|
|
 |
|
|
The Health Center Model of Care
Health centers build on and complement other
Federal and non-Federal health service efforts
and fill major gaps where there are no existing
programs or resources. For example, while the
Federal Government and States broaden access
to health care through financing streams such as
Medicaid, Medicare, and SCHIP, health centers
ensure access to a comprehensive and regular
source of care for the populations covered by these
funding streams. This is of particular importance
during a time when the proportion of physicians
serving existing Medicaid and uninsured patients
and those willing to accept new Medicaid or
uninsured patients has continued to decline.
Accordingly, over 45 percent of health center
patients are Medicaid, Medicare, SCHIP, or other
public insurance beneficiaries and nearly 40 percent
are uninsured.
As funding and eligibility for health center services
are not tied to individual patient characteristics
(e.g., women or infants) or specific health
conditions (e.g., diabetes or HIV/AIDS), health
centers have the unique ability to reach certain
underserved populations often excluded from
existing Federal, State, or private sector health
funding streams such as non-elderly, non-disabled,
low-income men.
Health Center Financing
Financing and revenue sources play a key role in
the ability of health centers to address their goals of
increasing access, improving quality, and reducing
health disparities.
Health centers rely on a number of revenue sources.
The major source for all health centers is Medicaid
with over one-third of health center revenue
coming from the program.
- About one-fifth (19 percent) of
health center revenue comes from
the Federal health center grant.
- Remaining funding comes from: State,
local, and philanthropic organizations;
other third party sources, sliding fee
schedules, and Medicare; as well as
other Federal programs or payors.
Given this mix of funding and revenue sources,
it is imperative that health centers continue to
coordinate and collaborate with payors at Federal,
State, and local levels to continuously demonstrate
their value and role in increasing access and
eliminating disparities as health care homes.
Is Health Center Care Free? While all health centers and FQHC Look-Alikes must
provide access to services without regard for a person’s
ability to pay, services are not free. Rather, each health
center has a set schedule of fees and corresponding
discounts—often referred to as a “sliding fee scale” for the
services they provide. The sliding fee scale is based on a
patient’s ability to pay, as determined by annual income
and family size according to the most recent Federal
poverty guidelines.
In order to remain financially viable and competitive in their
local marketplace and to help improve access to care,
health centers also assist patients with screening and
enrollment into all available public and private insurance
programs such as Medicaid, Medicare, and SCHIP.
Health centers must always ensure that billing for patients
without insurance, collection of copayments and fees,
and screening for financial status, is done in a culturally
appropriate manner to ensure that these steps do not
present a barrier to care.
How does the sliding fee scale work?
All patients whose annual individual and/or family income
is below 200 percent of the poverty guidelines are eligible
for discounts on the care they receive.
- Patients whose incomes fall below 100 percent of the
poverty guidelines receive care at no cost or for a
small fee.
- Patients whose incomes fall between 100 and 200
percent of the poverty guidelines pay some portion or
percent of the care received, the amount or percentage
is determined through policy set by the health center’s
governing board.
Health Center Performance
Health center data, peer reviewed literature, and
major reports continue to document that health
centers successfully increase access to care, promote
quality and cost-effective care, eliminate health
disparities and improve patient outcomes, especially
for traditionally underserved populations.
Prenatal Care and Birth Outcomes
Identifying maternal disease and risks for
complications of pregnancy or birth during the
first trimester helps improve birth outcomes. By
monitoring timely entry into prenatal care, the
Health Center Program can assess both quality of
care as well as health center outreach efforts.
Results over the past few years demonstrate
improved performance as the percentage of
pregnant health center patients that began prenatal
care in the first trimester grew from 60.7 percent in
2001 to over 64 percent in 2006.
Appropriate prenatal care management can also
have a significant effect on the incidence of low
birthweight (LBW), the risk factor most closely
associated with neonatal mortality. Monitoring
birthweight rates reflects both on quality of care and
health outcomes for health center women of childbearing
age, a key group served by the Program.
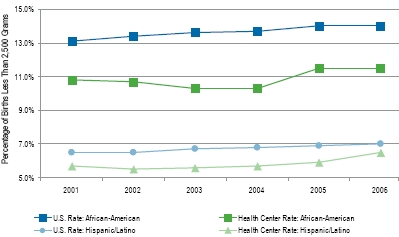
When compared to the national rate, health centers
demonstrate impressive performance. In 2005, 7.3 percent of health center patients had LBW
infants, a rate that was 11 percent lower than seen
nationally (8.2 percent, 2005 national LBW rate).
Overall, between 2001 and 2006, health center LBW
rates have continued to follow a steady pattern at
about 7 percent, more than 7 to 13 percent lower
than national rates which have continued to rise.10
Table 6. Improving Health Outcomes: Timely Entry into Prenatal Care at Health Centers, 2001-2006
Year |
2001 |
2002 |
2003 |
2004 |
2005 |
2006 |
| Percentage of Health
Center Patients Served Starting Prenatal Care
in First Trimester |
60.7% |
60.1% |
62.2% |
63.3% |
63.4% |
64.2% |
Source: U.S. Department of Health and Human Services, Health Resources and Services Administration, Bureau of Primary Health Care.
Uniform Data System. Rockville, Maryland: U.S. Department of Health and Human Services, 2004-2006.
Figure 3. Reducing Health Disparities: Health Center African-American and Hispanic/Latino Low Birthweight Rates, Consistently Below U.S. Rates, 2001-2006
[D]
Source: U.S. Department of Health and Human Services, Health Resources and Services Administration, Bureau of Primary Health Care.
Uniform Data System. Rockville, Maryland: U.S. Department of Health and Human Services, 2001-2006.
Source: Hamilton BE, Martin JA, Ventura SJ. Births: Preliminary Data for 2006. National vital statistics reports; vol 56 no 7.
Hyattsville, MD: National Center for Health Statistics. 2007.
Source: Martin JA, Hamilton BE, Sutton PD, Ventura SJ, Menacker F, Kirmeyer S, Munson ML. Births: Final data for 2005. National
vital statistics reports; vol. 56 no. 6. Hyattsville, MD: National Center for Health Statistics. 2007.
It should also be noted that health centers serve a
higher risk prenatal population than seen nationally,
making progress on these performance indicators a
particular accomplishment.
Health Centers Rated Among Top Federal
Programs. A 2007 Office of Management and Budget review tool used
to assess all Federal programs awarded health centers the
highest possible rating of Effective—a ranking achieved by
only 19 percent of all programs.11 Key findings include tha the Health Center Program:
- Effectively extends access and delivering high quality
health care to underserved populations;
- Demonstrates progress in meeting long-term and short-
term performance goals; and
- Effectively collaborates with other programs that share
common goals.
Chronic Disease
Health center patients, including low-income
individuals, racial/ethnic minority groups, and
persons who are uninsured, are more likely to suffer
from chronic diseases such as hypertension and
diabetes. Clinical evidence indicates that access to
appropriate care can improve the health status of
patients with chronic diseases and thus reduce or
eliminate health disparities.
Controlling blood pressure (hypertension) can
reduce the health risk associated with conditions
such as heart disease and stroke. However,
with increasing rates of hypertension, effective
control is a particularly ambitious undertaking as
improvements in such a chronic condition often
requires treatment with both lifestyle modifications,
usually as the first step, and, if needed, with
medications. According to the Centers for Disease
Control and Prevention (CDC) data for 2004, only
36 percent of adults nationally demonstrated
adequate high blood pressure control while health
center patients far exceeded the national rate at 44.4 percent of patients with blood pressure
under control.12, 13
Promoting Efficiency
Health centers have a demonstrated track record
in providing cost-effective services. Health centers
continue to maximize the number of patients
served per dollar while keeping cost increases below
annual national health care cost increases. In 2005,
the average cost per patient served at health centers
grew by only 2.1 percent. In 2006, costs grew at
a slightly higher rate (4.6 percent), but were still
about 33 percent below the 6.8 percent projected
growth rate for national health expenditures.
In fact, over the past 4 years, cost increases at
health centers have been at least 20 percent below
national cost increases.14 By restraining increases
in the cost per individual served at health centers
below the national per capita health care cost
increases, the Program has been able to serve
more patients that otherwise would have required
significant additional funding to serve annually
elsewhere.
Success in achieving cost-effectiveness may
in part be related to health centers’ use of a
interdisciplinary team that treats the “whole
patient.” This, in turn, is associated with the
delivery of high quality, culturally competent, and
comprehensive primary and health care services
that not only increases access and eliminate health
disparities, but promotes more effective care for
health center patients.
�
External Evaluation
In addition to internal monitoring of health center
performance, peer reviewed literature and major
reports continue to document that health centers
successfully increase access to care, promote
quality and cost-effective care, and improve patient
outcomes, especially for traditionally underserved
populations.
- Health center uninsured patients are more
likely to have a usual source of care than the
uninsured nationally (98 percent versus 75
percent).15, 16
- Health centers provide continuous and high
quality primary care and reduce the use of
costlier providers of care, such as emergency
departments and hospitals.17
- Uninsured people living within close proximity
to a health center are less likely to have an
unmet medical need.18
- Health centers have demonstrated success in
chronic disease management. A high proportion
of health center patients receive appropriate
diabetes care.19
- Medicaid beneficiaries receiving care from a
health center were less likely to be hospitalized
than Medicaid beneficiaries receiving care
elsewhere.20
- Health center Medicaid patients were 11
percent less likely to be inappropriately
hospitalized and 19 percent less likely to
visit the emergency room inappropriately
than Medicaid beneficiaries who had another
provider as their usual source of care.21
- Health centers have been found to improve
patient outcomes and reduce racial and ethnic
disparities in health care.22, 23, 24
- Health center low birthweight rates continue to
be lower than national averages for all infants.
In particular, the health center low birthweight
for African-American patients is lower than
the rate observed among African-Americans
nationally (10.7 percent versus 14.9 percent
respectively).25
- Health center patient rates of blood pressure
control were better than rates in hospital
affiliated clinics, the U.S. Department of
Veterans Affairs health system, or in commercial
managed care populations.26
next page > Sustaining the Connections
|
|
|
|
|

Health Centers:
A Coordinated Effort and
Investment
Health centers must:
- Coordinate and collaborate appropriately with other
health care and social service providers in their area to
ensure the most effective use of limited health resources
and to provide access to the most comprehensive array
of services and critical assistance including, housing,
food, and job support.
- Maximize all sources of revenue, including non-grant
resources.
|
|
|
