Cover Sheet - Background
- Methods - Results - Discussion
- Characteristics of Included Studies -
References - Tables &
Graphs
It has been postulated that early removal of bloody CSF by lumbar or ventricular tap might improve the prognosis of infants at risk of, or actually developing, PHH. The infants might benefit in terms of better neurological function because of reduced pressure and less periventricular edema. The physical removal of CSF containing blood and protein might allow the blocked pathways to be re-opened and re-establish normal CSF drainage. Removal of blood and protein might also prevent any inflammatory and fibrotic reaction and reduce the need for a permanent shunt.
Heterogeneity
An important issue is heterogeneity of the populations and/or intervention
between trials. Two trials (Mantovani 1980
and Anwar 1985) enrolled infants with IVH and
examined the effect of repeated lumbar puncture in preventing the development
of permanent hydrocephalus (as defined by ventriculoperitoneal shunt placement).Two
trials (Dykes 1989 and Ventriculomegaly 1990)
enrolled neonates with IVH who then went on to show progressive ventricular
dilatation. They examined the effect of lumbar punctures (Dykes
1989) or lumbar punctures or ventricular tapping (Ventriculomegaly
1990). The first approach is non-selective and allows earlier intervention
(which might, in theory, offer a better chance of success). The second
approach is selective but still means that some babies are treated who
would have resolved without shunting anyway. The second approach usually
means later treatment because one has to wait and see which IVH infants
will show progressive dilatation. A further point is that the Ventriculomegaly
trial used ventricular as well as lumbar tapping to achieve CSF drainage
whereas the other three trials used only lumbar puncture. Larger volumes
of CSF could be taken each time by ventricular tap than by lumbar puncture
but the potential for trauma and infection in the brain is probably greater
by the ventricular route. All four trials tackled the same question: does
repeated tapping of CSF reduce the risk of hydrocephalus? All four trials
attempted in their interventions to drain as much CSF as was practical.
For these reasons, we have examined them together.
Determination of outcomes:
1. Death during the period of follow-up was one outcome not liable
to bias
2. Insertion of a shunt was another major outcome. The indications
for shunt insertion varied somewhat in the wording used but they all required
a progressive increase in ventricular size despite a period of tapping.
This is a definition which is not likely to be biased although timing of
shunting could have been biased by knowledge of treatment allocation.
3. Neurodevelopmental outcome
Dykes 1989 had developmental outcome assessed at different ages by pediatric neurologists and a psychologist. The paper does not state whether they were blinded to early treatment allocation. The children were classified into 'major handicap' and "no major handicap". Those who had major handicap were further subdivided into those with a) 'single system disability' and b) those with 'multiple handicaps'. We extracted the numbers of children a) without major disability b) with a single disability c) with multiple disability.
In Ventriculomegaly 1990 virtually all the children were examined by one developmental pediatrician who was blind to early treatment allocation. Children were examined at 12 months post-term and at 30 months post-term. We extracted the numbers of children with single system disability and those with multiple impairments.
Impairments, disabilities and handicaps
The term 'handicap' may, in retrospect, have been used in rather an
imprecise way and it has been avoided in the analyses. Disability was taken
to mean a disturbance of function severe enough to prevent the child functioning
at an age appropriate level. Single system disability meant that the findings
were confined to one system of the nervous system eg a) hemiplegia without
mental retardation or b) sensorineural hearing loss.
The terms 'multiple handicap', 'multiple disability' or 'multiple impairments' were taken to mean clinically significant disturbances of function in different domains of the nervous system eg the combination of mental retardation, spastic diplegia, cortical blindness and epilepsy. When the figures for death or disability were calculated, the numbers of infants randomized but lost to follow-up were subtracted from the totals originally entered. Death or disability were mutually exclusive and thus could be aggregated.
MANTOVANI 1980
Method of randomization - alternation
Blinding of caretakers - no
Almost all subjects analyzed - yes
Blinding of observer - can't tell
ANWAR 1985
Method of randomization - random number table
Blinding of caretakers - no
Almost all subjects analyzed - yes
Blinding of observer - can't tell
DYKES 1989
Method of randomization - random number table
Blinding of caretakers - no
Almost all subjects analyzed - yes
Blinding of observer - can't tell
VENTRICULOMEGALY 1990
Method of randomization - telephone
Blinding of caretakers - no
Almost all subjects analyzed - yes
Blinding of observer - yes
Side effects of interventions:
Repeated CSF tapping of preterm infants carries a theoretical risk
of introducing infection. None of the infants in Dykes
1989 study developed CSF infection during tapping but 11 of the 157
infants in the Ventriculomegaly Trial developed CSF infections, all having
had some CSF taps (the infants in the control group were eventually tapped
if they developed symptoms or signs of raised intracranial pressure). CSF
infection (meningitis/ventriculitis) is a serious adverse effect of early
repeated CSF tapping. There is no information about the frequency of needle-track
lesions from repeated ventricular taps.
Many infants need few, if any, CSF taps but continue to expand their ventricles and heads at a rate which is clearly above normal. If this excessive expansion continues over 6 weeks observation, shunt surgery should be considered. The surgeon may wish to postpone surgery if the infant is still extremely small, if there is infection or if the CSF still has visible blood or high protein. If it has been necessary to tap the CSF repeatedly because of symptoms, then the case for earlier shunt surgery is stronger because repeated CSF taps, particularly ventricular taps, create morbidity.
Another therapeutic approach beginning to be evaluated is intraventricular fibrinolytic therapy, the object being to lyse fibrin and so open up the CSF reabsorption pathways. There is now a separate Cochrane review on intraventricular streptokinase after intraventricular hemorrhage. The available evidence suggests that fibrinolytic intervention relatively late (2 - 4 weeks after the IVH) is ineffective and current research is directed at understanding the early processes which initiate the process of fibrosis around the ventricular system (Whitelaw 1997; Whitelaw 1999).
| Study | Methods | Participants | Interventions | Outcomes | Notes | Allocation concealment |
| Anwar 1985 | Open randomized clinical trial | Preterm infants with grade 3 or 4 intraventricular hemorrhage on ultrasound scan | Daily lumbar puncture starting at 7 - 10 days. CSF was drained until flow stopped. Lumbar punctures were continued until the ventricular size decreased, remained unchanged for 2 consecutive weeks or if the infant developed hydrocephalus requiring a ventricular drain or shunt. | Hydrocephalus was defined as a progressive increase in ventricular
size as measured by ultrasound, in association with either signs of increased
ICP or an increase in head circumference >2 cm/week for at least 2 weeks.
Death before discharge from hospital. Death. |
A random number table was used. | B |
| Dykes 1989 | Open randomized clinical trial using random number tables | Neonates with asymptomatic severe posthemorrhagic hydrocephalus | Daily lumbar punctures, taking enough CSF to lower the CSF pressure by half. Volumes ranged from 2 - 21 ml. Duration 1 - 3 weeks. | Hydrocephalus management failure was defined as increasing head circumference,
progressive decrease in cortical mantle ( eg occipital cortical mantle
< 1 cm), signs of raised ICP.
Death during follow-up. Assessment at 3 - 6 years into no major handicap, single system disability and multiple disability. |
It is not stated whether the paediatric neurologists and the psychologist were blind to early treatment allocation. | B |
| Mantovani 1980 | Open clinical trial with alternation of treatment | Infants weighing less than 2000g with grade 2 or 3 intraventricular hemorrhage on CT scan | Daily lumbar punctures starting 24 hours after diagnosis of IVH. 3 - 5 ml of CSF was removed daily. Lumbar punctures were continued until the CSF was clear and protein concentration was < 180 mg/dl. | Hydrocephalus was defined as 2 CT scans with progressively enlarging
ventricles.
Death before discharge from hospital. |
Not true randomization. It is not stated if the observers of outcome were blind to early treatment allocation. | C |
| Ventriculomegaly 90 | Open randomized multicentre clinical trial at 15 neonatal intensive care units in England, Ireland and Switzerland. Randomization by telephoning and registering the infant before hearing the allocation. | Neonates with intraventricular haemorrhage, with progressive increase in ventricular size and whose ventricular width had increased to 4 mm over the 97th centile. | Repeated lumbar puncture taking as much CSF as possible, maximum 2 % body weight carried out daily or less frequently to prevent further increases in ventricular size. If not more than 2 ml of CSF could be obtained, ventricular tapping was carried out in the same way and often enough to hold the ventricular width constant. | Permament shunting was carried out if there was failure to control
head size despite medical management or if repeated tapping was necessary
for more than 4 weeks.
Death during follow up. Neurodevelopmental assessment was carried out at 12 months post term. Neurodevelopmental status examined at 30 months by a developmental pediatrician. Death during follow-up. |
The developmental pediatrician assessing the survivors at 12 and 30 months was blind to early treatment allocation. | A |
| Study | Reason for exclusion |
| Kreusser 1985 | Not a controlled trial |
| Lipscomb 1983 | Not a controlled trial |
| Papile 1980 | Not a controlled trial |
Anwar M, Kadam S, Hiatt IM, Hegyi T. Serial lumbar punctures in prevention of post-hemorrhagic hydrocephalus in preterm infants. J Pediatr 1985;107:446-450.
Dykes 1989 {published data only}
Dykes FD, Dunbar B, Lazarra A, Ahmann PA. Posthemorrhagic hydrocephalus in high risk infants: Natural history, management and long-term outcome. J Pediatr 1989;114:611-8.
Mantovani 1980 {published data only}
Mantovani JF, Pasternak JF, Mathew OP, Allen WC, Mills MT, Casper J, Volpe JJ. Failure of daily lumbar punctures to prevent the development of hydrocephalus following intraventricular hemorrhage. J Pediatr 1980;97:278-281.
Ventriculomegaly 90 {published data only}
* Ventriculomegaly Trial Group. Randomized trial of early tapping in neonatal posthaemorrhagic ventricular dilatation. Arch Dis Child 1990;65:3-10.
Ventriculomegaly Trial Group. Randomized trial of early tapping in neonatal posthaemorrhagic ventricular dilatation: results at 30 months. Arch Dis Child 1994;70:129-36.
Kreusser KL, Tarby TJ, Kovnar E, Taylor DA, Hill A, Volpe JJ. Serial lumbar punctures for at least temporary amelioration of neonatal posthemorrhagic hydrocephalus. Pediatrics 1985;75:719-24.
Lipscomb 1983 {published data only}
Lipscomb A, Thorburn R, Stewart A, Reynolds E, Hope P. Early treatment for rapidly progressive posthaemorrhagic hydrocephalus. Lancet 1983;i:1438-9.
Papile 1980 {published data only}
Papile LA, Burstein J, Burstein R, Koffler H, Koops BL, Johnson JD. Post-hemorrhagic hydrocephalus in low-birthweight infants: treatment by serial lumbar punctures. J Pediatr 1980;97:273-7.
* indicates the primary reference for the study
Hill A, Shackleford GD, Volpe JJ. A potential mechanism of pathogenesis for early posthemorrhagic hydrocephalus in the premature newborn. Pediatrics 1984;73:19-21.
Hudgins RJ, Boydston WR, Hudgins PA, Adler SR. Treatment of intraventricular hemorrhage in the premature infant with urokinase. A preliminary study. Pediatr Neurosurg 1994;20:190-7.
Levene MI. Measurement of the growth of the lateral ventricle in preterm infants with real time ultrasound. Arch Dis Child. 1981;56:900-4.
Punt J. Neurosurgical management of hydrocephalus. In: Levene MI, Lilford RJ, editor(s). Fetal and neonatal neurology and neurosurgery. Edinburgh: Churchill Livingstone:661-6.
Whitelaw A, Rivers R, Creighton L, Gaffney P. Low dose intraventricular fibrinolytic therapy to prevent posthaemorrhagic hydrocephalus. Arch Dis Child 1992;67:F12-4.
Whitelaw A, Saliba E, Fellman V, Mowinckel M-C, Acolet D, Marlow N. Phase 1 study of intraventricular recombinant tissue plasminogen activator for treatment of posthaemorrhagic hydrocephalus. Arch Dis Child. 1996;74:F20-26.
Whitelaw A. Intraventricular streptokinase after intraventricular hemorrhage in newborn infants (Cochrane Review). In: The Cochrane Library, Issue 4, 1997. Oxford: Update Software.
Whitelaw A, Christie S, Pople I. Transforming Growth Factor beta-1: a possible signal molecule for posthemorrhagic hydrocephalus. Pediatr Res 1999;46:576-580.
Whitelaw A, Kennedy CR, Brion LP. Diuretics for newborn infants with posthemorrhagic ventricular dilatation (Cochrane Protocol). In: The Cochrane Library, Issue 2, 2000. Oxford: Update Software.
Whitelaw A. Repeated lumbar or ventricular punctures in newborns with intraventricular hemorrhage (Cochrane Review). In: The Cochrane Library, Issue 3, 1998. Oxford: Update Software.
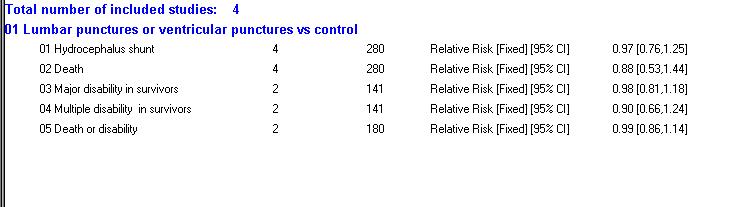
01.01 Hydrocephalus shunt
01.02 Death
01.03 Major disability in survivors
01.04 Multiple disability in survivors
01.05 Death or disability