolitan universities, and rural health tends to be overlooked. What is needed is a change on the mission to include rural issues more prominently. It was suggested that Land Grant University models may be a mechanism that could be used or built upon via cooperative extension, as this is a new perspective is community health.
Legislative Consultant Comments Developing a broader and more stable mental health workforce has to occur within the context of political realities. As described earlier, States are facing budget shortfalls that require tighter control over spending. It is unclear when the national and State-level economies will rebound, which creates generalized uncertainty and can interrupt planning. However, consulting legislators from South Dakota and Nevada provided a clearer picture of what States are facing politically and what can be done to facilitate mental health workforce development and connections to higher education within the current context of fiscal tightening. Each legislator explained aspects of their State, including current major issues. For instance, South Dakota was described as a generally low tax State, as it is a very rural and low wage (37th for per capita income) State. However, it has one of the most broad-based sales tax programs in the country. The pros and cons of this system were discussed, especially regarding the effect changes in the system would have on funding. There is also a very large Native American population in South Dakota, which, given the history of difficult relationships between this population and the government, raises unique issues. Nevada, on the other hand, was described as being a largely metropolitan State (70 percent of the population lives in Las Vegas). However, there are significant rural areas that deal with many of the issues described at the beginning of this report. Furthermore, legislators representing rural areas were described as less active in promoting mental health service programs. Nevada has recently increased their mental health budget, yet the State is ranked 50th in getting their share of Federal tax money back. The State has a growing Latino population, but no Latino legislators.
he legislators emphasized the importance of mental health organizations or groups presenting a unified message and relevant data regarding their needs. Too often, different groups from the same field will not collaborate and, in turn, present conflicting requests or ideas to legislators. Legislators are generally uncomfortable having to make a choice of one group over the other in such circumstances. There was agreement that higher education can play a significant role in workforce development. Early prevention with family involvement was seen as critical to addressing mental health problems generally; however, there was acknowledgement that the "No Child Left Behind" mandate is frightening to many teachers and school officials, and may remove focus from youth who have mental health problems. On the other hand, some see this program as a way to encourage schools to find ways of more effectively working with youth and their families, particularly through collaboration with mental health agencies.
Workforce Development Planning WICHE has been working with expert consultants to examine more closely the mental health workforce needs of the WICHE West as a first step in developing a comprehensive mental health workforce development strategy. A component of these activities was the identification of specific professional disciplines and potential training programs to accept students for inclusion in the PSEP program. Other aspects included identifying the components of a transformed rural and frontier mental health shortage initiative, the strengths of the region, the regional barriers/ challenges and the academic assets (e.g., current training programs) and resources. Tables 4 - 9 in Appendix B list responses for each of these areas, but each will be summarized in this narrative. Components of a Transformed Rural & Frontier Mental Health Shortage Initiative Creating the components of a transformed mental health workforce requires a strategy that looks at both short and long-term goals. For instance, one near-term goal identified was focusing on "professionals in transition" and helping them re-invent their roles. This group usually consists of young professionals, not many years out of their graduate programs, who have good clinical experience but are unsure in what direction to take their careers. Long-term goals include the idea of "grow your own" professionals, curriculum overhaul, and inter-disciplinary collaboration. A major component of transformation is rural-specific training and research. Regarding training, it was suggested that there be either rural training programs or rural tracks that lead a student from paraprofessional through post-graduate study and work. This will require significant overhaul of current curricula in many programs, as well as a greater emphasis on rural and cultural competence. Students should also have opportunities for rotations and/or practica in rural communities. In accordance with the "grow your own" concept, consultants suggested targeted efforts to engage indigenous rural/frontier residents in professional development. Distance learning and continuing education programs were considered important for addressing workforce shortages. Additionally, the importance of engaging research universities to provide support for developing best practices related to rural mental health cannot be understated. The WICHE West is a strong region for many reasons. A primary and fundamental reason noted by consultants is a shared philosophy regarding the desire for communities to prosper and be healthy. In this regard, there is a commonality of need, particularly in rural areas. In such places, there is what may be called "relationship capital," meaning that those who live and work together recognize and value what each member of the community has to offer. This also extends to collaborative efforts of organizations, such as rural associations or other agencies (e.g., VAs, IHS, HRSA). People from diverse backgrounds live in rural areas; there is a wealth of knowledge and experience into which one can tap. Furthermore, WICHE States have innovative programs to share, universities sensitive to rural issues (e.g., Health Sciences Centers) and researchers who can investigate and help identify best practices for treating Americans in rural areas with mental health problems. Technology is linking people together who were formerly separated by geographic or other barriers. In addition, the WICHE infrastructure and specific programs (e.g., Nursing) were identified as strengths of the region. Thus, the region has strengths that range from common philosophy to organized infrastructures that will facilitate change.
Regional Barriers and Challenges Capitalizing on strengths requires an honest assessment of the barriers and challenges one faces. The WICHE West has numerous strengths, but also significant barriers, some of which were described in previous sections focusing on rural mental health. Consultants identified a number of barriers and challenges western States face, which can be categorized as: 1) Disciplinary, 2) Academic/Practice, and 3) Political. As a discipline, mental health is fragmented. Squabbles between different groups of clinicians exist, as does competition to acquire students, communication is poor, and sub-disciplines have dissimilar training, philosophy and credentialing processes. In this regard, there is a significant rift between academia and mental health practice, especially related to rural. Part of the rift derives from a negative view of rural, considered to be "second class." Rural research is not considered significant. There is also a positive myth that rural areas are idyllic places where few problems exist. However, as described earlier, issues that many in urban or suburban areas take for granted, such as transportation, are highly salient issues for those in rural America. A lack of understanding about rural exists in Federal and State political arenas as well. The Federal government tends to use eastern and metropolitan models, assuming they apply to the rural west. As noted earlier, there are multiple Federal definitions of rural, which affect funding. States better understand rural issues, but a "suburbanization" of legislators translates into poorer representation in political decision making for rural residents. Similarly, there is limited family and consumer participation in shaping State systems of care. Furthermore, those systems tend to be reactionary and range-of-the-moment in their focus. Taken together, these are significant difficulties to be overcome, as they cut across multiple areas of the mental health care system. Potential Mental Health Disciplines, Academic Assets, and Resources As the WICHE West moves toward transforming the mental health workforce, it will need a clear vision of what it will do and how it will be done. That is, what will the workforce consist of and how will this vision be achieved programmatically. Consultants took on the task of answering these questions through several steps that included identifying: 1) potential mental health disciplines, 2) academic assets (i.e., existing training programs), and 3) resources to support their efforts. (Lists of each of these areas are provided in Tables 7-9 in Appendix B.) In terms of potential disciplines States might create, a general idea is that programs can be created that are geared toward a particular level of training (e.g., paraprofessionals, Masters, Doctoral), a particular focus (rural, community health, primary care), or a combination of the two. In any of the cases, it is important to look not only at those trained specifically in mental health (e.g., psychologists, social workers), but also those who work in a mental health capacity (e.g., nurses, school personnel, primary care) and are from the local area. For example, a program might be developed that begins with an associate's level certification combined with paraprofessional practice, then moves a person through bachelor's and graduate training to either a master's or doctoral level. Such a program could have a rural or community and cross-cultural emphasis, and recruitment could focus on people indigenous to the area in which the program is offered. A number of programs exist in the WICHE West that could be used as models for creating new disciplines. For example, there is the program at the University of Alaska that was described in an earlier section, a rural psychiatry program at the University of New Mexico, and multidisciplinary family practice residencies through the Universities of Wyoming, Utah, Hawaii and Idaho State University. The University of Alaska also has a distance learning program for working paraprofessionals called "Learn as You Earn." There are master's programs in human services at Sinte Gleska University and in nursing at UNLV. This is not an exhaustive list of relevant programs, but examples that others might consider doing in their States.
In order to realize the potential programs and disciplines identified, it is necessary to identify the resources that will support these efforts. Among the resources identified were State-sponsored loan repayment programs, the Federal Office of Rural Health Policy's Network and Outreach grants, or employer-sponsored career ladder programs for graduate degrees. Other suggestions included looking at Title IV-E possibilities, HCAP, the National Health Service Corps repayment and scholarships program or Americorp educational stipends. In addition to these ideas, two Federal partnership opportunities with the Rural Assistance Center (RAC) and the National Health Services Corps (NHSC) were described, which will be discussed in the next section. Federal Partnership Opportunities The Office of Rural Health Policy has created the Rural Assistance Center (RAC), which is a new national resource on rural health and human services information. From their Web site (www.raconline.org), the RAC was "established in 2002 as a rural health and human services 'information portal' to help rural communities and other rural stakeholders access the full range of available programs, funding, and research that can enable them to provide quality health and human services to rural residents. To accomplish this, RAC gathers and streamlines information from myriad sources and provides easy access to that information. In gathering, synthesizing, and disseminating that information, RAC works with the State Offices of Rural Health, the Rural Health Research Centers, Poverty Research Centers, Area Agencies on Aging, American Public Human Services Association, the National Association of State Workforce Agencies, the National Association of Counties and many other public and private efforts." To achieve its goals, RAC:
The RAC also provides links to funding opportunities across a range of disciplines. The National Health Services Corps (NHSC)
also has various programs that might present partnership opportunities
for States seeking to expand their mental health workforce. The
mission of the NHSC is to improve "the health of the Nation's
underserved." Approximately 50 million people live in communities
without access to primary health care, and NHSC helps these communities
recruit and retain primary care clinicians, including dental and
mental and behavioral health professionals. These communities exist
across the country, in rural and urban areas.
Review and Identification of Next Steps Based on the workforce development planning, WICHE asked consultants to describe the steps Key stakeholders such as State mental health divisions, legislators, advocacy organizations and educators can take to begin developing a more stable and effective mental health workforce in their respective areas. The identified steps are:
WICHE agreed to do the following:
The WICHE West is a vast area rich with people, knowledge and opportunity. Due to its very rural nature, there are barriers and challenges facing mental health, particularly in regard to workforce shortages. However, these consultations demonstrate that people in leadership positions are willing to meet these challenges head-on, with optimism and enthusiasm. Some major themes that emerged from the consultations were that WICHE States share a common philosophy about helping people in their communities, face similar problems in their respective systems, but also have resources within and among the States. Specifically, there are existing programs that train professionals to work in rural/frontier areas. However, there is a need to expand and support these programs innovatively and provide incentives for clinicians in multiple disciplines to remain in the areas where their services are most needed. Programs that "grow their own" clinicians starting at the paraprofessional level and moving to the advanced graduate level, will be particularly valuable. Additionally, there is a need to improve training curricula to focus on rural/frontier issues, provide opportunities to practice in those areas and conduct research that identifies best practices for treating rural residents. WICHE has programs in higher education that may be expanded to include mental health professions. WICHE's Mental Health Program can offer technical assistance, program evaluation, needs assessment and training in cultural and rural competence for those States interested. Health Professional Shortage Areas (Mental Health) Alaska
Arizona
California
Colorado
Idaho
Hawaii
Montana
Nevada
New Mexico
North Dakota
Oregon
South Dakota
Utah
Washington
Wyoming
Table 4
Table 5
Table 6
Table 7
Table 8
Table 9
APPENDIX C Alaska Blanche Brunk Bill Hogan Gerald Mohatt Karen Perdue Elizabeth Sirles Arizona Suzanne Rabideau Idaho Ray Millar Martha Wilson Maryland Blanca Fuertes Charles VanAnden Montana Arthur McDonald Nevada Carlos Brandenburg Larry Buel Roseann Colosimo Caroline Ford Sheila Leslie Pamela Matteoni Ron Sparks, II New Mexico Daniel Montoya North Dakota Mary Amundson Oregon Paula McNeil South Dakota Amy Iversen-Pollreisz Ed Olson Wyoming Pablo Hernandez James Page
Scott Adams Sandy Jackson David Longanecker Jere Mock Dennis Mohatt Jenny Shaw APPENDIX D Mental Health Oversight Committee Members FY 2003-04 ALASKA ARIZONA CALIFORNIA COLORADO HAWAII IDAHO MONTANA NORTH DAKOTA NEW MEXICO NEVADA OREGON Diane Vines SOUTH DAKOTA UTAH WASHINGTON WYOMING |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

![]()
Go to:
Top | HRSA
| HHS |
Disclaimer | Accessibility
| Privacy