Inhaled versus systemic corticosteroids for the treatment of
chronic lung disease in ventilated very low birth weight preterm infants
Shah SS, Ohlsson A, Halliday H, Shah VS
Dates
Date edited: 17/08/2007
Date of last substantive update: 03/08/2007
Date of last minor update: / /
Date next stage expected 03/08/2009
Protocol first published: Issue 2, 2000
Review first published: Issue 2, 2003
Contact reviewer
Dr Vibhuti S Shah
Staff Neonatologist
Department of Paediatrics
Mount Sinai Hospital
Room 775A
600 University Avenue
Toronto
Ontario CANADA
M5G 1X5
Telephone 1: 416 586 4816
Telephone 2: 416 664 6708
Facsimile: 416 586 8745
E-mail: vshah@mtsinai.on.ca
Contribution of reviewers
Sachin Shah: performance of literature search, identification of studies, abstraction of the data, analysis of data and writing of the review.
Arne Ohlsson: writing of the protocol, identification of studies (literature search), abstraction of data, analysis of data and editing of the review.
Henry Halliday: writing of protocol, identification of studies, abstraction of data, analysis of data and editing of review.
Vibhuti Shah: writing of the protocol, identification of studies (literature search), abstraction of data, analysis of data and editing of the review.This update was conducted by Vibhuti Shah and Arne Ohlsson.
Internal sources of support
Mount Sinai Hospital, Toronto, Ontario, CANADA
External sources of support
NoneWhat's new
This updates the review "Inhaled versus systemic corticosteroids for the treatment of chronic lung disease in ventilated very low birth weight preterm infants" published in The Cochrane Library Issue 2, 2003 (Shah 2003).For this update, one additional trial was identified and included in this review.
The conclusions of the review did not change.
Dates
Date review re-formatted: / /
Date new studies sought but none found: / /
Date new studies found but not yet included/excluded: / /
Date new studies found and included/excluded: / /
Date reviewers' conclusions section amended: / /
Date comment/criticism added: / /
Date response to comment/criticisms added: / /
Text of review
Synopsis
Preterm babies (babies who are born before term, 40 weeks pregnancy) often need breathing support (ventilator support) for breathing difficulties. Babies who need breathing support for a prolonged period of time often develop chronic lung disease (CLD). It is thought that inflammation in the lungs may be part of the cause. Corticosteroid drugs when given orally or through a vein reduces this inflammation (swelling) in the lungs and are used to treat such conditions. However, the use of corticosteroids is associated with serious side effects. Its use has been associated with cerebral palsy (motor problem) and developmental delay. Inhaling steroids, so that the drug directly reaches the lung, has been tried as a way to limit adverse effects. This review of trials found that inhaled steroids do not offer any advantages. More research is needed to show whether any form of routine use of steroids results in overall health improvements for babies at risk of CLD.
Abstract
Background
Chronic lung disease (CLD) remains a serious and common problem among very low birth weight infants despite the use of antenatal steroids and postnatal surfactant therapy to decrease the incidence and severity of respiratory distress syndrome. Due to their anti-inflammatory properties, corticosteroids have been widely used to treat or prevent CLD. However, the use of systemic steroids has been associated with serious short and long-term adverse effects. Administration of corticosteroids topically through the respiratory tract might result in beneficial effects on the pulmonary system with fewer undesirable systemic side effects.
Objectives
To determine the effect of inhaled versus systemic corticosteroids administered to ventilator dependent preterm neonates with birth weight < 1500 g or gestational age < 32 weeks after two weeks of life for the treatment of evolving CLD.
Search strategy
Randomized and quasi-randomized trials were identified by searching the Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library, Issue 3, 2007), MEDLINE (1966 - June 2007), EMBASE (1980 - June 2007), CINAHL (1982 - June 2007), reference lists of published trials and abstracts published in Pediatric Research or electronically on the Pediatric Academic Societies website (1990 - April 2007).
Selection criteria
Randomized or quasi-randomized trials comparing inhaled versus systemic corticosteroid therapy (irrespective of the dose and duration of therapy) starting after the first two weeks of life in ventilator dependent very low birth weight preterm infants.
Data collection & analysis
Data were extracted regarding clinical outcomes including CLD at 28 days or 36 weeks postmenstrual age (PMA), mortality, combined outcome of death or CLD at 28 days of age or 36 weeks PMA, other pulmonary outcomes and adverse effects. All data were analyzed using RevMan 4.2.10. When appropriate, meta-analysis was performed using relative risk (RR), risk difference (RD), and weighted mean difference (WMD) along with their 95% confidence intervals (CI). If RD was statistically significant, the number needed to treat (NNT) was calculated.
Main results
Data from one additional trial were available for inclusion in this update. Thus, five trials comparing inhaled versus systemic corticosteroids in the treatment of CLD were identified. Two trials were excluded as both included non-ventilator dependent patients and three trials qualified for inclusion in this review.
Halliday et al (Halliday 2001) randomized infants at < 72 hours, while Rozycki et al (Rozycki 2003) and Suchomski et al (Suchomski 2002) randomized at 12 - 21 days. The data from the two trials of Rozycki et al and Suchmoski et al are combined using meta-analytic techniques. The data from the trial by Halliday et al are reported separately, as outcomes were measured over different time periods from the age at randomization.
In none of the trials was there a statistically significant difference between the groups in the incidence of CLD at 36 weeks PMA among all randomized infants. The estimates for the trial by Halliday et al (Halliday 2001) were RR 1.10 (95% CI 0.82, 1.47), RD 0.03 (95% CI -0.08, 0.15); number of infants (n = 292).
For the trials by Rozycki et al (Rozycki 2003) and Suchomski et al (Suchomski 2002) the typical RR was 1.02 (95% CI 0.83, 1.25) and the typical RD 0.01 (95% CI -0.11, 0.14); (number of infants = 139 ). There were no statistically significant differences between the groups in either trial for oxygen dependency at 28 days of age, death by 28 days or 36 weeks PMA, the combined outcome of death by or CLD at 28 days or 36 weeks PMA, duration of intubation, duration of oxygen dependence, or adverse effects. Information on the long-term neurodevelopmental outcomes was not available.
Reviewers' conclusions
This review found no evidence that inhaled corticosteroids confer net advantages over systemic corticosteroids in the management of ventilator dependent preterm infants. Neither inhaled steroids nor systemic steroids can be recommended as standard treatment for ventilated preterm infants. There was no evidence of difference in effectiveness or side-effect profiles for inhaled versus systemic steroids. A better delivery system guaranteeing selective delivery of inhaled steroids to the alveoli might result in beneficial clinical effects without increasing side-effects. To resolve this issue, studies are needed to identify the risk/benefit ratio of different delivery techniques and dosing schedules for the administration of these medications. The long-term effects of inhaled steroids, with particular attention to neurodevelopmental outcome, should be addressed in future studies.
Background
Chronic lung disease (CLD) remains a serious and common problem among very low birth weight infants despite the use of antenatal steroids (Crowley 2002) and postnatal surfactant therapy (Yost 2002; Soll 2002) to decrease the incidence and severity of respiratory distress syndrome. The incidence of CLD varies between 23 - 26% (Lee 2000; Lemons 2001) in very low birth weight infants (< 1500 g) and has an inverse relationship to both gestational age and birth weight (Sinkin 1990; Lee 2000).
Several randomized controlled trials (Avery 1985; CDTG 1991; Cummings 1989; Harkavy 1989; Kazzi 1990; Ohlsson 1992) and systematic reviews (Shah 2001; Halliday 1999; Halliday 2002a; Halliday 2002b) have demonstrated that among infants with CLD, treatment with systemic corticosteroids facilitates extubation and improves respiratory system compliance. Marked heterogeneity regarding the dose and duration of dexamethasone administration has been noted among trials. However, corticosteroids appear to have little effect on the duration of supplemental oxygen, the duration of hospitalisation or mortality (Avery 1985; CDTG 1991; Harkavy 1989; Kazzi 1990; Ohlsson 1992). There are concerns regarding the short and long-term side effects of systemic steroids in this population. These include hyperglycemia, hypertension, hypertrophic cardiomyopathy, gastrointestinal hemorrhage and perforation, enhanced catabolism and growth failure, nephrocalcinosis, poor bone mineralization and susceptibility to infection (Ng 1993; Stark 2001).
The potential effects on brain growth and neurodevelopment are most alarming. Animal models (rat and rhesus monkey) at a similar stage of ontogeny to the human fetus have shown that steroids permanently affect brain cell division, differentiation, and myelination, as well as the ontogeny of cerebral cortical development (Johnson 1979; Weichsel 1977). These effects are long-lasting and associated with decreased head circumference and neuromotor abnormalities. Several follow-up studies of postnatal systemic corticosteroid therapy in preterm infants have shown a higher incidence of neurodevelopmental abnormalities in surviving dexamethasone treated infants (O'Shea 1999; Shinwell 2000; Yeh 1998).
In recent statements released by the European Association of Perinatal Medicine (Halliday 2001a), American Academy of Pediatrics (CFN/AAP 2002) and the Canadian Pediatric Society (FNC/CPS 2002), routine use of systemic dexamethasone for the prevention or treatment of CLD is not recommended. Outside the context of randomized, controlled trials, the use of corticosteroids should be limited to exceptional clinical circumstances. This recommendation was based on concerns regarding short and long-term complications, especially cerebral palsy.
Thus, alternatives to systemic corticosteroids that may have fewer adverse consequences need to be investigated. Administration of corticosteroids topically through the respiratory tract might result in beneficial effects on the pulmonary system with fewer undesirable systemic side effects.
This review aimed to examine the effectiveness of inhaled versus systemic corticosteroids administered to ventilator dependent very low birth weight neonates of 1500 g or less after the first two weeks of life, for the treatment of evolving CLD.
Objectives
The primary objective was to compare the effectiveness of inhaled versus systemic corticosteroids administered to ventilator dependent preterm neonates with birth weight < 1500 g or gestational age < 32 weeks after two weeks of life on the incidence of CLD at 36 weeks corrected postmenstrual age (PMA)
Secondary objectives were to compare the effectiveness of inhaled versus systemic corticosteroids on:
1. Other indicators of CLD including:
- Requirement for supplemental oxygen at 28 days of age
- Duration of requirement for supplemental oxygen (days)
- Duration of assisted ventilation (days)
- Duration of hospitalization (days)
- Change in pulmonary function tests (lung compliance and resistance)
2. The incidence of adverse events including:
- Mortality (expressed as neonatal mortality by 28 days of age or by 36 weeks PMA)
- Hyperglycemia (defined as a blood glucose of > 10 mmol/l) during the course of intervention
- Hypertension [defined as systolic or diastolic blood pressure > 2 standard deviations (SD) above the mean for infant's gestational and postnatal age (Zubrow 1995)] during the course of intervention
- Gastrointestinal hemorrhage (defined as presence of bloody nasogastric or orogastric aspirate)
- Necrotizing enterocolitis (NEC) (Bell's stage II and III) (Bell 1978)
- Intraventricular hemorrhage (IVH) any grade [defined as per Papile et al (Papile 1978)]
- Periventricular leucomalacia (PVL) (defined as cysts in the periventricular area on US or CT scan)
- Retinopathy of prematurity (ROP) any grade based on the international classification (ICROP 1984)
- Patent ductus arteriosus (PDA) defined by presence of clinical symptoms and signs and/or demonstration by echocardiography
- Hypertrophic cardiomyopathy defined as thickening of the intraventricular septum and/or of the left ventricular wall on echocardiography
- Sepsis defined by the presence of clinical symptoms and signs of infection and a positive culture from a normally sterile site
- Pneumonia based on clinical and radiological signs and a positive endotracheal tube aspirate culture
- Growth (weight, length/height and head circumference) at 36 weeks PMA
- Cataracts (defined by presence of opacities in the lens)
- Hypertrophy of the tongue
- Nephrocalcinosis (defined by the presence of echodensities in the medulla of the kidney on ultrasound) (Saarela 1999)
- Suppression of the hypothalamic-pituitary-adrenal axis assessed by metyrapone or ACTH stimulation test
3. Long-term neurodevelopmental outcome: Neurodevelopmental impairment is defined as presence of cerebral palsy and/or mental retardation [Bayley Scales of Infant Development (BSID), Mental Development Index (MDI) < 70] and/or legal blindness (< 20/200 visual acuity) and/or deafness (aided or < 60 dB on audiometric testing) assessed at 18-24 months.
Criteria for considering studies for this review
Types of studies
Randomized or quasi-randomized clinical trials.
Types of participants
Ventilator dependent preterm infants with birth weight < 1500 g or gestational age < 32 weeks and postnatal age of more than two weeks.
Types of interventions
Inhaled versus systemic corticosteroid therapy (irrespective of the dose or duration of therapy).
Types of outcome measures
Studies reported on at least one of the following outcomes:
1. Amongst all randomized:
- CLD at 36 weeks PMA (defined as requirement for supplemental oxygen at 36 weeks PMA)
- CLD at 28 days of age (defined as requirement for supplemental oxygen at 28 days of age)
- Death by 36 weeks PMA
- Death by 28 days of age
- Death by or CLD at 36 weeks PMA
- Death by or CLD at 28 days of age
- Additional administration of systemic corticosteroids
- Adverse events: infection, hyperglycemia, hypertension, gastrointestinal bleeding, cataracts, IVH, PVL, NEC, ROP, PDA and suppression of hypothalamic-pituitary-adrenal axis
2. Amongst survivors:
- CLD at 36 weeks PMA
- CLD at 28 days of age
3. Long-term neurodevelopmental outcome: Neurodevelopmental impairment is defined as presence of cerebral palsy and/or mental retardation [Bayley Scales of Infant Development (BSID), Mental Development Index (MDI) < 70] and/or legal blindness (< 20/200 visual acuity) and/or deafness (aided or < 60 dB on audiometric testing) assessed at 18 - 24 months.
Search strategy for identification of studies
Randomized controlled trials comparing inhaled versus systemic corticosteroid therapy in preterm neonates were identified from MEDLINE (1996 - June 2007) using MeSH headings: infant-newborn, chronic lung disease, bronchopulmonary dysplasia, anti-inflammatory agents, steroids, dexamethasone, administration, inhalation; aerosols, budesonide, beclomethasone dipropionate, flunisolide and fluticasone propionate.
Other databases were searched including: Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library, Issue 3, 2007), EMBASE (1980 - June 2007), CINAHL (1982 - June 2007), reference lists of published trials, and abstracts published in Pediatric Research or electronically on the Pediatric Academic Societies website (1990 - June 2007). No language restrictions were applied. For the original review, the articles were screened by four review authors (SS, VS, AO, HH) to identify articles eligible for inclusion in the review. For this update, two review authors (VS, AO) conducted the literature search and have reviewed the articles obtained.
Methods of the review
Criteria and methods used to assess the methodological quality of the trials: the standard method of Cochrane Collaboration and its Neonatal Review Group was used. For each trial, information was sought regarding the method of randomization, blinding and reporting of outcomes of all infants enrolled in the trial. Data from the primary investigator were obtained for unpublished trials or when published data were incomplete. Retrieved articles were assessed and data abstracted independently by four review authors (SS, VS, AO, HH). The update of this review was performed by two review authors (VS, AO). Discrepancies were resolved by discussion and consensus. The statistical analyses used were relative risk (RR), risk difference (RD), and weighted mean difference (WMD) when appropriate along with their 95% confidence intervals (CI). If RD was significant, number needed to treat (NNT) was calculated. A fixed effect model was used for meta-analysis. Heterogeneity tests [including the I squared (I2) test] were to be performed to assess the appropriateness of pooling the data.
Description of studies
Five trials comparing inhaled versus systemic corticosteroids in treatment of CLD were identified. Two trials (Dimitriou 1997; Nicholl 2002) were excluded as both included non-ventilator dependent patients and the groups of ventilated infants could not be identified separately. Three trials fulfilled the inclusion criteria and are included in this updated review: Halliday et al (Halliday 2001), Suchomski et al (Suchomski 2002) and Rozycki et al (Rozycki 2003) (published since our initial review). Even though Rozycki et al (Rozycki 2003) enrolled preterm infants with birth weights between 650 - 2,000 g, on review of the published data, 93% of the subjects enrolled had birth weights < 1,000 g with PMA ranging from 23 - 31 weeks. Therefore, the data from this trial are included in this review. Each of these trials have been published as a full text article. Details of each trial are given in the table "Characteristics of included studies".
Halliday et al (Halliday 2001) - This trial enrolled infants born at < 30 weeks gestation, postnatal age < 72 hours, needing mechanical ventilation and fractional inspired oxygen concentration (FiO2) > 0.30. Infants of 30 and 31 weeks could also be included if they needed FiO2 > 0.50. Infants with lethal congenital anomalies, severe IVH (grade 3 or 4), or proven systemic infection before entry were excluded from the trial. The trial was designed to evaluate the effectiveness of early (< 72 hours) or delayed (> 15 days) administration of systemic dexamethasone or inhaled budesonide. Infants were randomly allocated to one of four treatment groups in a factorial design: early (< 72 hours) dexamethasone, early budesonide, delayed selective (> 15 days) dexamethasone and delayed selective budesonide. Only the delayed budesonide and delayed dexamethasone groups are included in this review. One hundred and forty two babies were randomized to the delayed selective budesonide policy while 150 were randomized to the delayed selective dexamethasone policy. Budesonide was administered by metered dose inhaler and a spacing chamber in a dose of 400 µg/kg twice daily for 12 days. Dexamethasone was given intravenously (IV) or orally (PO) in a tapering course beginning with 0.5 mg/kg/day in two divided doses for three days reducing by half every three days for a total of 12 days of therapy. Delayed selective treatment was started if infants needed mechanical ventilation and more than 30% oxygen for > 15 days. Out of 142 infants randomized to the delayed selective budesonide group, 33 received a full course, 21 received a partial course while 88 did not receive budesonide. Out of 150 infants randomized to the delayed selective dexamethasone group, 35 received a complete course, 25 received a partial course while 90 infants did not receive dexamethasone. An intention to treat analysis was performed by the investigators in their report of this study, and by us in this review. The primary outcome was death or oxygen dependency at 36 weeks. Secondary outcome measures included death or major cerebral abnormality, duration of oxygen treatment, and complications of preterm birth.
Suchomski et al (Suchomski 2002) - This trial compared inhaled beclomethasone, either 400 or 800 µg/d, to intravenous dexamethasone in preterm infants dependent on conventional mechanical ventilation and supplemental oxygen at two weeks of age. Seventy eight preterm infants with birth weight < 1500 g, gestational age < 30 weeks and ventilatory dependence at 12 - 21 days of age with rate > 15/min and FiO2 > 0.30 with a persistence of these ventilator settings for a minimum of 72 hours were included in the study. Infants on high frequency ventilation were ineligible for the study. Infants were excluded from the study if they had major congenital malformations, culture proven sepsis, hypertension or hyperglycemia needing treatment, or persistent patent ductus arteriosus. Infants were randomly assigned to one of the three treatment groups: inhaled beclomethasone at 400 µg/d, at 800 µg/d, or intravenous dexamethasone. Inhaled beclomethasone was continued until extubation. Post-extubation the same dose was continued for another 48 hours. After that, the dose was halved every other day for six days, after which the steroids were stopped. Based on our inclusion criteria (to include all studies regardless of dosage of inhaled steroids), and because there was no significant difference in the effects of the two different doses, the two inhaled beclomethasone groups in the trial by Suchomski et al (Suchomski 2002) were combined to form one group in the present review. Intravenous dexamethasone was given as a 42 day tapering course starting with 0.5 mg/kg/day in two divided doses (Avery 1985). Crossover from either of the inhaled beclomethasone groups to intravenous dexamethasone was allowed if after four to five days of inhaled beclomethasone, the infant's ventilator and oxygen support had not decreased and the attending neonatologist felt that the infant could benefit from intravenous dexamethasone. Eighteen infants from the inhaled steroid group crossed over to systemic dexamethasone. An intention to treat analysis was performed by the investigators in their report of this study, and by us in this review. Outcome measures included adverse effects like sepsis, hypertension and hyperglycemia; short term ventilatory requirements, duration of mechanical ventilation, duration of supplemental oxygen, length of stay in the hospital and need for respiratory support at 28 days or 36 weeks PMA. For infants completing a 10 day course of either inhaled or intravenous steroids, an ACTH (adrenocorticotropic hormone) stimulation test was done two weeks after completion of the steroid course.
Rozycki et al (Rozycki 2003) enrolled 61 preterm infants with birth weights between 650 - 2,000 g if at 14 days of age they were at significant risk of developing moderate to severe CLD, defined as the need for mechanical ventilation and oxygen, along with X-ray changes beyond 28 days of life. Infants with culture proven sepsis and who were receiving FiO2 of > 0.30 were eligible if they had a ventilatory index (10,000/Ventilator rate x peak pressure x pCO2) of < 0.8. Infants without previous sepsis were eligible if the ventilatory index was < 0.51. Infants meeting these criteria had a 75% risk of developing moderate-severe CLD. Infants with the following conditions were excluded: preexisting hyperglycemia with blood glucose > 200 mg/dl for > 24 hours, hypertension with systolic pressures > 70-90 mm Hg, depending on birth weight, surgery within previous seven days, active bacterial infection unless repeat blood, urine or cerebrospinal fluid cultures were sterile after 72 hours of antibiotics, thrombocytopenia with a platelet count of < 100,000, any gastrointestinal bleeding within the previous seven days, significant weaning from ventilator support in the previous three days and previous exposure to postnatal steroids. Eligibility was determined at 14 days of age but the study could be delayed up to six days while awaiting resolution of infections. Infants were randomized to the following four groups: Group A: aerosol placebo-systemic dexamethasone; Group B: high beclomethasone-systemic placebo; Group C: medium beclomethasone-systemic placebo; and Group D: low beclomethasone-systemic placebo. Those receiving aerosol steroids who remained ventilator-dependent after seven days were switched to standard 42-day tapering doses of systemic dexamethasone. The primary outcome variable was extubation within the first seven days of the study. Secondary outcome measures included: changes in ventilatory settings and oxygen delivery over the first 7 days, the incidence of hypertension, hyperglycemia, infection and growth.
Methodological quality of included studies
Halliday et al (Halliday 2001) - This was a multicentre randomized controlled trial involving 47 centres. The interventions and outcome measures were not blinded in all the centres. However, in 11 centres the trial was conducted double blind. In these centres, placebo metered dose inhalers and intravenous saline were used to mask treatment allocation. After identifying an eligible infant, the clinician telephoned the randomization centre to enroll the infant and determine the treatment group. Outcomes were reported for all infants enrolled in the study. Comparisons were also made for the primary outcome variables between the centres observing double blind strategy and the other centres.
Suchomski et al (Suchomski 2002) - This was a prospective randomized controlled trial. Three sets of 27 cards were assembled followed by placement of one card each into one of 81 opaque envelopes. As infants were enrolled, a card was sequentially pulled and the infant assigned to the appropriate study group. Blinding of intervention was not performed. Blinding of outcome measurement was not ensured. Cross-over from inhaled steroid groups to intravenous dexamethasone was allowed at the discretion of attending neonatologist. Outcome measures were reported for all babies enrolled in the study.
Rozycki et al (Rozycki 2003) - This was a prospective randomized double-blind controlled trial. The infants were randomized using a random table number and only the pharmacy was aware of the individual group assignment. Blinding of intervention was performed. Blinding of outcome measurement was not ensured. Outcome measures were reported for all infants enrolled in the study.
Results
The data from two trials (Rozycki 2003; Suchomski 2002) were combined for meta-analysis, while the data from the study by Halliday 2001are presented separately due to clinical differences between these trials. Halliday et al (Halliday 2001) randomized infants < 72 hours, while Suchomski et al (Suchomski 2002) randomized at 12 - 21 days and Rozycki et al (Rozycki 2003) randomized after 14 days. Each trial reported outcomes from the age of randomization. Although the infants received steroids after the first two weeks of life in all these trials, the time period over which outcomes were measured differed between the studies.
INHALED VS. SYSTEMIC STEROIDS (INFANTS RANDOMIZED BETWEEN 12-21 DAYS OF AGE) (COMPARISON 01):
PRIMARY OUTCOMES:
CLD at 36 weeks PMA (Outcome 01.01):
Two trials enrolling 139 neonates reported on the incidence of CLD at 36 weeks PMA. There was no statistically significant difference in the incidence of CLD by 36 weeks PMA in the inhaled steroid compared to systemic steroid group [typical RR 1.02 (95% CI 0.83, 1.25); typical RD 0.01 (95% CI - 0.11, 0.14)]. There was high heterogeneity for this outcome for RR (p=0.03, I2=80%) and for RD (p=0.02, I2=81%).
SECONDARY OUTCOMES:
CLD at 28 days of age (Outcome 01.02):
One trial enrolling 78 neonates reported on the incidence of CLD at 28 days of age. There was no statistically significant difference in the incidence of CLD at 28 days of age [RR 0.97 (95% CI 0.90, 1.05), RD - 0.04 (95% CI -0.12, 0.04)].
Death by 36 weeks PMA (Outcome 01.03):
One trial enrolling 78 neonates reported on the incidence of death by 36 weeks PMA. There was no statistically significant effect on death by 36 weeks PMA [RR 2.69 (95% CI 0.13, 54.15), RD 0.04 (95% CI -0.04, 0.12)].
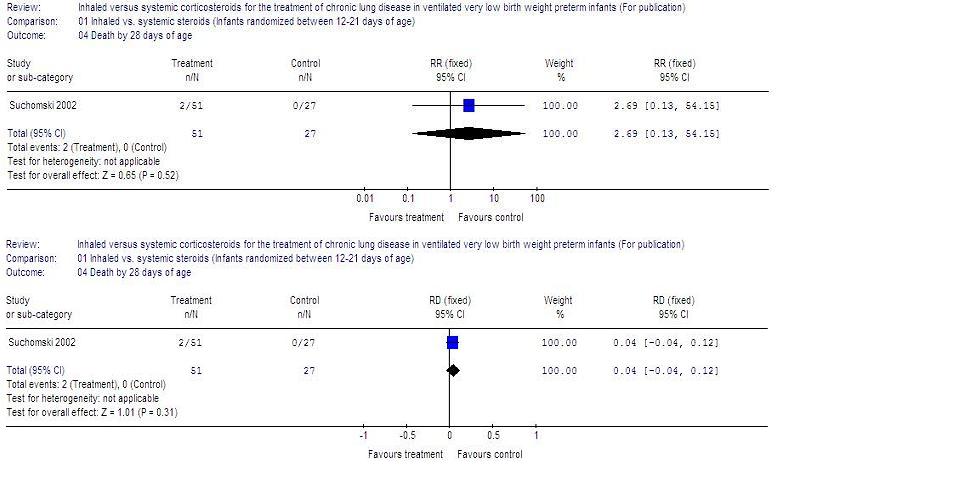
Death by 28 days of age (Outcome 01.04):
One trial enrolling 78 neonates reported on the incidence of death by 28 days. No statistically significant effect on mortality by 28 days was noted [RR 2.69 (95% CI 0.13, 54.15), RD
0.04 (95% CI 0.04, 0.12)].
Death by or CLD at 36 weeks PMA (Outcome 01.05):
One trial enrolling 78 neonates reported on the incidence of death by or CLD at 36 weeks PMA. There was no statistically significant difference between the groups for the combined outcome of death by or CLD at 36 weeks PMA [RR 0.94 (95% CI 0.83, 1.05), RD -0.06 (95% CI -0.17, 0.05)].
Death by or CLD at 28 days of age (Outcome 01.06):
One trial enrolling 78 neonates reported on the incidence of death by or CLD at 28 days. All enrolled infants (51 in the inhaled steroid group and 27 in the systemic steroid group) had this outcome and therefore the RR was not estimable. The RD for this outcome was 0.00 (95% CI -0.06, 0.06).
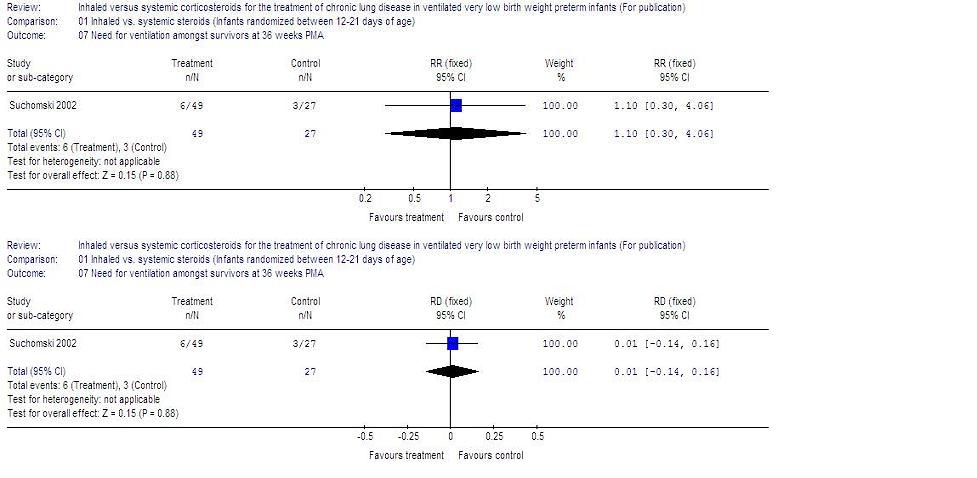
Need for ventilation amongst survivors at 36 weeks PMA (Outcome 01.07):
One trial reported on this outcome (n=76). There was no statistically significant difference for this outcome between groups [RR 1.10 (95% CI 0.30, 4.06), RD 0.01 (95% CI -0.14, 0.16)].
Duration mechanical ventilation among survivors (days) (Outcome 01.08):
One trial reported on this outcome for 77 neonates. The duration of mechanical ventilation was not statistically significantly different between groups (MD - 3 days, 95% CI -16, 10).
Duration of supplemental oxygen amongst survivors (days) (Outcome 01.09):
One trial reported on this outcome for 76 neonates. The duration of supplemental oxygen was not statistically significantly different between the two groups (MD -15 days, 95% CI
-37, 7).
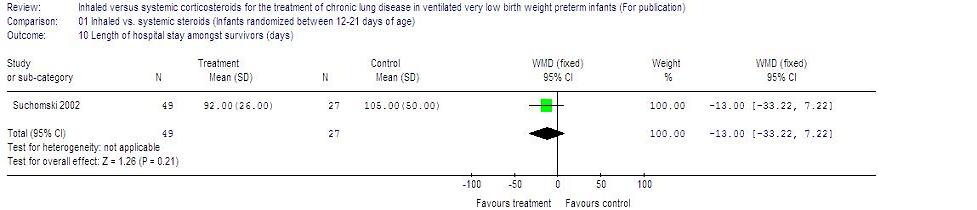
Length of hospital stay amongst survivors (days) (Outcome 01.10):
One trial reported on this outcome for 76 neonates. There was no statistically significant difference in the length of hospital stay amongst survivors between groups (MD -13, 95% CI -33, 7).
Hyperglycemia (Outcome 01.11):
Two trials enrolling 139 neonates reported on the incidence of hyperglycemia. There was no statistically significant difference in the incidence of hyperglycemia between groups [typical RR 0.33 (95% CI 0.05, 2.12); typical RD -0.04 (95% CI -0.11, 0.04)]. There was low heterogeneity for this outcome for RD (p=0.17, I2=47%).
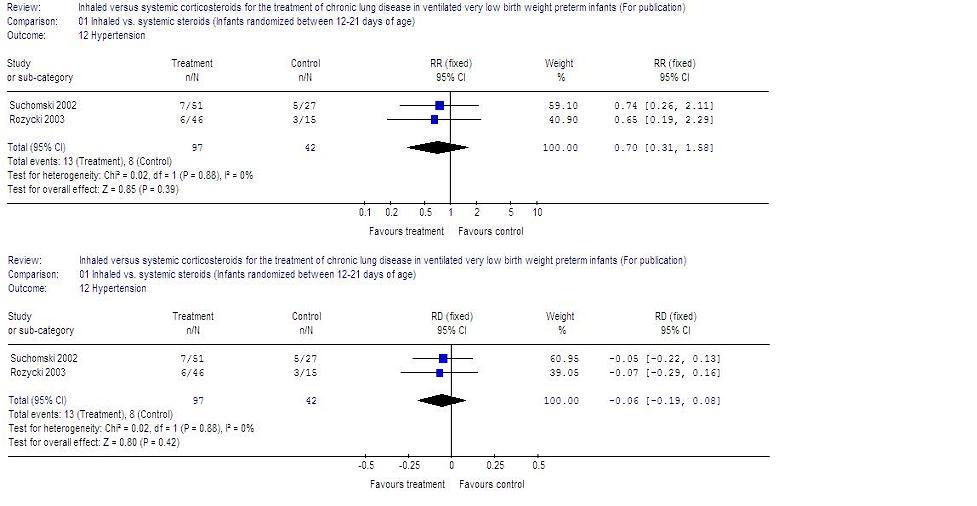
Hypertension (Outcome 01.12):
Two trials enrolling 139 neonates reported on the incidence of hypertension. There was no statistically significant difference in the incidence of hypertension between groups (typical RR 0.70, 95% CI 0.31, 1.58; typical RD -0.06, 95% CI -0.19, 0.08). There was no heterogeneity for this outcome for RR (p=0.88, I2=0%) and for RD (p=0.88, I2=0%).
Necrotizing enterocolitis (Outcome 01.13):
One trial enrolling 78 neonates reported on the incidence of NEC. There was no statistically significant difference in the incidence of NEC between groups (RR 2.12, 95% CI 0.25, 18.02; RD 0.04, 95% CI -0.06, 0.14).
Gastrointestinal bleed (Outcome 01.14):
One trial enrolling 78 neonates reported on the incidence of gastrointestinal bleed. None of the enrolled infants had this outcome and therefore the RR was not estimable. The RD was -0.00, 95% CI -0.06, 0.06).
Periventricular leucomalacia (Outcome 01.15):
Two trials enrolling 139 neonates reported on this outcome. There was no statistically significant difference in the incidence of periventricular malacia between groups (typical RR 0.83, 95% CI 0.33, 2.08; typical RD -0.02, 95% CI -0.15, 0.10 ).
Retinopathy of prematurity > stage 3 (Outcome 01.16):
Two trials enrolling 139 neonates reported on the incidence of ROP > stage 3. There was no statistically significant difference in the incidence of ROP > stage 3 between groups (typical RR 1.33, 95% CI 0.64, 2.74; typical RD 0.06, 95% CI -0.08, 0.21). There was no heterogeneity for this outcome for RR (p=0.59, I2= 0%) and for RD (p=0.62, I2=0%).
Culture proven sepsis (Outcome 01.17):
One trial enrolling 78 neonates reported on this outcome. There was no statistically significant difference in the incidence of culture proven sepsis between groups (typical RR 1.24, 95% CI 0.35, 4.4; RD 0.03, 95% CI -0.13, 0.18).
INHALED VS. SYSTEMIC STEROIDS (INFANTS RANDOMIZED AT < 72 HOURS OF AGE) (COMPARISON 02):
PRIMARY OUTCOME:
CLD at 36 weeks PMA (Outcome 02.01):
One trial enrolling 292 neonates reported on the incidence of CLD at 36 weeks PMA. There was no statistically significant difference in the incidence of CLD at 36 weeks PMA in the inhaled steroid compared to systemic steroid group [RR 1.10 (95% CI 0.82, 1.47); RD 0.03 (95% CI - 0.08, 0.15)].
SECONDARY OUTCOMES:
CLD at 28 days of age (Outcome 02.02):
One trial enrolling 292 neonates reported on the incidence of CLD at 28 days of age. There was no statistically significant difference in the incidence of CLD at 28 days [RR 1.06 (95% CI 0.88, 1.26), RD 0.03 (95% CI -0.08, 0.15)].
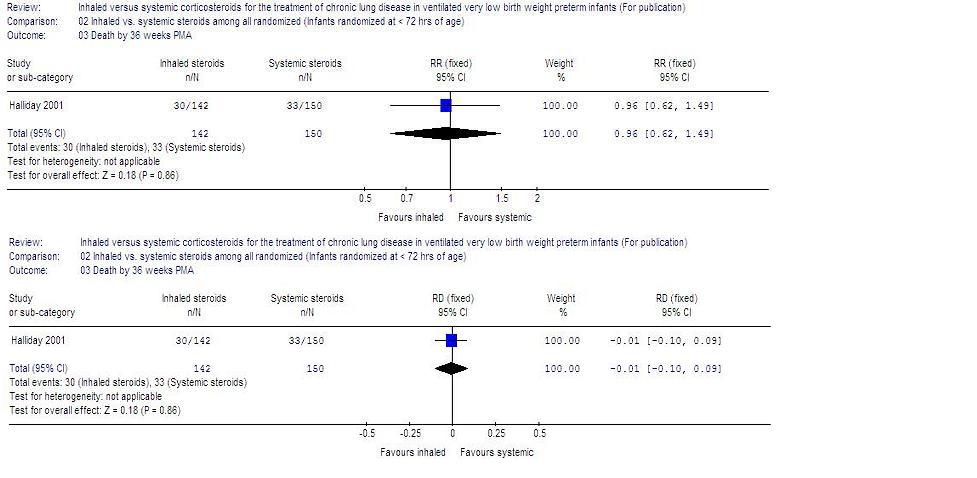
Death by 36 weeks PMA (Outcome 02.03):
One trial enrolling 292 neonates reported on the incidence of death by 36 weeks PMA. There was no statistically significant effect on death by 36 weeks PMA [RR 0.96 (95% CI 0.62, 1.49), RD -0.01 (95% CI -0.10, 0.09)].
Death by 28 days of age (Outcome 02.04):
One trial enrolling 292 neonates reported on the incidence of death by 28 days of age. No statistically significant effect on mortality by 28 days was noted [RR 0.85 (95% CI 0.52, 1.37), RD -0.03 (95% CI -0.12, 0.06)].
Death by or CLD at 36 weeks PMA (Outcome 02.05):
One trial enrolling 292 neonates reported on the incidence of death by or CLD at 36 weeks PMA. There was no statistically significant difference between the groups for the combined outcome of death by or CLD at 36 weeks PMA [RR 1.04 (95% CI 0.86, 1.26), RD 0.03 (95% CI -0.09, 0.14)].
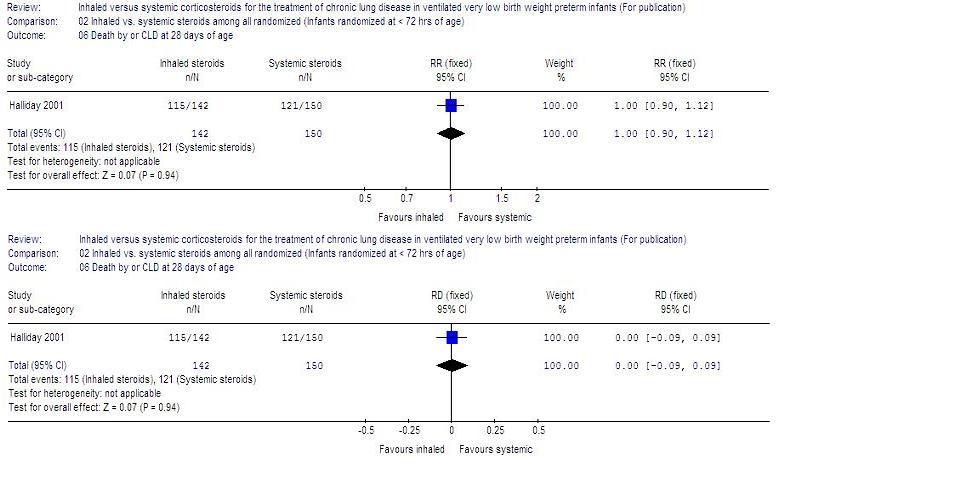
Death by or CLD at 28 days of age (Outcome 02.06):
One trial enrolling 292 neonates reported on the incidence of death by or CLD at 28 days of age. There was no statistically significant difference between the groups for the combined outcome of death by or CLD at 28 days of age [RR 1.00 (95% CI 0.90, 1.12), RD 0.00 (95% CI -0.09, 0.09)].
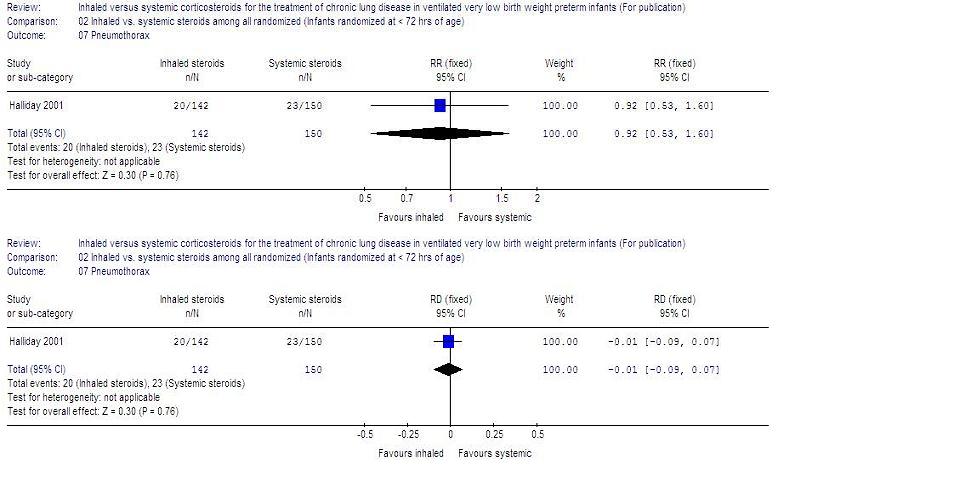
Pneumothorax (Outcome 02.07):
One trial reported on this outcome (n=292). There was no statistically significant difference for this outcome between groups [RR 0.92 (95% CI 0.53, 1.60), RD -0.01 (95% CI -0.09, 0.07)].
Other air leaks (Outcome 02.08):
One trial reported on this outcome (n=292). There was no statistically significant difference for this outcome between groups [RR 1.00 (95% CI 0.55, 1.83), RD 0.00 (95% CI -0.08, 0.08)].
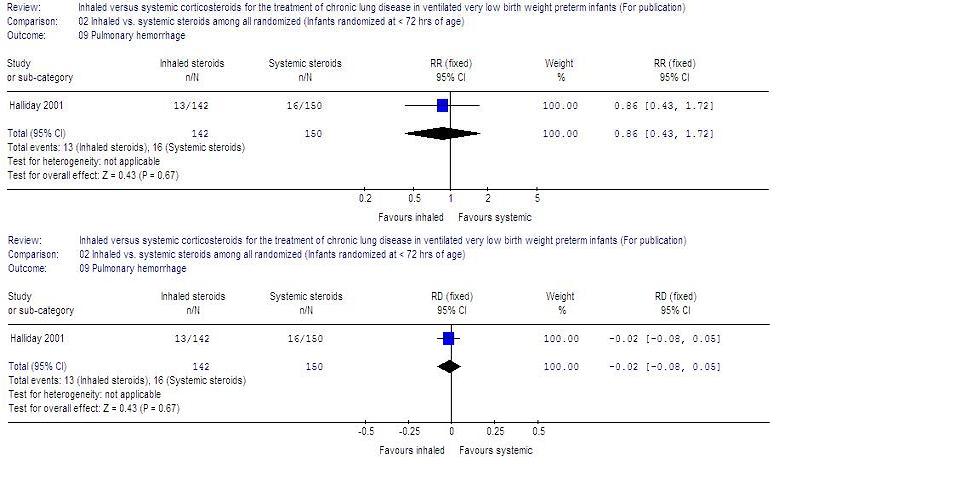
Pulmonary hemorrhage (Outcome 02.09):
One trial enrolling 292 neonates reported on this outcome. There was no statistically significant difference for this outcome between groups [RR 0.86 (95% CI 0.43, 1.72), RD -0.02 (95% CI -0.08, 0.05)].
Duration mechanical ventilation (days) (Outcome 02.10):
One trial reported on this outcome for 292 neonates. The duration of mechanical ventilation was not statistically significantly different between groups (MD 0.1 days, 95% CI -5.2, 5.4).
Duration of supplemental oxygen (days) (Outcome 02.11):
One trial reported on this outcome for 292 neonates. The duration of supplemental oxygen was not statistically significantly different between the two groups (MD 7 days, 95% CI
-17, 30).
Hyperglycemia (Outcome 02.12):
One trial enrolling 292 neonates reported on the incidence of hyperglycemia. There was no statistically significant difference in the incidence of hyperglycemia between groups (RR 0.90, 95% CI 0.63, 1.28; RD -0.03, 95% CI -0.14, 0.07).
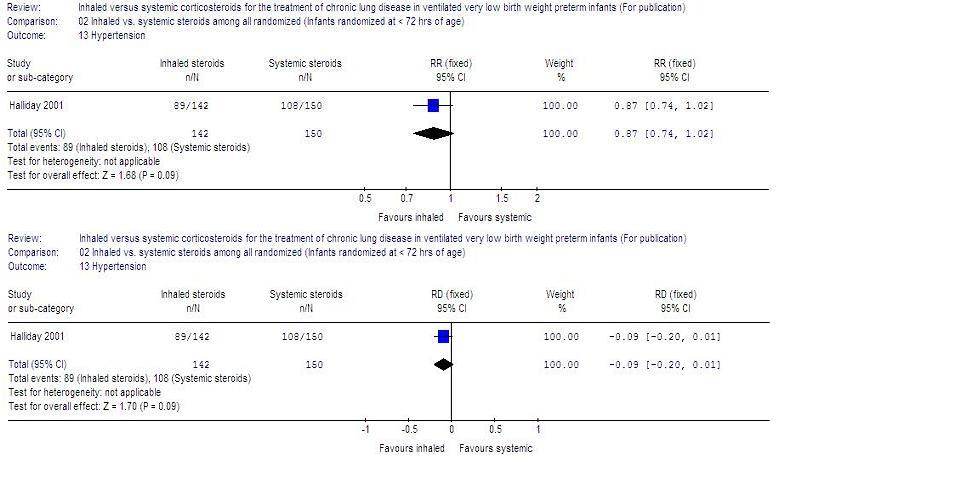
Hypertension (Outcome 02.13):
One trial enrolling 139 neonates reported on the incidence of hypertension. There was no statistically significant difference in the incidence of hypertension between groups (RR 0.87, 95% CI 0.74, 1.02; RD -0.09, 95% CI -0.20, 0.01).
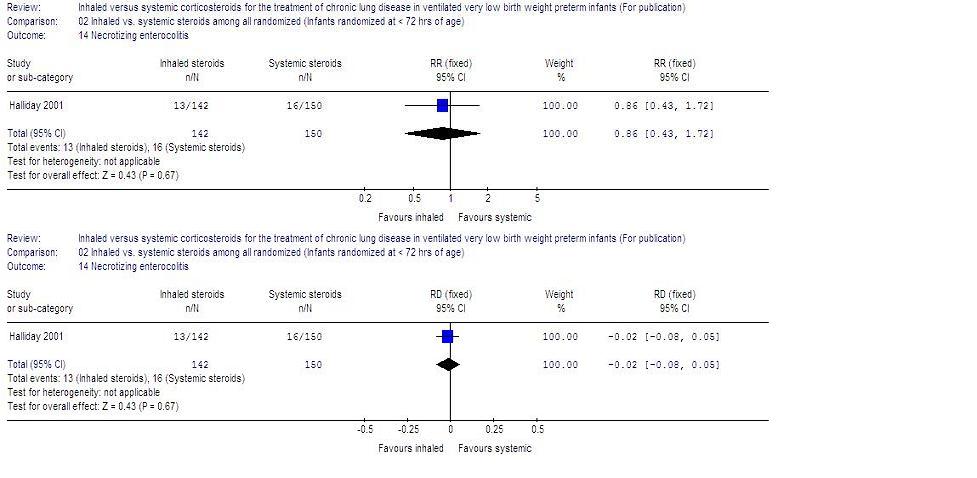
Necrotizing enterocolitis (Outcome 02.14):
One trial enrolling 292 neonates reported on the incidence of NEC. There was no statistically significant difference in the incidence of NEC between groups (RR 0.86, 95% CI 0.43, 1.72; RD -0.02, 95% CI -0.08, 0.05).
Gastrointestinal bleed (Outcome 02.15):
One trial enrolling 292 neonates reported on the incidence of gastrointestinal bleed. There was no statistically significant difference in the incidence of NEC between groups (RR 0.89, 95% CI 0.41, 1.93; RD -0.01, 95% CI -0.07, 0.05).
Gastrointestinal perforation (Outcome 02.16):
One trial enrolling 292 neonates reported on this outcome. There was no statistically significant difference in the incidence of gastrointestinal perforation between groups (RR 0.85, 95% CI 0.23, 3.08; RD -0.01, 95% CI -0.04, 0.03).
Patent ductus arterious (Outcome 02.17) :
One trial enrolling 292 neonates reported on this outcome. There was no statistically significant difference in the incidence of PDA between groups (RR 0.90, 95% CI 0.73, 1.11; RD -0.06, 95% CI -0.17, 0.06).
Retinopathy of prematurity, at any stage (Outcome 02.18):
One trial enrolling 292 neonates reported on the incidence of ROP at any stage. There was no statistically significant difference in the incidence of ROP groups (RR 1.27, 95% CI 0.86, 1.89; RD 0.06, 95% CI -0.04, 0.16).
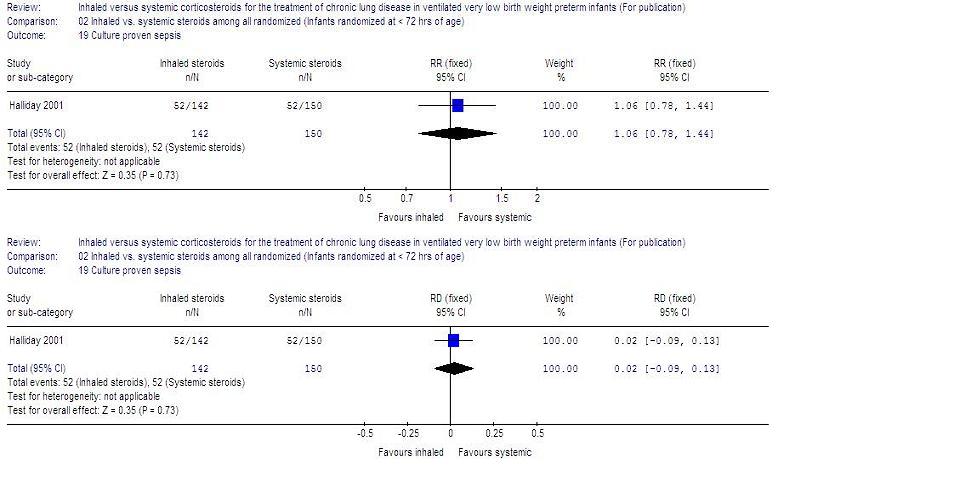
Culture proven sepsis (Outcome 02.19):
One trial enrolling 292 neonates reported on this outcome. There was no statistically significant difference in the incidence of culture proven sepsis between groups (RR 1.06, 95% CI 0.78, 1.44; RD 0.02, 95% CI -0.09, 0.13).
OTHER OUTCOMES:
ACTH stimulation test:
The ACTH test was completed in one trial (Suchomski 2002) on 24 infants. The baseline cortisol levels before the ACTH stimulation test for the 800 µg/d inhaled group (3 ± 2.3 µg/dl; n = 7) and the intravenous group (1.6 ± 1.3 µg/dl; n = 10) were statistically significantly lower than for the 400 µg/d inhaled group (7.3 ± 4.2 µg/dl; n = 7). However, the response to ACTH (i.e., relative rise in cortisol level) was similar in all the three groups: 12 ± 5.7 µg/dl in the 400 µg/d inhaled group, 15.6 ± 8.5 µg/dl in the 800 µg/d inhaled group and 10.7 ± 4.6 µg/dl in the intravenous group, p = 0.408. Post ACTH stimulation cortisol levels were 18.4 ± 8.0 µg/dl in the 800 µg/d inhaled group, 19.3 ± 5.9 µg/dl in the 400 µg/d inhaled group and 12.3 ± 5.7 µg/dl in the intravenous group, p = 0.048.
No relevant data for the following outcomes were available for analysis: long-term neurodevelopmental outcome, measurement of pulmonary functions, growth, nephrocalcinosis, hypertrophy of tongue, cataract, pneumonia or hypertrophic cardiomyopathy.
Discussion
This review found no evidence that inhaled as compared to systemic steroids decrease the incidence of CLD at 36 weeks PMA, CLD at 28 days of age, mortality by 28 days or 36 weeks PMA, or the combined outcome of death by or CLD at 28 days of age or 36 weeks PMA. There was no evidence of effect on the duration of ventilation, duration of oxygen supplementation or the incidence of adverse effects.
The data from the two trials (Rozycki 2003; Suchomski 2002) were combined as they enrolled infants between 12 - 21 days of age, while data from the trial by Halliday et al (Halliday 2001) were reported separately as they randomized infants < 72 hours of age. The period of measurement of outcomes varied between the studies by Halliday et al (Halliday 2001) and the other trials (Rozycki 2003; Suchomski 2002) making combination of results inappropriate. This may possibly explain the differences in the incidence of adverse events like CLD, mortality, etc. Halliday et al (Halliday 2001) counted deaths from < 72 hours onwards while Suchomski et al (Suchomski 2002) did so from 12 - 21 days onwards. This means that in Halliday 2001, all deaths from < 72 hours were attributed to the randomized treatment policy, whereas in Suchomski 2002, only deaths from 12 - 21 days were so attributed. Looking at the control event rate we see what we would expect - a much higher death rate in Halliday 2001 than in Suchomski 2002 (death by 36 weeks was 33/150 in Halliday 2001 and 0/27 in Suchomski 2002 ). Similar explanations could be provided for the other outcomes of interest. Due to these concerns, aggregation of the data in the two trials was not performed.
A systematic review (Halliday 2002a) of postnatal corticosteroid therapy begun after three weeks postnatal age showed a borderline significant decrease in incidence of CLD, but no evidence of effect on survival at discharge or duration of hospitalization. Also, systematic reviews of systemic postnatal corticosteroid therapy instituted between 7 -14 days postnatal age (Halliday 2002b, Shah 2001) showed a decrease in the incidence of CLD at 36 weeks PMA and mortality. However, the duration of hospitalization was not decreased.
A major concern with studies of inhaled steroid therapy is the uncertainty regarding drug delivery and deposition of steroids in the oropharynx and in the peripheral airways. Numerous factors affect drug delivery and deposition including the number of particles in the respirable range, the delivery technique (use of MDI with or without a spacer), nebulizers (jet or ultrasonic) and the presence or absence of an endotracheal tube. Previous workers have shown that the amount of aerosol delivery varies from 0.4% to 14% based on the technique used (Arnon 1992; Grigg 1992; O'Callaghan 1992). The delayed onset of activity (Dimitriou 1997; LaForce 1993) and a similar risk profile of inhaled steroids (Shah 2002) suggests that their effects may be secondary to systemic absorption.
Inhaled steroids are believed to be less effective compared to systemic steroids. The type, dosage and delivery methods may be inadequate. More refinements in the inhalational drug delivery system guaranteeing selective delivery in the alveoli and smaller airways may improve the clinical efficacy and decrease the side-effect profile of inhaled steroids. In the present review, there is no evidence of difference in effectiveness or side-effect profiles for inhaled versus systemic steroids. A better delivery system/higher dose of inhaled steroids may result in equivalence of effectiveness for the two modes of administration, but may also show evidence of side-effects. To resolve this issue, studies are needed to identify the risk/benefit ratio of different delivery techniques and dosing schedules for the administration of these medications.
This review found no evidence that inhaled steroids confer any net advantages over systemic steroids in the management of ventilator dependent preterm infants. Systemic steroids given late (after one week) do not show clear evidence of neurodevelopmental problems (Halliday 2002a; Halliday 2002b). However, systemic steroids, especially dexamethasone given early (< 96 hours), are associated with an increase in cerebral palsy (Halliday 2002c). Further studies with particular attention to long-term neurodevelopmental outcome need to be performed before delayed steroids, either inhaled or systemic, can be recommended as safe for treatment of evolving CLD in preterm infants. Follow-up studies are extremely important and all surviving infants in the OSECT study (Halliday 2001) are currently being traced and examined by pediatricians and psychologists.
Reviewers' conclusions
Implications for practice
This updated review of three trials found no evidence that inhaled corticosteroids confer net advantages over systemic corticosteroids in the management of ventilator dependent preterm infants. Neither inhaled nor systemic steroids can be recommended as standard treatment for ventilated preterm infants.
Implications for research
Studies are needed to identify the risk/benefit ratio of different delivery techniques and dosing schedules for the administration of steroids. Studies are needed to address the long-term effects of inhaled steroids, with particular attention to neurodevelopmental outcome.
Acknowledgements
We thank Dr. H. L. Halliday and Dr. Chris Patterson for providing additional data for the infants included in the 'OSECT" trial.
Potential conflict of interest
None
Characteristics of included
studies
| Study | Methods | Participants | Interventions | Outcomes | Notes | Allocation concealment |
| Halliday 2001 | Multicentre, randomized open study. 1. Blinding of randomization: Yes. 2. Blinding of intervention: Not in all centres.
11 centres - Yes; 36 centres - No 3. Blinding of outcome measurement: No 4. Complete follow up: Yes | 570 infants from 47 neonatal intensive care units worldwide (United Kingdom, Ireland, Canada, Switzerland, Norway, Greece, Portugal, Sweden, Slovenia, Poland, Singapore, UAE) were enrolled. Inclusion criteria: Gestational age < 30 weeks, postnatal age < 72 hours and need for mechanical ventilation and inspired FiO2 > 30%. Delayed selective treatment was started if infants needed mechanical ventilation and > 30% FiO2 for > 15 days. Infants of 30 - 31 weeks GA could also be included if they needed > 50% FiO2. Demographic data: values presented as mean (SD) or as appropriate Budesonide group
n = 142
Gestational age (weeks): 27 (2)
Birth weight (grams): 994 (279)
Gender (female/male) (number of infants): 64/78
Antenatal steroids (number and percentage): 89 (63%)
Surfactant treatment: 132 (93%)
Clinical Risk Index for Babies score: Median 6, Range 1-18 Dexamethasone group
n = 150
Gestational age (weeks): 27.1 (1.9)
Birth weight (grams): 1007 (283)
Gender (female/male) (number): 71/79
Antenatal steroids (number and percentage): 82 (55%)
Surfactant treatment (number and percentage): 138 (92%)
Clinical Risk Index for Babies score: median 7, range 1-16 Exclusion criteria: congenital lethal anomalies, severe IVH
(grade 3 or 4) and proven systemic infection before entry. A strong suspicion of infection, uncontrolled hypertension and hyperglycemia were considered to be indications to postpone trial entry until they resolved, provided that this occurred within 72 hours of birth. Study period: February 1994 to December 1998.
The trial had factorial design and a similar number of infants was allocated to each group. Group 1 received early
(< 72 hours) dexamethasone (n = 135); group 2 received delayed (> 15 days) dexamethasone (n = 150); group 3 received early budesonide (n = 143); Group 4 received delayed selective budesonide
(n = 142). | 1. Dexamethasone was administered IV or PO in initial dose of 0.5 mg/kg/day in 2 divided doses for 3 days, followed by 0.25 mg/kg/day in 2 divided doses for 3 days, then 0.10 mg/kg/day for 3 days, and finally 0.05 mg/kg/day in 2 divided doses for 3 days for a total of 12 days of treatment. 2. Budesonide was administered using a metered dose inhaler (MDI; 200µg/puff; Pulmicort, Astra Draco, Lund, Sweden) connected to spacing device (Aerochamber MV 15; Trudell Medical, Canada). The aerochamber was a rigid , clear plastic cylinder, 11 by 4.1 cm with an approximate capacity of 145 ml. After endotracheal suctioning, the MDI was shaken and inserted into the spacing chamber. The spacer was then filled with 100% oxygen and the infant's FiO2 was increased by 20%. The aerochamber was connected into the ventilatory circuit and manual inflations were given through the chamber using an inflatable bag. Budesonide was administered as soon as chest wall movements were established. A 500 -1000 g infant was given 2 puffs twice daily and 1000-1500 g infant was given 3 puffs twice daily. The puffs were given one at a time, activating MDI at end expiration and allowing 10 breaths after each activation. After each administration, the chamber was removed from the ventilator circuit and the infant was reconnected to the ventilator at the previous settings. The duration of budesonide treatment was up to 12 days provided the infant remained intubated. If the infant was extubated before 12 days budesonide was discontinued. | 1. Primary outcome measure was death or oxygen dependency at 36 weeks CGA. 2. Secondary outcome measures included death or major cerebral abnormality on ultrasound nearest to 6 weeks postnatal age, death or oxygen dependency at 28 days and expected date of delivery, duration >40% FiO2, duration of any supplemental oxygen, duration of assisted ventilation by endotracheal tube and duration of hospital stay. 3. Complications such as pneumothorax, other pulmonary air leaks, NEC, acquired pneumonia, PDA requiring treatment, pulmonary hemorrhage requiring increased ventilation, seizures treated with anticonvulsants, recurrent apnea needing treatment, ROP at 36 weeks CGA, gastric hemorrhage and GI perforation were noted. All neonates were monitored daily for blood pressure and blood glucose. Also, withdrawals from the intervention because of hypertension, hyperglycemia, sepsis, gastric bleeding, or intestinal perforation were noted. An intention to treat analysis was performed. | The study was performed double blind in 11 centres, and in these centres placebo MDIs and intravenous saline were used to mask treatment allocation. | A |
| Rozycki 2003 | Prospective randomized controlled trial.
1. Blinding of randomization: Yes
After parental consent, infants were stratified into two birth weight groups (650-1,000 grams and 1,001-2,000 g birth weight) and then into four dosing group using a random table number
2. Blinding of intervention: Yes
3. Blinding of outcome assessment: No
4. Complete follow up: Yes | 61 preterm infants with birth weights between 650-2,000 grams if at 14 days of age were at significant risk for developing moderate to severe CLD, defined as need for mechanical ventilation and oxygen, along with X-ray changes beyond 28 days of life were enrolled.
Infants with proven sepsis and receiving FiO2 of > or equal 0.3 and had a ventilatory index of < 0.8 were eligible while for infants without culture proven sepsis, the oxygen requirement was the same but the ventilatory index threshold was < 0.510. Demographic data: values presented as mean (SE) or as appropriate Group A: Dexamethasone group
n = 15
Birth weight (grams): 773 (132)
Gestational age (weeks): 26 (24-27)
Gender (male/female): 7/8
Prenatal steroids: 2/15
Inborn: 12
Prestudy sepsis: 8
Initial ventilation index: 0.252 (0.094) Group B: High dose beclomethasone group
n = 16
Birth weight (grams): 710 (148)
Gestational age (weeks): 26 (23-29)
Gender (male/female): 6/10
Prenatal steroids: 1/15
Inborn: 13
Prestudy sepsis: 10
Initial ventilation index: 0.300 (0.184) Group C: Medium dose beclomethasone group
n = 15
Birth weight (grams): 796 (152)
Gestational age (weeks): 26 (24-30)
Gender (male/female): 8/7
Prenatal steroids: 3/16
Inborn: 11
Prestudy sepsis: 7
Initial ventilation index: 0.294 (0.106) Group D: Low dose beclomethasone group
n = 15
Birth weight (grams): 760 (124)
Gestational age (weeks): 25 (24-31)
Gender (male/female): 9/6
Prenatal steroids: 2/15
Inborn: 13
Prestudy sepsis: 9
Initial ventilation index: 0.293 (0.158) | Infants were randomized into 4 groups:
Group A: aerosol placebo-
systemic dexamethasone
Group B: high dose beclomethasone-systemic placebo
Group C: medium dose beclomethasone-systemic placebo
Group D: low dose beclomethasone-systemic placeboDexamethasone group: 42 day course of dexamethasone as described by Avery et al followed by a 7 day course of placebo to ensure that all subjects ended the study at the same time.
Subjects in the aerosol steroid groups (B, C, or D) began a similar 42-day systemic dexamethasone course on day 8 if extubation was unsuccessful while on inhaled steroids. Aerosol steroid groups randomized to receive:
High dose beclomethasone group (2.4-3.69 micrograms/kg/day)
Medium dose beclomethasone group (1.0-1.85 micrograms/kg/
day)
Low dose beclomethasone group (0.48-0.74 micrograms/kg/
day) Beclomethasone dipropionate (42 micrograms/
actuation, Vanceril, Schering-Plough, Kenilworth, NJ) was administered using a metered dose inhaler (MDI) placed between the bag and the spacer. After disconnecting the ventilator circuit, a 250-ml Laerdal resuscitation
bag with oxygen resorvoir connected to an oxygen source (> 90% FiO2) was connected through a spacer to the endotracheal tube. After activating the MDI, infants were given three manual breaths. Infants < 1,001 grams at birth received one dose of beclomethasone every 12 hourly while larger infants received a dose every 8 hourly.
Inhaled steroids were administered for a maximum of 7 days. The medication was stopped if the infant was successfully extubated for more than 12 hours even if not all doses had been administered. | 1. Primary outcome measure was extubation within the first 7 days of the study 2. Secondary outcome measures included changes in ventilator settings and oxygen delivery
over the first 7 days. The rates of hypertension, hyperglycemia, infection and growth over the first 7 days were also analyzed. Long-term outcomes not included. | Infants were ventilated with time-cycled, pressure limited, nonsynchronized ventilators during this study. Ventilator management was prescribed during the first 2 weeks of the study. If the pCO2 was < 50 mm Hg, the peak pressure was lowered until it was < 15 cm H2O. Then, if the pCO2 was < 50 mm Hg, the ventilator rate was lowered, FiO2 was adjusted to maintain oxygen saturation between 88-92%. No subjects received bronchodilators during the study period. The use of caffeine or diuretics was left to the discretion of the attending physician. | A |
| Suchomski 2002 | Prospective randomized controlled trial.
1. Blinding of randomization: Yes
Random allocation using 3 sets of 27 assembled, opaque envelopes.
As infants were enrolled, a card was sequentially pulled and infant assigned to appropriate study group. In case of multiple gestation, all eligible siblings were assigned to same group to minimize parental anxiety.2. Blinding of intervention: No 3. Blinding of outcome measurement: No 4. Complete follow up: Yes | 78 preterm infants < or = 30 weeks, birth weight < or = 1500 g and conventional ventilator dependence at 12-21 days of age with rate > 15/min and FiO2 > 0.30 with persistence of these ventilator settings for a minimum of 72 hours were enrolled in the study. Demographic data: Values presented as mean (SD) or as appropriate Inhaled beclomethasone 800 µg/d group
n = 25
Gestational age (weeks): 26 (1)
Birth weight (grams): 843 (177)
Gender (female/male) (number of infants): 14/11
Maternal steroids (number and percentage): 12 (48%)
Age of commencement of steroids (days): 17 (3)
Baseline mean airway pressure: 7.1 (1.2)
Baseline FiO2: 0.44 (0.10) Inhaled beclomethasone 400 µg/day group
n = 26
Gestational age (weeks): 26 (2)
Birth weight (grams): 846 (139)
Gender (female/male) (number of infants): 12/14
Maternal steroids (number and percentage): 22 (84.6%)
Age of commencement of steroids (days): 18 (3)
Baseline mean airway pressure: 7.3 (1.9)
Baseline FiO2: 0.42 (0.13) Intravenous dexamethasone group
n=27
Gestational age (weeks): 26 (2)
Birth weight (grams): 843 (227)
Gender (female/male) (number of infants): 8/19
Maternal steroids (number and percentage): 16 (59.2%)
Age of commencement of steroids (days): 17 (2)
Baseline mean airway pressure: 7.9 (1.6)
Baseline FiO2: 0.49 (0.13)
Infants were ineligible if they were on high frequency oscillatory ventilation. Exclusion criteria: major congenital malformations, culture positive sepsis, hypertension which required medical management, persistent PDA, or hyperglycemia requiring insulin. Infants were also excluded if they received any postnatal steroid therapy (either inhaled or intravenous) before 12 days of age or before entry in the study. | 1. The inhaled beclomethasone was delivered through a metered dose inhaler with a spacer device (Aerovent) connected in line with the ventilator at 50 µg per puff. Between each puff, the infant was ventilated with 4 or 5 manual breaths delivered at a peak pressure identical to that delivered during mechanical ventilation.
The 400 µg/d group (n=26) received 4 puffs every 12 hours. The 800 µg/puff group (n=25) received 4 puffs every 6 hours. Beclomethasone was continued until extubation. If the infant was successfully extubated, then the same dose was administered for 48 hours more. Thereafter, the steroid dose was halved every other day for 6 days, after which the steroid was stopped. After extubation, the inhaled beclomethasone was given using a face mask with inhaler and spacer device.2. The intravenous dexamethasone group (n=27) received a 42 day tapering course (Avery 1985), starting with 0.5 mg/kg/day, divided every 12 hours. Cross over from either of the inhaled beclomethasone groups to intravenous dexamethasone was allowed if, after 4 to 5 days of inhaled beclomethasone, the infant's ventilator and oxygen support had not decreased and the attending neonatologist felt that the infant might benefit from intravenous dexamethasone. 3. All data were analysed according to original group assignment. | 1. Primary outcome measures: hypertension or hyperglycemia needing treatment or culture positive sepsis. 2. Other outcome variables: ventilatory settings, specifically rate, mean airway pressure (MAP), peak inspiratory pressure (PIP), positive end expiratory pressure (PEEP), and supplemental oxygen requirement every 6 hours daily on all enrolled patients starting from 5 days before initiation of steroid therapy and daily thereafter, until extubation. After extubation, the supplemental oxygen was recorded daily until patient was discharged or supplemental oxygen was discontinued. 3. The occurrence of the following was also recorded: IVH, PVL, NEC, ROP, GI bleed and death. 4. For babies who completed at least a 10 day course of either inhaled or intravenous steroids, an ACTH stimulation test was done 2 weeks after completion of steroid course. The test was completed in 24 neonates and the morning cortisol levels were noted before and one hour after intravenous bolus of 36 µg/kg synthetic ACTH
(Cortrosyn, Organon, West Orange, NJ). | Sample size was determined by assuming a rate of adverse effects (as defined by sepsis or hyperglycemia or hypertension requiring treatment) of 80% in intravenous steroid -treated infants. The sample size was calculated to detect a 30% difference in adverse effects at 80% power and p < 0.05.
There was a statistically significant difference between the groups regarding some maternal characteristics such as maternal steroid use and need for caesarean section. | A |
Abbreviations:
CGA: corrected gestational age
IVH: intraventricular hemorrhage
MDI: metered dose inhaler
NEC: necrotising enterocolitis
PDA: patent ductus arteriosus
PIP: peak inspiratory pressure
PEEP: positive end expiratory pressure
PO: per orally
ROP: retinopathy of prematurity
Characteristics of excluded studies
| Study | Reason for exclusion |
| Dimitriou 1997 | The authors included non ventilator dependent infants and the age of commencement of steroids varied from 5 to 118 days of life. |
| Nicholl 2002 | Non-ventilator dependent infants were included in the study. |
References to studies
References to included studies
Halliday 2001 {published data only}Halliday HL, Patterson CC, Halahakoon CW. A multicenter, randomized open study of early corticosteroid treatment (OSECT) in preterm infants with respiratory illness: comparison of early and late treatment and of dexamethasone and inhaled budesonide. Pediatrics 2001;107:232-40.
Rozycki 2003 {published data only}
Rozycki HJ, Byron PR, Elliott GR, Carroll T, Gutcher GR. Randomized controlled trial of three different doses of aerosol beclomethasone versus systemic dexamethasone to promote extubation in ventilated premature infants. Pediatric Pulmonology 2003;35:375-83.
Suchomski 2002 {published data only}
Suchomski SJ, Cummings JJ. A randomised trial of inhaled versus intravenous steroids in ventilator dependent preterm infants. Journal of Perinatology 2002;22:196-203.
References to excluded studies
Dimitriou 1997 {published data only}Dimitriou G, Greenhough A, Giffin FJ, Kavadia V. Inhaled versus systemic steroids in chronic oxygen dependency of preterm infants. European Journal of Pediatrics 1997;156:51-5.
Nicholl 2002 {published data only}
Nicholl RM, Greenough A, King M, Cheeseman P, Gamsu HR. Growth effects of systemic versus inhaled steroids in chronic lung disease. Archives of Disease in Childhood 2002;87:F59-F61.
* indicates the primary reference for the study
Other references
Additional references
Arnon 1992Arnon S, Grigg J, Nikander K, Silverman M. Delivery of micronised budesonide suspension by metered dose inhaler and jet nebuliser into a neonatal ventilator circuit. Pediatric Pulmonology 1992;13:172-5.
Avery 1985
Avery GB, Fletcher AB, Kaplan M, Brudno DS. Controlled trial of dexamethasone in respirator-dependent infants with bronchopulmonary dysplasia. Pediatrics 1985;75:106-11.
Bell 1978
Bell MJ, Ternberg JL, Feigin RD, Keating JP, Marshall R, Barton L, et al. Neonatal necrotising enterocolitis: Therapeutic decisions based upon clinical staging. Annals of Surgery 1978;187:1-7.
CDTG 1991
Collaborative Dexamethasone Trial Group. Dexamethasone therapy in neonatal chronic lung disease: an international placebo controlled trial. Pediatrics 1991;88:421-7.
CFN/AAP 2002
Committee on Fetus and Newborn: American Academy of Pediatrics. Postnatal corticosteroids to treat or prevent chronic lung disease in preterm infants. Pediatrics 2002;109:330-8.
Crowley 2002
Crowley P. Prophylactic corticosteroids for preterm delivery. Cochrane Database of Systematic Reviews 2002, Issue 3.
Cummings 1989
Cummings JJ, D'Eugenio DB, Gross SJ. A controlled trial of dexamethasone in preterm infants at high risk for bronchopulmonary dysplasia. New England Journal of Medicine 1989;320:1505-10.
FNC/CPS 2002
Fetus and Newborn Committee: Canadian Pediatric Society. Postnatal corticosteroids to treat or prevent chronic lung disease in preterm infants. Journal of Paediatrics and Child Health 2002;7:20-8.
Grigg 1992
Grigg J, Arnon S, Jones T, Clarke A, Silverman M. Delivery of therapeutic aerosols to intubated babies. Archives of Disease in Childhood 1992;67:25-30.
Halliday 1999
Halliday HL. Clinical trials of postnatal steroids: inhaled and systemic. Biology of the Neonate 1999;76:29-40.
Halliday 2001a
Halliday HL. Guidelines on neonatal steroids. Prenatal and Neonatal Medicine 2001;6:371-3.
Halliday 2002a
Halliday HL, Ehrenkranz RA. Delayed (>3 weeks) postnatal corticosteroids for chronic lung disease in preterm infants. Cochrane Database of Systematic Reviews 2002, Issue 3.
Halliday 2002b
Halliday HL, Ehrenkranz RA. Moderately early (7-14 days) postnatal steroids for preventing chronic lung disease in preterm infants. Cochrane Database of Systematic Reviews 2002, Issue 3.
Halliday 2002c
Halliday HL, Ehrenkranz RA. Early postnatal (< 96 hours) corticosteroids for preventing chronic lung disease in preterm infants. Cochrane Database of Systematic Reviews 2002, Issue 3.
Harkavy 1989
Harkavy KL, Scanlon JW, Chowdhry PK, Grylack LJ. Dexamethasone therapy for chronic lung disease in ventilator-and-oxygen- dependent infants: a controlled trial. Journal of Pediatrics 1989;115:979-83.
ICROP 1984
The Committee for the Classification of Retinopathy of Prematurity. An international classification of retinopathy of prematurity. Archives of Ophthalmology 1984;102:1130-4.
Johnson 1979
Johnson JW, Mitzner W, London WT, Palmer AE, Scott R. Betamethasone and the rhesus fetus: multisystemic effects. American Journal of Obstetrics and Gynecology 1979;133:677-84.
Kazzi 1990
Kazzi NJ, Brans YW, Poland RL. Dexamethasone effects on the hospital course of infants with bronchopulmonary dysplasia who are dependent on artificial ventilation. Pediatrics 1990;86:722-7.
LaForce 1993
LaForce WR, Brudno DS. Controlled trial of beclomethasone dipropionate by nebulization in oxygen-and-ventilator-dependent infants. Journal of Pediatrics 1993;122:285-8.
Lee 2000
Lee SK, McMillan DD, Ohlsson A, Pendray M, Synnes A, Whyte R, et al. Variations in practice and outcomes in the Canadian NICU Network: 1996-1997. Pediatrics 2000;106:1070-9.
Lemons 2001
Lemons JA, Bauer CR, Oh W, Korones SB, Papile LA, Stoll BJ, et al. Very low birth weight outcomes of National Institute of Child health and human development neonatal research network, January 1995 through December 1996. NICHD Neonatal Research Network. Pediatrics 2001;107:E1.
Ng 1993
Ng PC. The effectiveness and side effects of dexamethasone in preterm infants with bronchopulmonary dysplasia. Archives of Disease in Childhood 1993;68:330-6.
O'Callaghan 1992
O'Callaghan C, Hardy J, Stammers J, Stephensen T, Hull D. Evaluation of techniques for delivery of steroids to lungs of neonates using a rabbit model. Archives of Disease in Childhood 1992;67:20-4.
O'Shea 1999
O'Shea TM, Kothadia JM, Klinepeter KL, Goldstein DJ, Jackson BG, Weaver RG 3rd, et al. Randomized placebo-controlled trial of a 42 day tapering course of dexamethasone to reduce the duration of ventilatory dependency in very low birth weight infants: outcomes of study participants at 1-year adjusted age. Pediatrics 1999;104:15-21.
Ohlsson 1992
Ohlsson A, Calvert SA, Hosking M, Shennan AT. Randomized controlled trial of dexamethasone treatment in very-low-birth-weight infants with ventilatory dependent chronic lung disease. Acta Paediatrica 1992;81:751-6.
Papile 1978
Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 grams. Journal of Pediatrics 1978;92:529-34.
Saarela 1999
Saarela T, Vaarala A, Lanning P, Koivisto M. Incidence, ultrasonic patterns and resolution of nephrocalcinosis in very low birth-weight infants. Acta Paediatrica 1999;86:655-60.
Shah 2001
Shah V, Ohlsson A. Postnatal dexamethasone in the prevention of chronic lung disease. In: David TJ, editor(s). Recent Advances in Paediatrics. London, England: Churchill Livingstone, 2001:77-96.
Shah 2002
Shah V, Ohlsson A, Halliday HL, Dunn MS. Early administration of inhaled corticosteroids for preventing chronic lung disease in ventilated very low birth weight preterm neonates. Cochrane Database of Systematic Reviews 2002, Issue 3.
Shinwell 2000
Shinwell ES, Karplus M, Reich D, Weintraub Z, Blaazer S, Bader D, et al. Early postnatal dexamethasone treatment and increased incidence of cerebral palsy. Archives of Disease in Childhood Fetal Neonatal Edition 2000;83:F177- 81.
Sinkin 1990
Sinkin RA, Cox C, Phelps DL. Predicting risk for bronchopulmonary dysplasia: selection criteria for clinical trials. Pediatrics 1990;86:728-36.
Soll 2002
Soll RF. Synthetic surfactant for respiratory distress syndrome in preterm infants. Cochrane Database of Systematic Reviews 2002, Issue 3.
Stark 2001
Stark AR, Carlo WA, Tyson JE, Papile LA, Wright LL, Shankaran EF, et al. Adverse effects of early dexamethasone treatment in extremely-low-birth-weight infants. New England Journal of Medicine 2001;344:95-101.
Weichsel 1977
Weichsel ME. The therapeutic use of glucocorticoid hormones in the perinatal period: potential neurologic hazards. Annals of Neurology 1977;2:364-6.
Yeh 1998
Yeh TF, Lin YJ, Huang CC, Chen YJ, Lin CH, Lin HC, et al. Early dexamethasone therapy in preterm infants: a follow up study. Pediatrics 1998;101:E7.
Yost 2002
Yost CC, Soll RF. Early versus delayed selective surfactant treatment for neonatal respiratory distress syndrome. Cochrane Database of Systematic Reviews 2002, Issue 3.
Zubrow 1995
Zubrow A, Hulman S, Kushner H, Falkner B. Determinants of blood pressure in infants admitted to neonatal intensive care units: a prospective multicenter study. Journal of Perinatology 1995;15:470-9.
Comparisons and data
| Comparison or outcome |
Studies |
Participants |
Statistical method |
Effect size |
| 01 Inhaled vs. systemic steroids (Infants
randomized between 12-21 days of age) |
| 01 CLD at 36 weeks PMA |
2 |
139 |
RR (fixed), 95% CI |
1.02 [0.83, 1.25] |
| 02 CLD at 28 days of age |
1 |
78 |
RR (fixed), 95% CI |
0.97 [0.90, 1.05] |
| 03 Death by 36 weeks PMA |
1 |
78 |
RR (fixed), 95% CI |
2.69 [0.13, 54.15] |
| 04 Death by 28 days of age |
1 |
78 |
RR (fixed), 95% CI |
2.69 [0.13, 54.15] |
| 05 Death by or CLD at 36 weeks PMA |
1 |
78 |
RR (fixed), 95% CI |
0.94 [0.83, 1.05] |
| 06 Death by or CLD at 28 days of age |
1 |
78 |
RR (fixed), 95% CI |
Not estimable |
| 07 Need for ventilation amongst survivors at 36 weeks
PMA |
1 |
76 |
RR (fixed), 95% CI |
1.10 [0.30, 4.06] |
| 08 Duration of mechanical ventilation amongst survivors
(days) |
1 |
77 |
WMD (fixed), 95% CI |
-3.00 [-16.28, 10.28] |
| 09 Duration of supplemental oxygen amongst survivors (days) |
1 |
76 |
WMD (fixed), 95% CI |
-15.00 [-36.83, 6.83] |
| 10 Length of hospital stay amongst survivors (days) |
1 |
76 |
WMD (fixed), 95% CI |
-13.00 [-33.22, 7.22] |
| 11 Hyperglycemia |
2 |
139 |
RR (fixed), 95% CI |
0.33 [0.05, 2.12] |
| 12 Hypertension |
2 |
139 |
RR (fixed), 95% CI |
0.70 [0.31, 1.58] |
| 13 Necrotizing enterocolitis |
1 |
78 |
RR (fixed), 95% CI |
2.12 [0.25, 18.02] |
| 14 Gastrointestional bleed |
1 |
78 |
RR (fixed), 95% CI |
Not estimable |
| 15 Periventricular leucomalacia |
2 |
139 |
RR (fixed), 95% CI |
0.83 [0.33, 2.08] |
| 16 Retinopathy of prematurity > or equal to stage 3 |
2 |
139 |
RR (fixed), 95% CI |
1.33 [0.64, 2.74] |
| 17 Culture proven sepsis |
1 |
78 |
RR (fixed), 95% CI |
1.24 [0.35, 4.40] |
| 02 Inhaled vs. systemic steroids among all
randomized (Infants randomized at < 72 hrs of age) |
| 01 CLD at 36 weeks PMA |
1 |
292 |
RR (fixed), 95% CI |
1.10 [0.82, 1.47] |
| 02 CLD at 28 days of age |
1 |
292 |
RR (fixed), 95% CI |
1.06 [0.88, 1.26] |
| 03 Death by 36 weeks PMA |
1 |
292 |
RR (fixed), 95% CI |
0.96 [0.62, 1.49] |
| 04 Death by 28 days of age |
1 |
292 |
RR (fixed), 95% CI |
0.85 [0.52, 1.37] |
| 05 Death by or CLD at 36 weeks PMA |
1 |
292 |
RR (fixed), 95% CI |
1.04 [0.86, 1.26] |
| 06 Death by or CLD at 28 days of age |
1 |
292 |
RR (fixed), 95% CI |
1.00 [0.90, 1.12] |
| 07 Pneumothorax |
1 |
292 |
RR (fixed), 95% CI |
0.92 [0.53, 1.60] |
| 08 Other air leaks |
1 |
292 |
RR (fixed), 95% CI |
1.00 [0.55, 1.83] |
| 09 Pulmonary hemorrhage |
1 |
292 |
RR (fixed), 95% CI |
0.86 [0.43, 1.72] |
| 10 Duration of mechanical ventilation (days) |
1 |
292 |
WMD (fixed), 95% CI |
0.13 [-5.17, 5.43] |
| 11 Duration of supplemental oxygen (days) |
1 |
292 |
WMD (fixed), 95% CI |
6.72 [-16.70, 30.14] |
| 12 Hyperglycemia |
1 |
292 |
RR (fixed), 95% CI |
0.90 [0.63, 1.28] |
| 13 Hypertension |
1 |
292 |
RR (fixed), 95% CI |
0.87 [0.74, 1.02] |
| 14 Necrotizing enterocolitis |
1 |
292 |
RR (fixed), 95% CI |
0.86 [0.43, 1.72] |
| 15 Gastrointestinal bleed |
1 |
292 |
RR (fixed), 95% CI |
0.89 [0.41, 1.93] |
| 16 Gastrointestinal perforation |
1 |
292 |
RR (fixed), 95% CI |
0.85 [0.23, 3.08] |
| 17 Patent ductus arteriosus |
1 |
292 |
RR (fixed), 95% CI |
0.90 [0.73, 1.11] |
| 18 Retinopathy of prematurity, any stage |
1 |
292 |
RR (fixed), 95% CI |
1.27 [0.86, 1.89] |
| 19 Culture proven sepsis |
1 |
292 |
RR (fixed), 95% CI |
1.06 [0.78, 1.44] |
01 Inhaled vs. systemic steroids (Infants randomized between 12-21 days of age)
01.01 CLD at 36 weeks PMA
01.02 CLD at 28 days of age
01.03 Death by 36 weeks PMA
01.04 Death by 28 days of age
01.05 Death by or CLD at 36 weeks PMA
01.06 Death by or CLD at 28 days of age
01.07 Need for ventilation amongst survivors at
36 weeks PMA
01.08 Duration of mechanical ventilation amongst
survivors (days)
01.09 Duration of supplemental oxygen amongst
survivors (days)
01.10 Length of hospital stay amongst survivors
(days)
01.11 Hyperglycemia
01.12 Hypertension
01.13 Necrotizing enterocolitis
01.14 Gastrointestional bleed
01.15 Periventricular leucomalacia
01.16 Retinopathy of prematurity > or equal
to stage 3
01.17 Culture proven sepsis
02 Inhaled vs. systemic steroids among all randomized (Infants randomized at < 72 hrs of age)
02.01 CLD at 36 weeks PMA
02.02 CLD at 28 days of age
02.03 Death by 36 weeks PMA
02.04 Death by 28 days of age
02.05 Death by or CLD at 36 weeks PMA
02.06 Death by or CLD at 28 days of age
02.07 Pneumothorax
02.08 Other air leaks
02.09 Pulmonary hemorrhage
02.10 Duration of mechanical ventilation (days)
02.11 Duration of supplemental oxygen (days)
02.12 Hyperglycemia
02.13 Hypertension
02.14 Necrotizing enterocolitis
02.15 Gastrointestinal bleed
02.16 Gastrointestinal perforation
02.17 Patent ductus arteriosus
02.18 Retinopathy of prematurity, any stage
02.19 Culture proven sepsis
Contact details for co-reviewers
Prof Henry L Halliday
Consultant Neonatologist
Regional Neonatal Unit
Royal-Jubilee Maternity Service
Royal Maternity Hospital
Grosvenor Road
Belfast
Northern Ireland UK
BT12 6BA
Telephone 1: + 44 02890 894687
Facsimile: 02890 236203
E-mail: h.halliday@qub.ac.uk
Dr Arne Ohlsson
Director Evidence Based Neonatal Care and Outcomes Research
Department of Paediatrics
Mount Sinai Hospital
600 University Avenue
Toronto
Ontario CANADA
M5G 1X5
Telephone 1: +1 416 586 8379
Telephone 2: +1 416 341 0444
Facsimile: +1 416 586 8745
E-mail: aohlsson@mtsinai.on.ca
| This review is published as a Cochrane review in The Cochrane Library,
Issue 4, 2007 (see http://www.thecochrane.library.com for information).
Cochrane reviews are regularly updated as new evidence emerges and in response
to feedback. The Cochrane Library should be consulted for the most recent
version of the review. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}