 |
 |
 |
 |
 |
||||
 |
|||
| Setup Instructions |
|
EMERGENCY
MEDICAL SERVICES IN FRONTIER AREAS:
VOLUNTEER COMMUNITY ORGANIZATIONS
This publication
was funded by the Health Resources and Services Administration's
Office of Rural Health Policy with the Frontier Education Center
under
TABLE OF CONTENTS Note on the Definition Of
Frontier
Appendix A: Frontier and Rural Expert Panel Appendix C: Frontier
Education Center EMS Information Request, April 2005:
All references to "frontier" use the Consensus Definition of the Frontier Education Center unless otherwise indicated. Counties and/or frontier areas so defined have been developed with the involvement of all of the relevant State Offices of Rural Health (100 percent response rate). This definition has not been adopted by any Federal programs but has been adopted as policy by the Western Governors' Association and the National Rural Health Association. The Consensus Definition weights three elements - population density, distance in miles and travel time in minutes - which together, generally describe the geographic isolation of frontier communities from market and/or service centers. The Center understands that various programs will establish their own programmatic definitions and eligibility criteria.
Emergency Medical Services in Frontier Areas: The purpose of this paper is to provide information on paid and volunteer Emergency Medical Services (EMS) workers in frontier and rural areas. This is not a formal research paper, but a presentation of an information-gathering project and a fact checking of anecdotes. Frontier and Rural Expert Panel. A panel of frontier and rural leaders from varied backgrounds met on April 14, 2005 to discuss several issues facing frontier and rural communities. The members of the panel are listed in Appendix A. Pertinent to this paper, a discussion was held on the broad topic 'Volunteer and Paid Emergency Medical Services in Frontier and Rural Areas.' In preparation for the meeting, readily available information was gathered to supplement the panel discussion. An Internet literature search for information on paid and volunteer EMS workers in frontier and rural areas was conducted. Because only limited information was available from any single source, multiple data sources were combined. Information from State EMS Offices. Using the directory of the National Association of EMS Directors (NAEMSD), each State EMS office was contacted by email and/or telephone. Appendix C presents a compilation of State responses. Where possible, these data were supplemented by other data available online, including a 2003 survey conducted by the National EMSC (EMS for Children) Data Analysis Resource Center (NEDARC). It became clear that there is no uniform EMS data collection among the States. Some States collect information about paid or volunteer workers; others do not. Among those that do, only a few of those report rural or frontier services separately. Therefore, outreach was made directly to the field to clarify or expand upon the information available to the public and gathered for the Expert Panel. Unsurprisingly, the view from the grassroots is often quite different from the data presented by various agencies. Complicating the entire project is the absolute lack of a consistent definition of the word "volunteer." A. Brief History of Modern EMS Prior to the development of modern EMS in the 1960s, only a few hospitals in large cities provided ambulance service. In most communities, a trip to the hospital was provided by friends and family or by the funeral home. In the late 1950s, as more Americans became car owners and driving a car replaced other forms of transportation, more people were subsequently injured and killed in crashes. The first rescue squads began to emerge and they were primarily volunteer (Nelsen & Barley 1997). According to Nelsen & Barley (1997), "The EMT's work emerged out of a series of social movements that first made a national priority and then a medical issue of what was initially a logistical problem: how to transport injured motorists to hospitals" (p. 627). The modern era of EMS began after the 1966 publication by the National Academy of Sciences, National Research Council paper "Accidental Death and Disability: the Neglected Disease of Modern Society" (McGinnis 2004). Improved equipment and advanced training for medics during the Viet Nam War led to numerous advances in emergency medicine. These new skills and equipment were soon put to use at home. The National Highway Safety Act of 1966 was the first Federal legislation requiring States to develop systems to rescue injured motorists. Most States provided these services by organizing and equipping volunteer rescue services. The Federal Emergency Medical Services Systems Act of 1973 established the first national standards for training and equipment. In many communities, EMS is provided as a public safety function supported by the National Highway Transportation Safety Administration (NHTSA) as well as State and local governments. In other communities EMS is considered a health service with State and/or local support. Recently, Homeland Security planning has recognized the importance of EMS. A recent issue brief recommends creating an Emergency Medical Services Administration within the Department of Homeland Security (Cilluffo, Kaniewski and Maniscalco 2005). B. Models of EMS Service Provision In the United States, a number of funding and
staffing models are used to provide EMS. Distinctions are 1. organizational
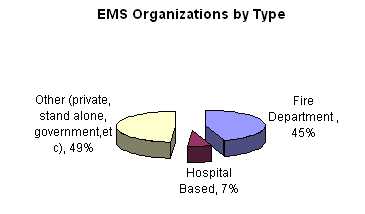
type (public, private non-profit, private for-profit); According to the Journal of Emergency Medical Services, 44.89 percent of EMS systems are fire department based, 6.51 percent are hospital based, and 48.60 percent are either private, stand alone government agency, or other type (Journal of Emergency Medical Services 2004).
In most rural areas, EMS evolved from the same volunteer model as fire departments. A significant difference is that there are more ambulance calls than fire calls, longer distances to the scene as well as longer transport times. So the time commitment is often much greater for a community EMS volunteer than for a volunteer fire fighter. Many consider EMS to be in the process of "professionalization,"
undergoing a transition from a volunteer service to a paid occupation
(Nelsen & Barley 1997). In urban areas, this transition is mostly
complete. Although some consider completion of this transition to
be inevitable, others view this process as neither inevitable nor
desirable. The 1996 NHTSA EMS Agenda for the Future asserts
that provision of EMS services "will continue to be diverse
at the local level" Studying the mix of paid and volunteer EMS providers is difficult for a number of reasons. First, all EMS providers receive the same training, testing and certification at the State level, regardless of whether they are paid or volunteer. Most States do not track paid or volunteer status in their data systems. Multiple Definitions of Volunteer. As mentioned
previously, there is no single definition of "volunteer."
In rural communities, many volunteers are paid a stipend for being
on call or for responding to an emergency and/or transporting patients,
but since they do not derive their living from this they are still
considered volunteers. In North Dakota, for example, 90 to 95 percent
of EMS workers are considered volunteer, while 45 percent report
being compensated in some way for EMS work (UND Rural EMS Initiative
2000a). In some EMS systems, they might be reported as "paid"
to the State EMS bureau, but in reality they are rarely compensated
as a fulltime professional. Where a service makes use of both paid and volunteer providers, the service itself may be classified as paid. Wendover Ambulance in Nevada is a "paid" service, operating with four fulltime paid workers. Fifty volunteers, half of whom come from Salt Lake City, located 120 miles away, supplement this capacity. For the purpose of this paper, "volunteers"
are those who are described as volunteers by informants.
II. CHALLENGES FACING VOLUNTEER EMS SYSTEMS In frontier and rural areas, volunteers provide most EMS. Challenges facing volunteer EMS providers include the availability of volunteers, aging of the volunteer workforce, the impact of national standards and testing, challenges at the primary workplace, and maintaining skills in a low-volume environment. Many informants reported that recruiting and retaining EMS volunteers is becoming more difficult. The National Rural Health Association "Agenda for the Future" reports that 2000 and 2004 surveys of State EMS directors identified ongoing recruitment and retention of personnel as the greatest challenge (McGinnis 2004). Demographic, social, cultural and economic changes of the past 30-40 years have reduced the number of people who have time available to volunteer. Based on population alone, frontier and rural areas have a smaller pool of potential workers who must serve larger geographic areas. Many frontier and rural communities face declining populations, with older, often retired populations remaining. In many of these communities, economic stress causes individuals to work at more than one job when employment is available. There are often long commutes to distant jobs. Families in which both parents work have become common in rural communities. Many potential volunteers are also hampered by a lack of childcare options, especially with the unplanned, middle of the night, urgent nature of EMS. A North Dakota survey of EMS personnel found that the time commitment was the most significant barrier to recruiting new providers, as well as the primary reason former EMT's give for leaving EMS (UND Rural EMS Initiative 2000b). Reports from Nebraska (Ullrich, Mueller and Shambaugh-Miller 2004) and Minnesota (Minnesota Department of Health 2002) identified the same factors. In these three States volunteers indicated that the time commitment was especially burdensome because they are either completely uncompensated or paid lower stipends than urban volunteers. Time away from job and time away from family were reported as significant barriers by rural squad leaders (UND Rural EMS Initiative 2000c). Retention is as serious a problem as recruitment; the survey found that the average volunteer plans on working in EMS for five years yet leaves after three. A number of States are focusing on ways to improve volunteer recruitment and retention. The Rural Emergency Medical Services Initiative at the University of North Dakota Center for Rural Health developed an EMS Recruitment and Retention Manual (UND Rural EMS Initiative, no date). In Wisconsin, EMS Association Director Don Hunjadi reports that with effective recruiting tools and working with local services, his organization has been able to attract one volunteer for each 500 - 1000 people in a service area. Aging volunteers will one day become retiring volunteers, further reducing the volunteer base. The 2002 report, "A Quiet Crisis: Minnesota's Rural Ambulance Services at Risk," shows that in rural Minnesota, volunteers make up 77 percent of personnel (Minnesota Department of Health 2002). In two regions (Southwest and South Central), the volunteer percentage is 91 and 92 percent. The average age of rural volunteers tends to be older with 45 percent over the age of 40, compared to 34 percent in urban areas. A 2003 Nevada survey, "Nevada Emergency Medical Services Survey Results," documented that respondents in rural counties "were older on average than their urban counterparts, while at the same time Census figures show an older than average general population in many rural counties" (Fadali, Nolan and Harris 2003). C. Impacts of National Standards and Testing The National Registry of Emergency Medical Technicians (NREMT) administers a national exam for each level of emergency services provider in order to standardize training and testing. A benefit of standardization is increased reciprocity of workers among States. Some States require continuous NREMT testing; others require it only for the first licensure exam. The NREMT website shows only five States with no national registry exam requirement (NREMT 2005). o Nevada The rate of those passing the NREMT exam in Nevada to date is 50 percent. Some people opt out of the training because they do not want to take the national test, or drop out at the time of the test. The class commitment is 110 hours of class time plus 10 hours of clinical experience. Soon the State may add components on Weapons of Mass Destruction and Incident Command. Adding this material would enable the State to apply for additional Federal funds; however, it will further increase the burden of recruiting and retaining personnel. o Nebraska D. Challenges at the Primary Workplace Volunteer EMT's report that responding during work hours is a problem. Some employers are reluctant to have employees leave their jobs. There are particular occupations where leaving is especially difficult, if not impossible; for example, classroom teachers or certain medical personnel. Hourly employees and those doing shift work report a loss of income while they are away from their job, as do self-employed volunteers. Distance to and from workplaces is frequently responsible for a squad's inability to respond to a call because EMT's away at work can't get to the ambulance quickly enough (Ullrich, Mueller and Shambaugh-Miller 2004). One informant from rural New York Stated that 20 years ago volunteers were more abundant, as there were more businesses that allowed employees to take time for EMS response. Now there are fewer large businesses in the area, and the "Mom and Pop" operations often cannot afford to let their employees take the time to be an EMT during work hours. While some employers are reluctant to have employees leave during the workday to respond to emergencies, even more are unsupportive of employees participating in long transports that take people away from the workplace for hours or even an entire workday. In Greeley County, Kansas, one informant stated that inter-facility transfers are more burdensome than emergency runs, due to the time involved. Until recently, their regular transport was to a town 90 miles away; now they sometimes transport to a town 170 miles away, because of perceived quality of care issues. It is anticipated that this will cause problems for both the volunteers and their employers. One example of extreme distances may be found in the St. John's Valley of northern Maine. A patient transfer to Bangor takes 7 to 8 hours roundtrip, in good weather, and they occur two to three times a week. EMS volunteers are paid $150 per trip for transfer to Bangor. In Nebraska, more than one-third of volunteers
found it difficult to get time off from their job to go on EMS calls.
The Nevada study showed that more rural respondents (28 percent)
said getting time off for EMS-related duties was difficult compared
to urban residents (16 percent). E. Maintaining Skills in Low Volume Services The infrequency of calls for service in small communities is another challenge for frontier and rural EMT's. Respondents repeatedly commented on the irony that, while patient acuity and the length of transports are often greater in rural areas, the more highly trained personnel are in urban areas. Long transport times challenge the lower skill levels of rural providers. In Nebraska, 15 percent of the EMS squads responded to 25 or fewer calls during 2003. In Nevada, some of the small services respond to only 12 to 30 calls per year. Low volume services need frequent training and hands-on opportunities for maintaining skills. Frontier and rural EMS squads are less likely than urban squads to have personnel qualified at the Advanced Life Support (ALS) or paramedic level. The "rural ALS paradox" or "paramedicine paradox," or lack of advanced skills in EMS squads in rural and frontier areas, is in part a result of the low volume environment (McGinnis 2004). Higher levels of training and certification are harder to maintain with insufficient practice. Further, all EMS services have the same
high fixed costs regardless of call volume. Low volume services
cannot generate sufficient revenues to pay for the higher levels
of training and commitment of paramedics (Capitol Area Rural Health
Roundtable 2001).
In some States, all or most EMS workers are paid, while in other States a high percentage is volunteer. Programs in four States were reviewed as a sample of these differences. 1. High Percentage of "Paid" Workers Missouri Paid emergency medical service has been the tradition in Missouri, although as in other States, there are different levels of paid. All workers identified as "paid" are not necessarily paid a forty-hour per week wage. According to Steven Maxwell, Licensing Coordinator in the State Bureau of EMS, many years ago the State encouraged the development of advanced life support services and today 95 to 96 percent of Missouri's EMS providers offer advanced life support. In urban areas, ambulance services tend to be private; in rural areas they are often organized as ambulance districts with taxing authority and a six-member board. Most bill for services, but in some cases they rely only on tax revenue. Rural recruitment is becoming a bigger problem. This is especially true at the paramedic level with more intensive training requirements and better-paid jobs in urban areas. Missouri uses the National Registry exam, and at the EMT Basic level, the pass rate is lower than at the more advanced levels. The State is working to identify the underlying factors for these differences in exam passage. Staff at two frontier counties with ambulance districts, Chariton and Mercer, provided information for this report. According to USA Counties in Profile 2004, Chariton County has a population of 8142 people in a county of 755 square miles located in north central Missouri. Mercer County, located at the Iowa border of central Missouri has a population of 3618 in an area of 454 square miles. Both counties have lost substantial population over the last 35 years. Both ambulance districts derive their revenue from taxes supplemented by billing. Neither county has a hospital. Chariton County Ambulance District makes 30-minute transports to three small hospitals. Mercer County Ambulance District transports are to a hospital 25 miles away. Both offer advanced life support and train their staff in house. In the case of Chariton County, 25 volunteer first responders support the paid ALS units staffed by nurses and paramedics. According to Shane Grooms, Assistant Director of the Mercer County Ambulance District, when jobs become available, volunteers provide a pool of potential hires. Chariton County Ambulance District Superintendent William Pearman says recruiting workers is becoming more difficult especially at the advanced levels. He attributes this to both the isolated location and low pay. Tennessee In 1968, the Tennessee legislature gave local governments the authority to provide ambulance service, replacing the service supplied by funeral homes. In 1972, additional legislation established standards for ambulance services and consequently every county has an ambulance service. Tennessee ambulance service staff has been paid from the beginning. Because EMS is a required community service there is some property tax support, but most support comes from third party reimbursement. Joe Phillips, Director, Tennessee Division of Emergency Medical Services reported that most services are currently breaking even. Phillips described Tennessee as being in a unique situation geographically and demographically. Large cities, with tertiary care facilities and trauma centers, are situated across the State at a distance of 100-200 miles from each other. In addition there are three medical schools and five teaching hospitals in the State. Tennessee is bordered by eight States and has a large inflow of patients from five of those States (MS, AL, GA, KY and VA). Although Tennessee has no frontier counties much of the State is rural. It is one of several States that from the beginning have had an all paid EMS system for urban and rural communities.
Nebraska Nebraska's volunteer EMS services date back to the mid-1960s. In small communities across the State, various civic groups jumped in to provide ambulance service - fire departments, Jaycees, groups of citizens. They survived on bake sales and other local fundraisers. Today there are 423 volunteer ambulance services in a State of 1.7 million people. Eighty percent are volunteer services, some of which are affiliated with fire departments, others are stand-alone. According to Dean Cole, Director of the Nebraska Division of Emergency Medical Services, recruiting volunteers is a huge challenge, especially in areas where the population is elderly and sparse. Coverage during the day is the biggest problem. The State EMS office is helping some small communities join together in tiered services with priority dispatch, so one community can cover for another or more than one can respond if needed. Seward County is working with its 13 ambulance services to put them all under one license and insurance policy so they can respond to each other's calls. Tradition plays a role in maintaining many Nebraska services. They have been a valued part of the community for years. Historically, billing was not a high priority because the ambulance response was often provided at no charge. As payment for service becomes critical to maintain the more costly, modern EMS system, there is sometimes resistance on the part of the public to pay for something that was formerly "free". Shared professional billing services are emerging as a solution for small agencies that do not have the expertise to manage complicated billing procedures. Cole says Nebraska students do well on the National Registry exam. First responders have an 85 percent pass rate and all levels combined are at 80 percent. Nebraska has a proactive approach to training. They evaluated their training agencies and instructors and monitored those programs where students did well learning that successful instructors stick to the curriculum, test students often, have others monitor their style, and teach more than one class per year. Nebraska learned that students who failed the national test often had difficulty reading. So in advance of taking EMT classes, students must take a reading comprehension inventory prepared by the University of Nebraska-Lincoln Adult Education Department. While the overall class material is rated at an 8th grade level, required course readings are rated at 10th grade through college sophomore level. If students do not do well on the inventory, organizers urge that they first work on reading skills before beginning EMT training. The Nebraska EMS Division, in cooperation with the University of Nebraska-Lincoln, has developed eight online learning modules. Now, in addition to taking classes, students will be able to improve their preparation for the test using online materials. The EMS Division is also developing online courses for EMS instructors to help them become more effective when using telemedicine instructional technology. Based on the continued growth of minority populations, particularly Hispanics, the State EMS Division is beginning to look at second language issues. While minorities are encouraged to volunteer, many have very demanding work schedules, leaving little time for volunteering. Wisconsin Rural Wisconsin EMS relies heavily on volunteers. Wisconsin is a home rule State, and every municipality has the responsibility to provide its own EMS either directly or through a contractual arrangement. In urban areas, these services are staffed by full time paid providers. In rural areas, coverage tends to be by volunteers. Most volunteers receive some financial compensation for taking calls, for example, $10 per call or $50 per month. Since fewer volunteers are available during daytime hours, more services are paying a stipend for daytime service. Most ambulance services bill for services. In 2002, the Wisconsin EMS Association (WEMSA)
organized a Statewide effort to train individual ambulance services
how to recruit new volunteers. WEMSA had found that simply putting
out a call for volunteers was not effective. People failed to respond
because they tended to think they would respond later, were intimidated
by the responsibility and training, or perhaps had questions but
were reluctant to ask them. A new Statewide recruitment drive is being planned for 2006. The Wisconsin EMS Association has made their recruitment tools available to other agencies. 1. Paid and Volunteer: Two Communities with Shared Management St. John's Valley, Northern Maine Two adjacent towns located in frontier Aroostook County in the St. John's Valley of Northern Maine are each served by a town-operated ambulance service. Madawaska Ambulance Service is operated by all paid staff, the other, Ambulance Service Incorporated in Fort Kent, is primarily a volunteer service. The same person, John Labrie, manages both services. Madawaska. For twenty hours per week, Labrie manages a full time paid crew, including a paramedic. The crew is housed at the fire station in Madawaska, a paper mill town of 5000 residents. The emergency service has benefited in the past from support from local government and the mill, which needs an immediate response when there is an accident. Five years ago there was an extensive local government subsidy. This year Madawaska Ambulance Service, which has an annual budget of $350,000, collected $250,000 through billing and collections and expects to be self-sufficient next year. An outside private company does billing. Fort Kent. Labrie is also paid 16 hours per week to oversee the volunteer service in Fort Kent, Maine, a town 22 miles away. Labrie has a 0.5 FTE paid assistant in Fort Kent who helps manage the ambulance. Thirty-six volunteers and five ambulances serve an area of 15,000-17,000 people. Two ambulances are stationed at the Northern Maine Medical Center in Fort Kent, and one in each of three towns 20-30 minutes away. These "volunteers" are paid $2-3 hour for being on call and $25 for responding to a call. Volunteers are on call for three 24-hour shifts a week. Despite a strong tradition of volunteering in the area, it is becoming more difficult to recruit new volunteers. But tradition aside, Labrie says there has to be some remuneration for the amount of effort expected from these volunteers to compensate them for their time commitment and to improve retention. As stated previously, volunteers are currently paid a stipend for the 7-8 hour trip to transport patients to Bangor. In addition to Labrie, EMS coordinators in other States share his belief that EMS volunteering is far more demanding than most other types of volunteerism. Training is linked to the Northern Maine Community College in Presque Isle, about 60 miles away, and is paid for by Ambulance Service Incorporated. The training combines students traveling to Presque Isle, faculty coming to the hospital, and some lectures delivered by telemedicine. Fort Kent is located near the Canadian border and has a large French-speaking population. Prospective volunteers must pass an English language test prior to taking the EMT course, but clearly their bilingual skills are an asset. Labrie expects that eventually Fort Kent will have a fully paid service. Ambulance Service Incorporated has operated for 30 years and remains a volunteer service to keep costs down for the 12 small towns that together subsidize 25 percent of its operation. Labrie explained that if the ambulance service were staffed by full time paid EMT's, the budget would increase by 75 to 100 percent. Billing and collections has been moved to the billing department at Northern Maine Medical Center and the collection rate is improving. From his vantage point, Labrie says the quality of the two services is equal, but the response time of Madawaska is faster because paid staff are on duty at all times. The Kansas EMS office provided information on paid and volunteer workers in their 52 frontier counties. For the purpose of comparison they also provided the same information for the two largest counties. Data for 2005, 2000, and 1998 (the year they began collecting this data) was received. Unlike other States, frontier counties in Kansas have experienced increases in the numbers of volunteers since 1998 as well as increases in the numbers of paid personnel. The same pattern was true for the two urban counties. But those increases do not translate to increased worker availability. In some cases workers are kept on the roster even when they move. The experience of the following two frontier counties, exemplifies the difficulties faced largely by volunteer services in remote, sparsely populated areas of Kansas. Greeley County, Kansas Greeley County Ambulance is a completely volunteer service. Greeley County is located in western Kansas and has a population of 1500 people in a 778 square mile area. Although Greeley County Ambulance lists 21 volunteers on their roster, ten make about 90 percent of the runs. The county pays the service $7.00 per EMT per run, for up to four EMT's per run. These payments do not go to the volunteers but into an equipment and expense fund. The director receives $350 per month, recently increased from $156 per month. In addition to providing emergency care, Greeley County Ambulance transports patients to the hospital for tests, often without reimbursement. Recruiting new, active volunteers is an ongoing problem. Greeley County Ambulance pays for all training and certification fees. The county pays for most continuing education and reimburses students for their initial training. Students have 50 percent of the training costs reimbursed after passing the national exam and the remaining 50 percent after one year of service as an EMT. In the last two years, two courses were held and as a result five EMT's joined the ambulance service. Of these, two will leave for college within the next year so the net gain over two years is three volunteers. Economic pressures are believed to limit the involvement of new volunteers. Greeley County Ambulance is considering paying for on-call time and paying an hourly rate for transports directly to the techs. The national test is not a deterrent to volunteering, but after the initial National Registry test, most EMT's in Kansas maintain only their State certification, which has fewer requirements. One important issue is the need for higher levels of skill, especially in rural areas. The town of Tribune, where Greeley County Ambulance is based, has an 18-bed Critical Access Hospital. People living close to town and those whose medical needs can be served by that facility, have a quick transport. But for people further away, or for those who need a higher level of care, there is a long transport, and often those patients require more advanced skills during transport. Greeley County officials do not think it can afford a paid service. Billing is done by a volunteer who is paid a flat rate of $8 per claim, with no additional fee for follow-up and/or clarifications. Discussions with the county hospital billing department were initiated, but both the county commissioners and the ambulance service had issues with paying a higher fee. Sheridan County, Kansas Sheridan County is a 900 square mile county with about 2000 residents. A county-subsidized EMS program is based in Hoxie, Kansas where the Sheridan County Health Complex, a Critical Access Hospital, is located. Sheridan County EMS Director Debbie Kaufman says attracting volunteers is becoming increasingly difficult as the population decreases and EMS becomes more of a profession. Recently, Kaufman met with other members of the 18-county EMS region of northwest Kansas to discuss the extreme shortage of volunteers. There was a sense that in five years, without additional support or restructuring, they will not be able to continue to maintain volunteer services. Regionalization has been considered but, due to distances, there are concerns about the increased response times to reach patients. The county began financial support in 1975. Currently, the county provides one-third of the budget of Sheridan County EMS with the remaining two-thirds from billing and collections. The service fields about 200 calls per year, an average of four per week. One-third of the calls are transfers - 85 miles to Hays, Kansas, or 260 miles to either Wichita or Denver. Volunteers receive a trip reimbursement stipend. There are four EMT's in town, plus one first responder. A few EMT's in other parts of the county help out on an informal basis. C. Innovative Approaches to Maintaining Frontier EMS Research identified two models, which have been developed to help maintain and support frontier ambulance services. One model is the cross training of hospital staff as EMT's and the other is a creative funding mechanism used in Utah. Hospital cross training of staff has several advantages. The workers are already onsite and those that are selected for training have hospital jobs that can be interrupted. The training benefits the workers with additional career opportunities as well as providing additional EMS staff. Examples of two hospitals that provide emergency medical training to regular staff members in order to increase the availability of EMS workers follow. The State of Utah has tackled EMS funding in an unusual but effective way. Utah takes a creative approach to generating revenue by adding a surcharge on all criminal fines. Cross-Training Hospital Staff as EMT's 1. Owyhee Community Health Facility, Nevada The Owyhee Community Health Facility is a 15-bed hospital with a staff of 70 located on the Owyhee Indian reservation in frontier Elko County. The hospital provides EMS training annually to non-medical hospital workers. This approach has been successful and eight trained hospital workers are currently part of the ambulance service. When needed for an emergency, they are able to leave their regular position to assume emergency medical duties. Their rate of pay depends on the service they are providing. While working as an EMT, they are paid as an EMT; while working in their daily job, they are paid their regular salary. The ambulance averages 160 calls each year, with 75 percent of them being transfers to other facilities in larger communities such as Elko, Nevada (96 miles) or Boise, Idaho (142 miles). They respond to both reservation and non-reservation areas within a 50-mile radius, which crosses the Idaho/Nevada State line. 2. Margaretville Memorial Hospital, New York The ambulance service operated by Margaretville Memorial Hospital has a similar program in rural Delaware County, New York. The ambulance service area is approximately 706 square miles with a population of about 4200, with seasonal increases. Hospital staff members are offered EMT training, which is reimbursed by the State, and once licensed, they augment the EMT pool. During daytime hours, when working as EMT's they are paid their regular plus an extra hourly rate for time spent on a call. Nights and weekends are covered by on call staff paid a stipend. The hospital and staff are reported to be satisfied with this arrangement. Among the EMS-trained staff members, certain occupations are more available for emergency response than others. For example, a housekeeper is usually more readily available than an operating room technician. In the State of Utah, every criminal conviction carries a surcharge, a portion of which benefits EMS (Utah Code Section 63-63a-1). In 2005 the State EMS program received $2.5 million from these surcharges. These funds are used for administration, EMS training programs in high schools, competitive grants to ambulance services, and a per capita disbursement to counties. Many frontier and rural EMS services have used this source to purchase new ambulances and other equipment. D. Issues Related to Billing and Collections There was a great variability of knowledge about generating revenues through billing and collections among rural and frontier ambulance services. Many services do no billing at all and were therefore the least informed about the reimbursement system. At the other end of the spectrum are services that aggressively make every effort to capture all possible reimbursements. Some ambulance services turn the billing over to another department or agency and are not themselves informed about the billing and collection procedures. Outside billing services were generally reported as a positive solution to billing difficulties. These are often contractual relationships where the billing and collections are either performed by a private company, a local health provider or hospital. Experienced billing services provide efficiency, knowledge of the process and more orderly collection of fees. For example, the Wendover, Nevada ambulance is fully supported by its billing and collections. In order to insure that responders' narratives on run forms are complete and appropriate for billing Medicare and other payors, the service pays a $5 trip completion bonus each time the volunteers submit accurate and complete information.
In most cases, the decision to operate a volunteer ambulance service rather than a paid service is not a "choice," but based on real or perceived financial limitations. It was frequently stated that (a) local governments cannot afford to provide the service, or (b) operating a volunteer service holds costs down for the local government. In some rural areas, camaraderie and tradition are strong factors in keeping a volunteer service. Challenges to Staffing and Financial Sustainability Several issues were raised numerous times
and reflect current concerns of EMS staff working at both the State
and community level.
As systems change, one option is to work toward a blend of paid and volunteer EMT's within small ambulance services. There are a variety of types of blended systems. Blended Systems: Successful Models o One Paid Staff Person o Multiple Funding Sources o Shared Services Future Research Research on frontier and rural EMS needs to identify
methods to sustain EMS systems in small and/or geographically isolated
communities. While many frontier and rural communities are providing EMS using a number of creative staffing and financing solutions, other communities are increasingly at risk from an EMS system in distress. To inform policy, it is important that future research identify fragile communities and ways that they can become sustainable. Despite anecdotal evidence that frontier and rural communities experiencing population losses may have difficulty maintaining their EMS systems, the lack of data hinders the ability to help them. Future research focused on how to support frontier EMS might include:
Capitol Area Rural
Health Roundtable (2001). "Rural Cilluffo, F. J., D.
J. Kaniewski and P. M. Maniscalco (2005). Back
to the Future: An Agenda for Federal Leadership of Emergency Medical
Services. Erisman, G. (2005).
"Rural
Emergency Response - The Safety and Health Safety Net."
Available ( Fadali, E., Nolan, J., & Harris, T.
(2003). “ Journal of Emergency Medical Services (2004)."JEMS
2004 Platinum Resource Guide." Available ( Kansas Board of EMS, “EMS Board Registry Data,
2005,” Topeka, McGinnis, K. (2004), “Rural
and Frontier Emergency Medical Services: Agenda for the Future,”
Mears, G., Kagarise, J., Raiser, C., (2004).
"Rural Implications, Appendix 2 of the 2003 National Emergency
Medical Services (EMS) Survey." Minnesota Department of Health (2002). “A
Quiet Crisis: National Association of State National EMSC Data Analysis Resource Center (NEDARC), “2003 EMSC Data Collection System,” Available ( 4/01/05) at http://www.nedarc.org (no longer available). National
Registry of Emergency Medical Technicians (2001). State Office
Information. Available ( Nelsen, B.J., & Barley, S.R. (1997). “For Love or Money? Commodification and the Construction of an Occupational Mandate,” Administrative Science Quarterly, Vol. 42, No. 4, 619-653. National
Ullrich,
F, Mueller, K., & Shambaugh-Miller, M. (2004). “Emergency
Medical Services Volunteer Personnel in UND Rural UND Rural UND Rural UND Rural EMS Initiative
(no date). EMS
Recruitment and Retention Manual (online). USA
Counties in Profile. Available Utah Code, Title 63--Chapter 63a--Crime Victim Reparation Trust, Public Safety Support Funds, Substance Abuse Prevention Account, and Services for Victims of Domestic Violence Account. Available (8/11/05). Appendix A: Frontier and Rural Expert Panel PETER G. BEESON MARTIN BERNSTEIN PATRICIA CARR GAR ELISON CAROLINE FORD REBECCA SLIFKIN
Randy Cardonell, Volunteer Dean Cole, Director Pat Delameter, EMS Director Rosanna Gignac, EMS Coordinator Shane Grooms, Assistant Director Mary Hedges, Executive Director Don Hunjadi, Director Leslie Johnson, Program Manager, Certification
and Grants Program Debbie Kaufman, Director John Labrie, Director Jim Mayberry, EMS Program Manager Joe Moreland, Policy and Program Analyst William Pearman, Superintendent Kenny Pete, EMS Coordinator Joe Phillips, Director Garry Steele Dan Williams, Chief Gary Wingrove
Appendix C:
|
![]()
Go to:
Top
| HRSA | HHS
| Disclaimer | Accessibility
| Privacy