No new trials were identified as a result of the most recent search completed March 5, 2004.
The previous conclusion of no significant difference in somatic growth of infants fed by continuous versus intermittent bolus tube feeds remains unchanged.
Theoretical risks and benefits of both continuous nasogastric milk feeding and intermittent bolus milk feeding have been proposed. Continuous nasogastric feedings may be more energy efficient by increasing energy absorbed and decreasing energy expenditure (Grant 1991), reduce feeding intolerance, improve nutrient absorption, and improve growth (Toce 1987). However, continuous infusion of milk into the gut could alter the cyclical pattern of release of gut hormones which might affect metabolic homeostasis, and growth (Aynsley-Green 1982). Furthermore, a properly functioning lower esophageal sphincter is an important barrier against the reflux of stomach contents into the esophagus and aspiration. Reflux and aspiration may be compounded in the premature infant receiving continuous nasogastric feedings. Not only do these infants have reduced lower esophageal sphincter pressure (Newell 1988), but the nasogastric tube remains in situ preventing complete closure of the sphincter.
Milk feedings given by the intermittent bolus gavage method are thought to be more physiologic because they promote the cyclical surges of gut hormones normally seen in healthy term infants (Aynsley-Green 1982; Aynsley-Green 1990). Gastrointestinal hormones such as gastrin, gastric inhibitory peptide, and enteroglucagon are trophic and require the presence of intraluminal nutrients to stimulate secretion. Surges in plasma concentrations of gut hormones postnatally may be important for gut development (Aynsley-Green 1989; Lucas 1986). On the other hand, functional limitations of the premature infant's gastrointestinal system such as delayed gastric emptying or intestinal transit could hinder the premature infant's ability to handle bolus milk feeds, resulting in feeding intolerance. Additionally, this feeding regimen alternates between periods of feeding and fasting which may challenge the premature infant's ability to maintain metabolic homeostasis and, therefore, decrease growth (Aynsley-Green 1982).
The effects of the feeding method on feeding tolerance, weight gain or days to regain birth weight were examined in two non-randomized controlled trials (Krishnan 1981; Urrutia 1983). In a retrospective study, Krishnan 1981 found that infants fed milk by continuous nasogastric tube feeding reached enteral intakes of 90 kcal/kg/day almost twice as quickly as those infants fed milk by intermittent bolus gavage feeding (16 +/- 6 vs 26 +/- 17 days, respectively). As well, infants in the continuous group achieved steady weight gain sooner than infants in the intermittent group (24 +/- 10 vs 32 +/- 14 days). Unfortunately, these findings are difficult to interpret due to study design and methodologic limitations. First, the non-random assignment of patients allows for selection bias. Second, energy intake was not controlled and may have influenced feeding tolerance and weight gain. Third, a convenience sample rather than a predetermined sample size was used, making it difficult to achieve both clinical and statistical significance in a study. Hence, it is difficult to make generalizations regarding these findings to similar populations of infants (Raudonis 1995).
Urrutia 1983 conducted a non-randomized
prospective study of continuous versus intermittent nasogastric tube milk
feedings. They found no difference between groups in days to regain birth
weight. These findings are also difficult to interpret because patients were
allocated to the continuous or intermittent group based on neonatologists'
preference rather than random assignment, and a convenience sample was used.
Clearly it is important to determine the clinical risks and benefits
of each method of feeding to enable clinicians to make informed decisions
regarding the most appropriate feeding method for an individual infant. Therefore,
a systematic review of trials which compare the two methods of milk feedings
was performed.
i) identifying all experimental and quasi-experimental trials of continuous versus intermittent nasogastric tube milk feeding in this population
ii) assessing the methodologic quality of each study
iii) examining the risks and benefits of continuous versus intermittent nasogastric tube milk feeding in preterm infants < 1500 grams on clinically relevant outcomes including:
Primary Outcomes:
a) feeding intolerance as measured by number of feeding interruptions and days on total parenteral nutrition (TPN)
b) days to regain birth weight
c) age at full enteral feedings
d) age at discharge to referral hospital or home
e) somatic growth including rates of gain in weight, length, and head circumference
f) necrotizing enterocolitis (NEC) including suspected and confirmed (Bell's Stage II or greater)
Secondary Outcomes:
a) Apnea
iv) doing subgroup analyses based on weight groups including <= 749 grams, 750 to 999 grams, and 1000 to < 1500 grams
Secondary Outcomes:
a) Apnea
All potentially relevant titles and abstracts identified in the searches, by either reviewer, were retrieved. The reference list of each article was reviewed independently for additional relevant titles and abstracts and these were also retrieved.
Methodologic quality was assessed using the following key criteria: blindness of randomization, blindness of intervention, completeness of follow-up and blinding of outcome measurement. Additional criteria of study quality included evidence of confounders, objective criteria of measuring outcomes, and defined exclusion/inclusion criteria. The interventions being compared could not be blinded to those providing care, but should have been blinded to the assessors of the outcomes.
Those articles judged to have the appropriate quality by both reviewers were included in the analysis. Data were extracted independently by the two reviewers. Posteriori subgroup analysis based on birth weight groups (< 1000 grams, 1000 -1249grams and 1250 - 1499 grams) was conducted where available, although these differed from the subgroups proposed a priori (< 750 g, 750 - 999 grams, 1000 - 1500 grams).
Weighted mean differences are reported for continuous outcomes such as days of feeding intolerance, and relative risk for categorical outcomes such as incidence of NEC. The comparisons have been displayed with 95% confidence intervals in Cochrane plots. Homogeneity of the estimates was tested.
Investigators were contacted for additional information and/or clarification regarding five studies (Dollberg 2000;, Macdonald 1992; Schanler 1999, Silvestre 1996, and Toce 1987). See characteristics of included studies for details. Individual group standard deviation for data on days to full feeds from Macdonald 1992 (reported pooled standard deviations), and subgroup data from Dollberg 2000; Schanler 1999; Toce 1987 were not available to include in this update.
Akintorin 1997 included clinically stable infants 700 to 1250 grams who were able to start feeding before day 10 of life. Continuous feeds (N=39) were delivered by an infusion pump while bolus feeds (N=41) were given every three hours over 15-30 minutes by gravity via an indwelling feeding tube. Feeding protocols were developed for each 50-100 gram weight category and strategies were identified for managing feeding intolerance. Infants were followed until they were tolerating full feeds, defined as 100 Kcal/kg/d of enteral feeds for at least 48 hours. In addition to the primary outcome of days to full feeds, the authors reported feeding intolerance (feeds withheld for > 12 hours), days to regain birth weight, and days to discharge weight of 2040 grams.
Dollberg 2000 included infants 500 to 1250 grams who were < 48 hours postnatal age. Feeds were initiated between day two and five as per feeding protocol which included guidelines to manage feeding intolerance (gastric residual volume (GRV) > 20% volume of feeds over previous 4 hours). Continuous feeds (N=10) were delivered by infusion pump. Infants 501-750 grams received intermittent bolus feeding every two hours while infants > 750 grams received feedings every three hours by gravity (N=13). The major outcome variable was "delay in reaching full feeds", defined as the difference between the expected time to reach full feeds as per feeding protocol and the actual time taken by infants to attain full feeds, defined as 160 cc/kg/d. Days to full feeds, and days to regain birth weight were also reported.
Macdonald 1992 (partial) included infants < 1400 grams whose route of feed was determined on day two of life when milk feedings were commenced. Infants were fed by bolus nasogastric (N=12), continuous nasogastric (N=12), or transpyloric (N=10) feeding method. Infants were supplemented with total parenteral nutrition. Although a feeding protocol was described, it appears to pertain to continuous feeding method as initial volume of feed and increments are described in mls/hour. The delivery equipment for continuous feeds, the bolus feeding method, transpyloric feeding method, and management of feeding intolerance was not described. The selected method of feeding was used until infants reached a weight of 1600 grams after which all infants were switched to bolus nasogastric feeding method. Energy supplements were not provided during the trial period. The primary outcome of this study was growth including length, weight, and occipitofrontal circumference. Standard deviations for days to full enteral feedings was not reported and we are awaiting response from the co-investigator of this study. Triceps and quadriceps skinfold thickness, and chosen biochemical indices (e.g., alkaline phosphatase, urea, albumin, prealbumin, and transferrin) were also measured but were not included in this review.
Schanler 1999 included infants 26 to 30 weeks gestation who were < 96 hours of age and whose fraction of inspired oxygen was < 0.6 by 72 hours. Feeding protocols were developed for feeding schedules and management of feeding intolerance. The continuous feeding method (N=83) was not described. Intermittent feedings (N=88) were given every three hours over 20 minutes. The primary outcome was days to attain full oral feeds, defined as eight bottle or breast feeds per day. Other outcomes reported in this study included days to full feeding (150 cc/kg/d), weight gain, head circumference gain, length gain, skinfold thickness (five sites), feeding intolerance, nutritional balance studies, bone mineral content and serum indices of protein and mineral status.
Silvestre 1996 (partial) included infants 750 to < 1500 grams who were able to start feeds on day two or three of life. Infants in the continuous feeding group (N=42) received a feeding over a three hour period. Infants in the intermittent bolus feeding group (N=40) were fed every three hours over 15-30 minutes up to a maximum of one hour if feeding difficulties were encountered. Feeding protocols were developed for advancement of feeds and for the management of feeding intolerance (GRV >= 2 hours feed volume for continuous; >= 2 mL feed for intermittent bolus). The primary outcome was rate of weight gain. Days to full feeds (75 kcal/kg/day) and days to discharge (criteria not defined) were also reported. Anthropometric measurements (change in head circumference, length, midtricipetal skin-fold thickness, skin-fold thickness, and subscapular skin-fold thickness) and retention rates of nitrogen, fat, total carbohydrate, and lactose were also compared between groups. There appears to be a significant difference between the continuous and intermittent feeding method groups in head circumference data, however, the difference is reported as being insignificant. Clarification has been requested.
Toce 1987 included infants < 1500 grams who were ready for enteral nutrition. The timing of feeds was not specified. Continuous feeds (N=30) were delivered by an infusion pump. Intermittent feeds (N=23) were given every three hours by gravity. Feeding protocols and management of feeding intolerance were standardized. The following outcomes were reported: somatic growth including weight gain, change in length, occipitofrontal circumference, and skin fold thickness, total protein, bilirubin, feeding related complications such as NEC, suspected NEC, feeding intolerance, hours NPO per day, number of apnea episodes per day, number of stools per day, and fraction heme-positive stools.
Caregivers were not blinded to the intervention as this would not be feasible. In one study (Silvestre 1996) outcome assessors were blinded, and in one study they were not (Dollberg 2000). For the remaining four studies, blinding of the outcome assessors could not be determined.
In each of the trials, several infants were removed from the assigned feeding protocols for clinical reasons, including but not limited to feeding intolerance. An intention-to-treat analysis should include outcome results for such infants. Only one study (Schanler 1999) had complete follow-up. In this study, infants were removed from the treatment protocol if they were not able to adhere to the feeding protocol for more than one week. Ten infants in the continuous group and one in the intermittent group were removed from their assigned feeding protocols because of feeding intolerance. However, data from these infants were included in the analysis. Silvestri 1996 reported complete follow-up only for stratified groups. In this study, 11 infants were removed from treatment protocols and excluded from overall analyses. Of three infants excluded from the continuous group, none were excluded for feeding intolerance although one was excluded for protocol violation. Of eight infants excluded from the intermittent group, three were excluded for feeding intolerance and another two for protocol violation. Follow-up was incomplete in the remaining three studies. Akintorin 1997 excluded nine infants from analysis. Of four patients excluded from the continuous group, one had been switched to breastfeeding, but none were excluded for feeding intolerance. Of five infants excluded from the intermittent group, three infants were excluded for protocol violation (feeding intolerance not specified) and one had been switched to breastfeeding. Dollberg 2000 excluded five infants from analysis, one for protocol violation (the infant was switched to bolus feeding method because of failure to establish full feedings) and the other four because of death. Macdonald 1992 enrolled 13 babies in the continuous feeding method group but only 12 completed the study as one infant was transferred to another hospital at age two weeks of life. Three of the 15 infants enrolled in the bolus feeding method group died within the first week of life, before milk feedings were established and were, therefore excluded from the analysis. In the Toce 1987 study, 30 infants were excluded because they did not complete seven days in the study. In these studies, the post-randomization exclusion of infants from the analysis has resulted in loss to follow-up.
The overall methodologic quality of the studies was fair. Refer to the table, Characteristics of Included Studies, for quality assessment.
01) Feeding performance
Days to full feeds (four trials). Dollberg 2000 and Schanler 1999 found that it took significantly longer for infants fed by the continuous feeding method to reach full feeds. However, Akintorin 1997 and Silvestre 1996 found no significant difference in the time taken to achieve full feeds. The meta-analysis revealed that it took infants significantly longer to reach full feeds when fed by the continuous tube feeding method (WMD 3.0 days; 95% CI 0.7, 5.2)
Days to full oral feeds (one trial). Schanler 1999 found no difference between groups.
Feeding intolerance (three trials). Schanler 1999 found no difference between groups in the number of days on which feedings were interrupted for feeding intolerance. Similarly, Toce 1987 found no difference between groups in the average number of hours spent NPO per day for feeding intolerance. Finally, Akintorin 1997 found no difference in the number of infants who experienced feeding intolerance, defined as feeds held longer than 12 hours. A meta-analysis could not be performed because the measures of feeding intolerance were not comparable.
Days on TPN (one trial). Schanler 1999 found no difference in the number of days on TPN for infants fed by either method.
02) Growth Outcomes
Days to regain birth weight (three trials). Akintorin 1997; Schanler 1999 and Silvestre 1996 found no difference in time to regain birth weight between the two feeding groups. The meta-analysis found no evidence of a difference between feeding methods (WMD -0.6 days; 95% CI -1.78, 0.6).
Weight gain (four trials). Two studies (Schanler 1999, and Toce 1987) reported weight gain in grams per kg per day while the other two studies (Macdonald 1992, and Silvestre 1996) reported weight gain in grams per week. Schanler 1999 found that infants fed by the continuous feeding method gained weight slower than infants fed by the intermittent bolus feeding method. However, Toce 1987 did not find a difference in weight gain between the two groups. The meta-analysis did not support a difference in growth rates between the two groups (WMD -1.1 g per kg per day; 95% CI -2.3, 0.03). Similarly, Macdonald 1992 and Silvestre 1996 did not find a difference in weight gain (grams per week) between the two groups. The meta-analysis once again did not support a difference in growth rates between the two groups (WMD 6.27 g/week 95% CI -1.28, 13.8).
Length gain (four trials). None of the trials showed a difference in length gain between the two groups (Macdonald 1992; Schanler 1999; Silvestre 1996; Toce 1987). The meta-analysis of the four trials (Macdonald 1992; Schanler 1999; Silvestre 1996; Toce 1987) that reported length gain found there was no evidence of a difference in length gain between the two groups (WMD 0.08 cm/week; 95% CI -0.01, 0.17).
Head circumference gain (four trials). Macdonald 1992; Schanler 1999 and Toce 1987 did not find any difference between groups, and the meta-analysis did not support a difference (WMD -0.03 cm/week; 95% CI -0.09, 0.04). Data from Silvestre 1996 have been excluded from the meta-analysis until clarified by the author (see Characteristics of Included Studies).
Change in triceps skinfold thickness (three trials). No difference in skinfold thickness was seen between groups in trials by Silvestre 1996 and Toce 1987 (WMD 0 mm/week; 95% CI -0.1, 0.1). Macdonald 1992 found marked interobserver variability in measurements of skinfold thickness and concluded that this was not a reliable method of assessing growth in low birth weight infants. The findings were not reported.
03) Utilization of Resources
Days to discharge (two trials). Schanler 1999 and Silvestre 1996 were unable to find any difference between groups in time to discharge. The meta-analysis supports this conclusion (WMD -1.94 days; 95% CI -8.3, 4.4).
Days to discharge weight of 2040 grams (one trial). Akintorin 1997 did not find any difference between groups.
Days on mechanical ventilation (one trial). Akintorin 1997 found that infants were ventilated for similar lengths of time regardless of the method of feeding.
04) Complications (categorical)
Proven necrotizing enterocolitis (NEC), Bell's stage II or greater (5 trials). In the trials by Akintorin 1997; Schanler 1999 and Toce 1987 there were no differences between groups in the incidence of proven NEC. Silvestre 1996 had no cases of NEC in study infants. In the meta-analysis of these four studies, there was no evidence of effect (RR 0.96; 95% CI 0.49, 1.90). Macdonald 1992 reported cases of proven and suspected NEC determined solely on radiographic findings which were not described. Hence, the data were not included in the meta-analysis. There was one case of proven NEC and one case of probable NEC in the continuous group. Infants in the bolus group had no cases of NEC, proven or probable.
Probable NEC (two trials). Neither Toce 1987 nor Akintorin 1997 found any difference between groups in the incidence of probable NEC.
Failure to complete protocol because of feeding intolerance (two trials). Schanler 1999 and Silvestre 1996 reported the number of infants who were unable to complete the feeding protocol due to feeding intolerance. Schanler 1999 found that infants allocated to continuous feeds were significantly more likely to be withdrawn from the assigned feeding protocol. The meta-analysis found no evidence of a difference between groups in infants removed from the assigned feeding protocol due to feeding intolerance (RR 2.5; 95% CI 0.8, 7.4). However, it is difficult to draw a conclusion from these data because there was significant statistical heterogeneity suggesting the two studies may have assessed this outcome differently.
05) Complications (continuous)
Apnea (two trials). Toce 1987 did not find a significant difference in the number of apneas per infant per day between groups. Schanler 1999 did show a trend toward increased number of apneic episodes during the study period in infants fed by continuous feeding method (MD 14.0 apneas; 95% CI -0.2, 28.2). A meta-analysis could not be performed as the two studies reported episodes differently. The results of Schanler 1999 are in contrast to observations of Akintorin 1997 in which apnea was more commonly observed in the intermittent feeding group (data not provided). Similarly, Silvestre 1996 reported that only infants in the intermittent feeding group (750-999 gram weight category) had feedings held for recurrent apnea.
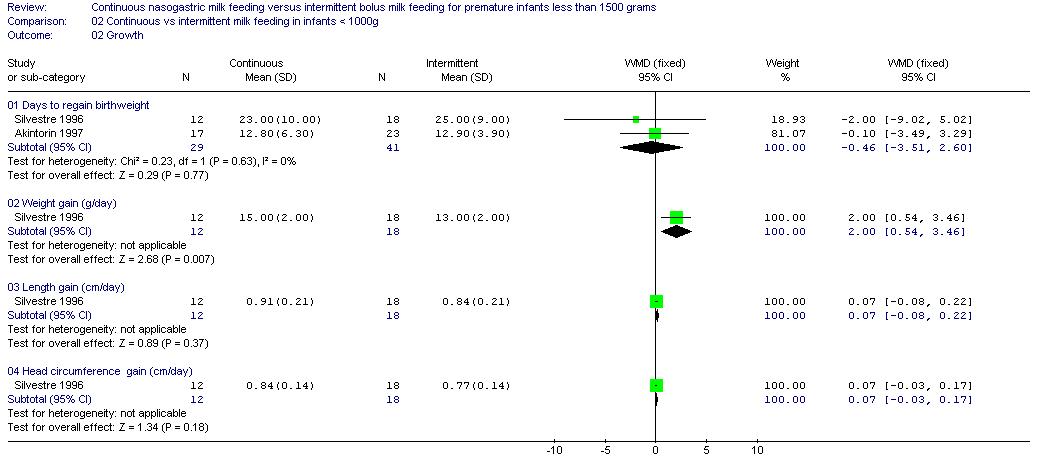
2) CONTINUOUS VERSUS INTERMITTENT BOLUS MILK FEEDING - INFANTS < 1000 GRAMS
01) Feeding Performance
Days to full feeds (two trials). Trials by Akintorin 1997 and Silvestre 1996 did not find a difference in days to full feeds between groups. The meta-analysis also found no difference between groups (WMD 0.8 days; 95% CI -2.8, 4.3).
02) Growth Outcomes
Days to regain birthweight (two trials). Akintorin 1997 and Silvestre 1996 did not show a difference between groups. The meta-analysis did not show a difference between groups (WMD -0.5 days; 95% CI -3.5, 2.6).
Weight gain (one trial). Data from Silvestre 1996 suggested that infants < 1000 grams birth weight gained weight faster when fed by continuous tube feeding method (mean difference 2.0 g/day; 95% CI 0.5, 3.5).
Length gain (one trial). Silvestre 1996 found no difference between groups.
Head circumference gain (one trial). Silvestre 1996 found no difference between groups.
03) Utilization of Resources
Days to discharge (one trial). Data from Silvestre 1996 suggested a trend toward earlier discharge in infants with birth weight less than 1000 grams fed by continuous tube feeding method (mean difference -11 days; 95% CI -21.8, -0.2).
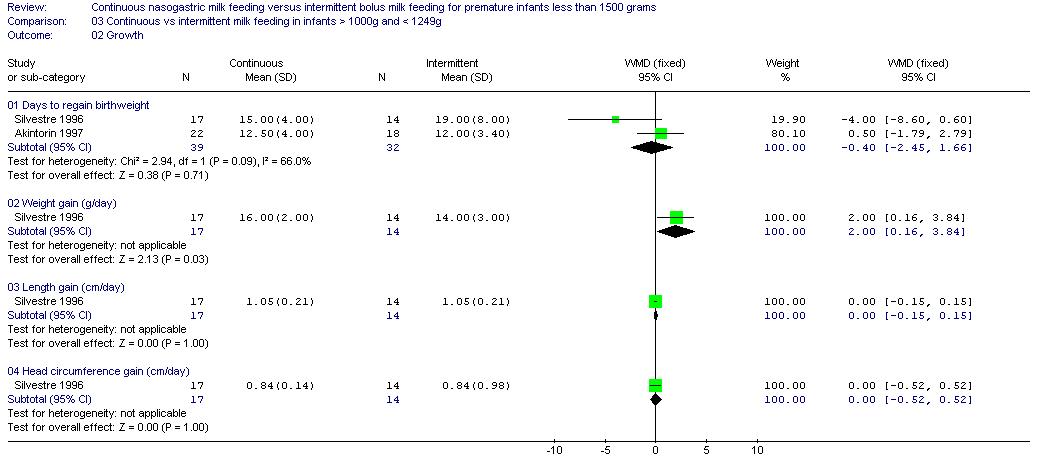
3) CONTINUOUS VERSUS INTERMITTENT BOLUS MILK FEEDING - INFANTS 1000 - 1249 GRAMS
01) Feeding Performance
Days to full feeds (two trials). Neither Akintorin 1997 nor Silvestre 1996 found a difference between groups. The meta-analysis also found no difference (WMD -0.2 days; 95% CI 2.5, 2.2).
02) Growth Outcomes
Days to regain birthweight (two trials). Neither Akintorin 1997 nor Silvestre 1996 found a difference in days to regain birthweight between infants fed by continuous or intermittent tube feeding method. The meta-analysis also showed no evidence of a difference (WMD -0.4 days; 95% CI -2.5, 1.7).
Weight gain (one trial). Data from Silvestre 1996 suggested that infants with birth weight 1000 - 1249 grams gained weight faster when fed by continuous tube feeding method (mean difference 2.0 grams/day; 95% CI 0.2, 3.8).
Length gain (one trial). Silvestre 1996 found no difference in length gain between groups.
Head circumference gain (one trial). Silvestre 1996 found no difference in head circumference gain between groups.
03) Utilization of Resources
Days to discharge (one trial). Silvestre 1996 found no difference in days to discharge for infants fed by continuous versus intermittent tube feeding methods.
Days to discharge weight of 2040 grams (one trial). Akintorin 1997 found no difference between groups in days to reach discharge weight.
4) CONTINUOUS VERSUS INTERMITTENT BOLUS MILK FEEDING - INFANTS 1250 - 1499 GRAMS
01) Feeding Performance
Days to full feeds (one trial). Silvestre 1996 found no difference between groups in days to full feeds.
02) Growth Outcomes
Days to regain birthweight (one trial). Silvestre 1996 found no difference between groups in the days to regain birthweight.
Weight gain (one trial). Silvestre 1996 found no difference between groups.
Length gain (one trial). Silvestre 1996 found no difference between groups.
Head circumference gain (one trial). Silvestre 1996 found no difference between groups.
03) Utilization of Resources
Days to discharge (one trial). Silvestre 1996 found no difference between groups.
Five studies (Akintorin 1997; Dollberg 2000; Schanler 1999; Silvestre 1996; Toce 1987) compared continuous infusion with intermittent feeds given every two or three hours. One study (Macdonald 1992) compared continuous infusion, intermittent feeds (frequency unknown), and transpyloric method of feeding. All but one study (Macdonald 1992) stratified participants, either by birth weight or gestational age, in order to obtain more homogeneous samples for comparison. Overall, the evidence suggests that infants fed by the continuous tube feeding method took longer to reach full feeds. However, there was no difference in growth (weight, length, head circumference) of infants fed by either method. Although infants with birth weight < 1000 grams and 1000 - 1249 grams had better weight gain on continuous feeds, these results were only reported in one study with a small sample size. To assess this further, subgroup data has been requested from Dollberg 2000; Schanler 1999; Toce 1987. The lack of an effect on growth may, in part, be attributed to the consistent provision of nutrients within studies with the use of parenteral nutrition (Akintorin 1997; Macdonald 1992; Schanler 1999; Toce 1987). There was a trend toward increased number of apneas per patient in infants fed by the continuous tube feeding method (p=0.05), but this trend is in contrast to results observed in other studies. Finally, there was a trend toward earlier discharge in infants < 1000 grams birth weight fed by the continuous tube feeding method (p=0.05), but this trend was seen only in one study, again with a small sample size. Overall, there was no difference in days to discharge between groups.
These results should be interpreted with caution. While statistically and clinically significant, the finding that infants fed by continuous tube feeding method took longer to reach full feeds may be confounded by the definition and management of feeding intolerance. For example, five studies (Akintorin 1997; Dollberg 2000; Schanler 1999; Silvestre 1996; Toce 1987) had predetermined criteria to advance feeds and to identify and manage feeding intolerance. Gastric residual volume was a major criterion in determining feeding tolerance. Three of the studies (Akintorin 1997; Dollberg 2000; Schanler 1999) reported a greater incidence of residuals in infants fed by continuous tube feeding, and this may have resulted in a greater number of interruptions of feeds and / or slower increases in feeds, thereby increasing the number of days taken to reach full feeds. Dollberg 2000 reported that regression analysis suggested that only the method of feeding affected feeding intolerance defined as presence of residual > 20 % of the feed volume. In this study, continuous feeding was associated with increased feeding intolerance. Schanler 1999 reported an association between the greater number of residuals in the continuous group and increased time to full feeds. Akintorin 1997 similarly reported that there was an association between feeding intolerance and time to full feeds and time to reach discharge weight. On the other hand, Silvestre 1996 found that only infants in the intermittent group were removed from the study protocol for feeding-related reasons, including significant residuals. Depending on the individual tolerance for and response to gastric residuals, the management of feeding intolerance may significantly affect the reported feeding tolerance and the time taken to reach full feeds. The need for an evidence based approach to management of gastric residual volumes is apparent. Furthermore, only one study (Schanler 1999) included all infants in the results whether or not they were able to adhere to the feeding protocol. Silvestre 1996 included all infants in the analysis for subgroup analysis but not for overall analysis. Unfortunately, there were several infants in each study who were removed from the treatment protocol for various reasons including feeding intolerance and protocol violation. Exclusion of these infants might influence study outcomes such as days to full feeds.
There was statistical heterogeneity in the outcomes of weight gain and the number of infants who failed to complete the protocol because of feeding intolerance. Potential sources of heterogeneity might include differences in participants, intervention, and study quality.
Participants
In five studies (Akintorin 1997; Dollberg 2000; Schanler 1999; Silvestre 1996; Toce 1987)
infants were stratified into groups, either by birth weight or gestational
age prior to randomization because the feeding method may influence outcomes
differently across different weight groups. However, stratification varied
between these studies (see Characteristics of Included Studies).
Intervention
Although feeding protocols had been predetermined for all studies, both
the timing of initiation of feeds and the type of feeding varied between
studies. In two studies (Dollberg 2000; Silvestre 1996),
it is not clear when feeds were initiated, or if they were initiated at the
same postnatal age for all infants. Although one study (Macdonald 1992)
states on day 2 of life milk route was determined and milk feedings initiated,
it is unclear if all study infants were able to start feeds on day 2. In
the study by Schanler 1999, infants within
each feeding group were randomized to early or late feedings to be initiated
on postnatal day 4 or 14 respectively (actual initiation day 6 and 16 respectively).
The number of infants who started feeds early versus late was similar between
the two groups. Akintorin 1997 reported similar timing of feeds for infants in the two groups (intermittent 5.6 +/- 2.2 days; continuous 5.7 +/- 2.1 days). Toce 1987
initiated feeds later (intermittent 7.3 +/- 4.8 days; continuous 9.7 +/-
7.1 days), but the difference between groups was not significant. The type
of feeding might also influence feeding tolerance and advancement to full
enteral feeds. Three studies (Akintorin 1997; Macdonald 1992; Silvestre 1996) excluded infants fed human milk. The other three studies (Dollberg 2000; Schanler 1999; Toce 1987) included infants fed either human milk or infant formula. In the studies by Dollberg 2000 and Toce 1987, there were more infants fed human milk in the intermittent bolus group as compared with the continuous group (Dollberg 2000 4 vs 2 respectively, and Toce 1987
5 vs 0 respectively). Both the timing and the type of feedings might influence
outcomes such as days to reach full feeds, feeding intolerance and somatic
growth.
Study quality
Only three studies (Akintorin 1997; Schanler 1999; Silvestre 1996)
reported use of a power calculation to determine sample size. The primary
outcome used to determine the sample size differed in each of the three studies
and included days to full feeds, days to full oral feeds, and rate of weight
gain. This systematic review includes 459 infants. The mean and standard
deviation for days to full feeds from the largest study, Schanler 1999,
was used to determine the sample size required to show a significant difference
between Continuous and Intermittent bolus milk feeding. Based on a 2-tailed
unpaired t-test, alpha level of 0.05 and power of 0.8, the sample size was
estimated at 400 per group.
Only two studies included infants dropped from the feeding protocols in the analyses. Schanler 1999 included all infants in the analysis. Silvestre 1996 included all infants in the analyses of stratified groups, but excluded the infants dropped from the feeding protocols from the overall analysis. In each of the six studies included in this review, several infants were dropped from the treatment groups for various reasons, including feeding intolerance, protocol violations, and transfer to another hospital at 2 weeks of life. Exclusion of these infants who were unable to feed according to the assigned protocol might have impacted on outcomes including feeding tolerance, days to full feeds and days to discharge, as well as incidence of NEC and apnea.
Caregivers were not blinded to the intervention as this would not be feasible. This may have introduced bias in decisions related to feeding management of infants.
Finally, although all studies attempted to compare demographic data and various indices of acuity between groups, the health state of the infant might affect some of the outcomes of interest. For example, smaller, sicker infants may take longer to reach full feeds, and be discharged later. Akintorin 1997 reported that infants with feeding intolerance were more likely to weigh less than 1000 grams and to require ventilatory support for a longer period of time. In that study, 20 of 28 infants with feeding intolerance were < 1000 grams birth weight.
| Study | Methods | Participants | Interventions | Outcomes | Notes | Allocation concealment |
| Akintorin 1997 | Randomized. Stratified: Blindness of randomization - Yes. | 89 infants randomized. 9 post-randomization exclusions. 80 infants analyzed. Inclusion: Infants 700-1250g, hemodynamically stable and ready to start enteral feeds. Exclusion: Apgar score < 3 at 5 minutes, to receive breast milk, documented sepsis, NEC or unable to start feeding before day 10 of life. | Feeding did not begin until umbilical arterial catheter removed. Continuous feeding by infusion pump. Intermittent feeding given every 3 hours for 15-30 minutes by gravity via indwelling feeding tube. Feeding protocol for each 50-100 g weight category. Protocol to manage feeding intolerance (feeds held > 12 hours). Energy and protein intake kept identical between groups. Feeds: undiluted preterm formula (20 Kcal/oz). Timing of Feeds: | Primary: Days to full feeds (100 Kcal/kg/d). Secondary: Feeding intolerance, days to regain birth weight, days to discharge weight of 2040 g, NEC, and apnea (>15 seconds). | Sample size calculation based on 35% decrease in number of days to full feeds in continuous group. Did not exclude SGA infants. Uncertain when feeds changed from continuous to bolus feeding. Numbers unbalanced. Exclusions: 4 Continuous (none due to protocol violation) and 5 Bolus (3 due to protocol violation). Larger proportion of infants whose feeds were held in the continuous group had residuals, whereas in the bolus group infants had apnea/bradycardia. Guidelines for residuals may allow larger volumes than some other studies. | A |
| Dollberg 2000 | Randomized. Stratified: Blindness of randomization - Yes. | 28 infants randomized. 5 post-randomization exclusions. 23 infants analyzed. Inclusion: AGA, < 48 hours postnatal age, no major congenital malformations, and informed consent. | Continuous feeding by syringe pump. Intermittent feeding by gravity every 2 hours in 501 - 750g group; every 3 hours in other infants. Feeding protocol for each weight group. Protocol to manage feeding intolerance (gastric residual > 20% of the volume fed over the previous 4 hr). Feeds: undiluted human milk, preterm formula, (initially diluted), or both. Timing of Feeds: | Days to full feeds (160 mL/kg/day). Days to regain birth weight. Delay between expected time to full feeds vs actual time to full feeds. | Pilot study. Additional data re: intervention, sample size and methodologic criteria provided by investigator as study initially available as abstract (now published). No sample size calculation. 5 post-randomization exclusions. Regression analysis suggested mode of feeding as the only variable affecting feeding tolerance. Awaiting subgroup data. | A |
| Macdonald 1992 | Randomized. No Stratification. Blindness of randomization - Yes. Blindness of intervention - No. Complete follow-up - No. Blinding of outcome measurement - Can't tell. | 43 infants randomized. 9 post-randomization exclusions. 34 infants analyzed. Inclusion: Infants < 1400 g. | Milk
feeding started on day 2 of life with 1 mL/hr of SMA low birthweight formula
(Wyeth). Increased 0.5 to 1.0 mL/hr until tolerating 150 mL/kg/day (supplemented
with total parenteral nutrition). Unclear frequency of bolus feeding, frequency
of increase in feeds, equipment for delivery of continuous feeds. Selected method used until infant attained weight of 1600 g. No energy supplements during study period. | Growth
rate including weight gain (grams/week), length gain (mm/week), and occipitofrontal
circumference (mm/week), and triceps and quadriceps skinfold thickness, oral
energy input, days to full feedings, and chosen biochemical indices (e.g.,
alkaline phosphatase, urea, albumin, prealbumin, and transferrin). Complications: extra abdominal radiographs, proved aspiration, NEC (proved and probable - ?used Bell's staging), septicemia, gastric bleeding. | No sample size calculation. Did not exclude SGA infants. Feeding intervention not described in detail. 5 exclusions in transpyloric group, 1 in continuous group and 3 in bolus group. Report pooled standard deviations for days to full feedings (awaiting mean and standard deviation). Extra
abdominal radiographs (n=31) were performed for transpyloric tube placements.
Aspiration (1 in continuous group) occured when babies were over 1600 grams,
hence were being fed by bolus nasogastric route. Gastric bleeding ( 1 in
bolus group) occurred before milk feedings were started. Staphylococcus
epidermidis - 1 case in each group - unclear if this was during study period
or during length of stay in NICU. | A |
| Schanler 1999 | Randomized. (balanced 2 way design). Stratified: Diet: human milk and formula. Blindness of randomization - yes. | 171 infants randomized. Inclusion: 26 to 30 weeks gestation, AGA, postnatal age < or = 96 hours, no congenital anomalies, fraction of inspired oxygen < 0.6 by 72 hours, and written informed consent. Removed infants from treatment protocol if unable to adhere to feeding protocol for > 1 week. | GI
priming vs no enteral intake day 4 to 14 and continuous vs bolus nasogastric
tube feedings. 4 Groups: NPO continuous, NPO bolus, GI priming continuous,
and GI prime bolus. Bolus feeding given every 3 hours over 20 minutes. Continuous
feeding method not described. Feeding protocol for infants. Protocol to
manage feeding intolerance based on excess gastric residual volume. Nutrient
intakes similar between groups. Feeds: undiluted human milk or initially
diluted preterm infant formula. Timing of Feeds: Protocol was 4 - 14 days. Actual was 6 - 16 days. | Primary: time to full oral feeding (8 breast/bottle feeding per day). Secondary: days to full enteral feeding (150cc/kg/d), weight gain, head circumference gain, length gain, skinfold thickness (5 sites), feeding intolerance, NEC, apnea (>20 seconds), nutritional balance studies, bone mineral content and serum indices of protein and mineral status. | Data comparing continuous vs intermittent groups obtained from investigator. Intent-to-treat analysis. Sample size calculation based on a 2 week difference in the time to full oral feeds. Infants randomized to early vs late enteral feeds (day 4 vs 14). Small sample size given the number of effects being examined (NPO, early feeding, and stratification of gestation age and feed type). Have established criteria for transition to oral feeds, however, not well described, some criteria subjective (e.g. favorable oral motor assessment, increased apnea, or oxygen needs). Awaiting subgroup data. | A |
| Silvestre 1996 | Randomized. Stratified: | 93 infants randomized. 11 post randomization exclusions.
82 infants analyzed (all 93 infants included in analysis of stratified groups).
Inclusion: Infants AGA with birth weight 750-1500 grams, born between 27-34 weeks gestation, had no major congenital malformations and stable to start feeds on day 2 or 3 of life. | Continuous feeds administered
over 3 hours, every 3 hours. Intermittent bolus feeds every 3 hours over
15-30 minutes. Feeding protocol for infants. Criteria to define feeding intolerance
predetermined (gastric residual volume >= 2 hr feed for continuous or
>= 2mL bolus feeds). Feeds: water, initially diluted preterm infant formula. Timing of Feeds: Protocol was day 2-3. Actual was not stated. | Primary: rate of weight gain. (*growth data was converted to grams/week). Secondary: days to full feeds, days to regain birth weight, days to discharge, length gain, and head circumference gain. | Clarification
of data for head circumference requested (data printed in the article appears
to be significant but was reported as insignificant - ? typographical error
in data). Data on complete study sample not "intent-to-treat". Intent-to-treat anlysis by weight groups. Sample size calculation based on >/= 10% increase rate of weight gain in continuous group. Full feeds not defined. 11 exclusions: ?criteria for discharge. Initial feed of water given for different duration (2 hours in continuous group vs 6 hours in bolus group). Nipple feeding 34 wks or 1500 grams. | A |
| Toce 1987 | Quasi-experimental. Alternate assignment within 16 groups. Stratified: <1250g, 1250-1500g, sex, IUGR, and prior need for ventilation. Blindness of randomization - Can't tell. | 83 infants (obtained consent). 30 excluded (completed less than 7 days). 53 analyzed. Inclusion: | Continuous
feeds delivered by infusion pump. Intermittent feeds every 3 hours by gravity.
Feeding protocol for infants. Predetermined criteria to manage feeding intolerance
(feeds held > 16 hours). Energy intake constant between groups. Feeds:
sterile water, initially diluted formula. Timing of Feeds: Protocol was not stated. Actual for Continuous group was 9.7 +/- 7.1 days and for Intermittent group was 7.3 +/- 4.8 days. | Somatic growth (weight, length, head circumference, and skinfold thickness gains), feeding related complications, changes in total protein, bilirubin, and albumin. | Subjective eligibility criteria, no sample size calculation, and not intent-to-treat. Definition of feeding intolerance not described. Significant differences in demographic factors between groups: low one-minute Apgar scores in the Continous group, and increase frequency of human milk feeding in the Intermittent bolus gavage feeding method. Awaiting subgroup data. | C |
| Study | Reason for exclusion |
| Baker 1997 | Outcomes not clinically relevant to this review - duodenal motor responses. |
| Berseth 1992 | Population unknown (i.e. weight). Outcomes not clinically relevant to this review - intestinal motor activity. |
Akintorin SM, Kamat M, Pildes RS, Kling P, Andes S, Hill J, Pyati S. A propective randomized trial of feeding methods in very low birth weight infants. Pediatrics 1997 Oct;100:E4.
Dollberg 2000 {published and unpublished data}
Dollberg S, Kuint J, Mazkereth R, et al. Feeding tolerance in preterm infants: Randomized trial of bolus and continuous feeding. Journal of the American College of Nutrition 2000;19(6):797-800.
Macdonald 1992 {published and unpublished data}
Macdonald PD, Skeoch CH, Carse H, Dryburgh F, Alroomi LG, Galea P, Gettinby G. Randomised trial of continuous nasogastric, bolus nasogastric, and transpyloric feeding in infants of birth weight under 1400 g. Archives of Disease in Childhood 1992;67:429-31.
Schanler 1999 {published and unpublished data}
* Schanler RJ, Shulman RJ, Lau C, Smith EO, Heitkemper MM. Feeding strategies for premature infants: Randomized trial of gastrointestinal priming and tube-feeding method. Pediatrics 1999;103(2):434-9.
Schanler RJ, Shulman RJ, Lau C. Feeding strategies for premature infants: Beneficial outcomes of feeding fortified milk versus preterm formula. Pediatrics 1999;103:1150-7.
Shulman RJ, Schanler RJ, Lau C, Heitkemper M, Ou CN, Smith EO. Early feeding, antenatal glucocorticoids, and human milk decrease intestinal permeability in preterm infants. Pediatric Research 1998;44:519-23.
Silvestre 1996 {published data only}
Silvestre MA, Morbach CA, Brans YW, Shankaran S. A prospective randomized trial comparing continuous versus intermittent feeding method in very low birth weight neonates. Journal of Pediatrics 1996;128:748-52.
Toce 1987 {published data only}
Toce SS, Keenan WJ, Homan SM. Enteral feeding in very-low-birth-weight infants. A comparison of two nasogastric methods. American Journal of Diseases of Children 1987;141:439-44.
Baker JH, Berseth CL. Duodenal motor responses in preterm infants fed formula with varying concentrations and rates of infusion. Pediatric Research 1997;42:618-22.
Berseth 1992 {published data only}
Berseth CL, Baker J, DeVille K, et al. Rate of feeding and nutrient concentration affect preterm small intestinal motor responses to orogastric feedings. Gastroenterology 1992;103:1385(Abstract).
* indicates the primary reference for the study
Aynsley-Green A, Adrian TE, Bloom SR. Feeding and the development of enteroinsular hormone secretion in the preterm infant: Effects of continuous gastric infusions of human milk compared with intermittent boluses. Acta Paediatrica Scandinavica 1982;71:379-83.
Aynsley-Green A. New insights into the nutritional management of newborn infants derived from studies of metabolic and endocrine inter-relations during the adaptation of postnatal life. The Proceedings of the Nutrition Society 1989;48:283-92.
Aynsley-Green A, Lucas A, Lawson GR, Bloom SR. Gut hormones and regulatory peptides in relation to enteral feeding, gastroenteritis, and necrotizing enterocolitis in infancy. Journal of Pediatrics 1990;117:S24-32.
Grant J, Denne SC. Effect of intermittent versus continuous enteral feeding on energy expenditure in premature infants. Journal of Pediatrics 1991;118:928-32.
Krishnan V, Satish M.. Continuous (C) vs. intermittent (I) nasogastric (N/G) feeding in very low birth weight (VLBW) infants. Pediatric Research 1981;15:537 (Abstract).
Lucas A, Bloom SR, Aynsley-Green A. Gut hormones and "minimal enteral feeding". Acta Paediatrica Scandinavica 1986;75:719-23.
Newell SJ, Sarkar PK, Durbin GM, Booth IW, McNeish AS. Maturation of the lower esophageal sphincter in the preterm baby. Gut 1988;29:167-72.
Raudonis BM, Talbot LA. Use of critical thinking in research: The research critique. In: Talbot LA, editor(s). Principles and practice of nursing research. St. Louis: Mosby:513-534.
Urrutia J, Poole E. Continuous nasogastric versus intermittent gavage feedings in very low birth weight infants. Pediatric Research 1983;17:203A (Abstract).
Valman HB, Heath CD, Brown RJK. Continuous intragastric milk feeds in infants of low birth weight. BMJ 1972;3:547-50.
Premji S, Chessell L. Continuous nasogastric milk feeding versus intermittent bolus milk feeding for premature infants less than 1500 grams (Cochrane Review). In: The Cochrane Library, Issue 1, 2001. Oxford: Update Software.
Premji S, Chessell L. Continuous nasogastric milk feeding versus intermittent bolus milk feeding for premature infants less than 1500 grams (Cochrane Review). In: The Cochrane Library, Issue 1, 2003. Oxford: Update Software.
01.01 Feeding performance
01.02 Growth
01.03 Utilization of resources
01.04 Complications (categorical)
01.05 Complications (continuous)
02 Continuous vs intermittent milk feeding in infants < 1000g
02.01 Feeding performance
02.02 Growth
02.03 Utilization of resources
03 Continuous vs intermittent milk feeding in infants > 1000g and < 1249g
03.01 Feeding performance
03.02 Growth
03.03 Utilization of resources
04 Continuous vs intermittent milk feeding in infants > 1250g and < 1499g
04.01 Feeding performance
04.02 Growth
04.03 Utilization of resources
| Comparison or outcome | Studies | Participants | Statistical method | Effect size |
|---|---|---|---|---|
| 01 Continuous vs intermittent milk feeding - all infants | ||||
| 01 Feeding performance | WMD (fixed), 95% CI | Subtotals only | ||
| 02 Growth | WMD (fixed), 95% CI | Subtotals only | ||
| 03 Utilization of resources | WMD (fixed), 95% CI | Subtotals only | ||
| 04 Complications (categorical) | RR (fixed), 95% CI | Subtotals only | ||
| 05 Complications (continuous) | WMD (fixed), 95% CI | Subtotals only | ||
| 02 Continuous vs intermittent milk feeding in infants < 1000g | ||||
| 01 Feeding performance | WMD (fixed), 95% CI | Subtotals only | ||
| 02 Growth | WMD (fixed), 95% CI | Subtotals only | ||
| 03 Utilization of resources | 2 | 70 | WMD (fixed), 95% CI | -2.48 [-7.63, 2.66] |
| 03 Continuous vs intermittent milk feeding in infants > 1000g and < 1249g | ||||
| 01 Feeding performance | WMD (fixed), 95% CI | Subtotals only | ||
| 02 Growth | WMD (fixed), 95% CI | Subtotals only | ||
| 03 Utilization of resources | WMD (fixed), 95% CI | Subtotals only | ||
| 04 Continuous vs intermittent milk feeding in infants > 1250g and < 1499g | ||||
| 01 Feeding performance | WMD (fixed), 95% CI | Subtotals only | ||
| 02 Growth | WMD (fixed), 95% CI | Subtotals only | ||
| 03 Utilization of resources | WMD (fixed), 95% CI | Subtotals only | ||
| This review is published as a Cochrane review in The
Cochrane Library 2004, Issue 3, 2004 (see www.CochraneLibrary.net for information).
Cochrane reviews are regularly updated as new evidence emerges and in response
to comments and criticisms, and The Cochrane Library should be consulted
for the most recent version of the Review. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}