Prophylactic systemic antifungal agents to prevent mortality
and morbidity in very low birth weight infants
Clerihew L, Austin N, McGuire W
Dates
Date edited: 22/08/2007
Date of last substantive update: 24/07/2007
Date of last minor update: / /
Date next stage expected 20/07/2009
Protocol first published: Issue 4, 2002
Review first published: Issue 1, 2003
Contact reviewer
Dr William McGuire
Associate Professor of Neonatology
Department of Paediatrics and Child Health
Australian National University Medical School
Canberra Hospital Campus
Canberra
ACT 2606 AUSTRALIA
Telephone 1: +61 2 62442222
Facsimile: +61 2 62443112
E-mail: william.mcguire@act.gov.au
Contribution of reviewers
Nicola Austin (NA) and William McGuire (WM) screened the title and abstract of all studies identified by the search strategy. Linda Clerihew (LC) and WM screened the full text of the report of each study identified as of potential relevance. LC and WM extracted the data separately, compared data, and resolved differences by consensus, and with discusion with NA. LC, NA, and WM completed the final review.Internal sources of support
Wishaw General Hospital, UK
Christchurch Womens Hospital, NEW ZEALAND
ANU Medical School, AUSTRALIA
External sources of support
NoneWhat's new
This review updates the review "Prophylactic intravenous antifungal agents to prevent mortality and morbidity in very low birth weight infants" published in the Cochrane Database of Systematic Reviews, The Cochrane Library, Issue 1, 2004 (McGuire 2004). For this update, the title was changed to "Prophylactic systemic antifungal agents to prevent mortality and morbidity in very low birth weight infants" since this better reflects the clinical context. Consequently, one small trial in which a systemic antifungal agent was administered enterally is now included (Violaris 1998).
The electronic search was updated in May 2007. Two new trials that fulfilled eligibility criteria were identified. One of these is the largest trial of this intervention yet reported (Manzoni 2007a). Inclusion of this trial more than doubled the total number of participants in the review. Inclusion of the data in the meta-analyses increased the precision of the estimates of effect size. The finding of a reduced incidence of invasive fungal infection in infants who received systemic antifungal prophylaxis was not altered. However, the previous finding of a statistically significantly lower mortality rate no longer holds.
Six observational studies of the intervention were found and we have described these in the excluded studies section.
Dates
Date review re-formatted: / /
Date new studies sought but none found: / /
Date new studies found but not yet included/excluded: / /
Date new studies found and included/excluded: 05/03/2007
Date reviewers' conclusions section amended: / /
Date comment/criticism added: / /
Date response to comment/criticisms added: / /
Text of review
Synopsis
Fungi such as candida (the organism that causes thrush) can cause severe infections in very low birth weight infants (birth weight less than 1.5 kilograms). These infections are often difficult to diagnose. Therefore, it may be appropriate to attempt to prevent such infections by giving all very low birth weight infants antifungal drugs as a routine part of their care. This review assessed whether evidence exists that such a practice prevents severe fungal infection, death, and disability in very low birth weight infants. There is evidence that giving infants an antifungal drug (fluconazole) regularly for the first four to six weeks after birth reduces the number of infants who develop severe infection. There is no convincing evidence that death or disability rates were affected. However, the findings were based on only a few trials, and further trials are needed.
Abstract
Background
Invasive fungal infection is an important cause of mortality and morbidity in very low birth weight infants. Early diagnosis is difficult, and treatment is often delayed. The available data are insufficient to conclude that topical/oral prophylaxis (usually nystatin and/or miconazole) prevents invasive fungal infection or mortality in very low birth weight infants. Systemic antifungal agents (usually azoles) are increasingly used as prophylaxis against invasive fungal infection.
Objectives
To assess the effect of prophylactic systemic antifungal therapy on mortality and morbidity in very low birth weight infants.
Search strategy
The standard search strategy of the Cochrane Neonatal Review Group was used. This included searches of the Cochrane Controlled Trials Register (The Cochrane Library, Issue 2, 2007), MEDLINE (1966 - May 2007), EMBASE (1980 - May 2007), conference proceedings, and previous reviews.
Selection criteria
Randomised controlled trials that compared the effect of prophylactic systemic antifungal therapy versus placebo, or no drug, or another antifungal agent or dose regimen, in very low birth weight infants.
Data collection & analysis
Data were extracted using the standard methods of the Cochrane Neonatal Review Group, with separate evaluation of trial quality and data extraction by each author, and synthesis of data using relative risk, risk difference, and weighted mean difference. The pre-specified outcomes were death prior to hospital discharge, long-term neurodevelopment, incidence of invasive fungal infection, emergence of antifungal resistance, and adverse drug reactions.
Main results
Seven eligible trials enrolling a total of 638 participating infants were identified. Meta-analysis of data from four trials that compared prophylactic fluconazole versus placebo revealed a statistically significant reduction in the risk of invasive fungal infection in the infants who received prophylaxis [typical relative risk: 0.23 (95% confidence interval 0.11, 0.46); typical risk difference: -0.11 (95% confidence interval -0.16, -0.06); number needed to treat: 9 (95% confidence interval 6, 17)]. There was no statistically significant difference in the risk of death prior to hospital discharge [typical relative risk: 0.61 (95% confidence interval 0.37, 1.03); typical risk difference: -0.05 (95% confidence interval -0.11, -0.00)]. Only one trial reported long term neurodevelopmental outcomes. There were no statistically significant differences in the incidence of developmental delay, or motor or sensory neurological impairment in children assessed at a median age of 16 months. One small trial that compared systemic versus oral/topical prophylaxis did not detect a statistically significant effect on invasive fungal infection or mortality. Two trials compared different dosing regimens of prophylactic intravenous fluconazole. These did not detect any significant differences in infection rates or mortality.
Reviewers' conclusions
Prophylactic systemic antifungal therapy reduces the incidence of invasive fungal infection in very low birth weight infants. This finding should be interpreted cautiously. The incidence of invasive fungal infection was very high in the control groups of some of the included trials. Furthermore, the trials may have been affected by ascertainment bias since use of prophylactic fluconazole may reduce the sensitivity of microbiological culture for detecting fungi in blood, urine, or cerebrospinal fluid. Meta-analysis does not demonstrate a statistically significant effect on overall mortality rates, but the 95% confidence interval around this estimate of effect is wide. There are currently only limited data on the long-term neurodevelopmental consequences for infants exposed to this intervention. In addition, there is a need for further data on the effect of the intervention on the emergence of organisms with antifungal resistance.
Background
Invasive fungal infection is an increasingly common cause of morbidity and mortality in very low birth weight infants (Kossoff 1998; Benjamin 2006). The incidence is between about 1% and 5% (Saiman 2000; Makhoul 2002; Clerihew 2006). In extremely low birth weight infants, the incidence has been reported to be as high as 10% (Karlowicz 2002). Additional specific risk factors include fungal colonisation, severe illness at birth, the use of multiple courses of antibiotics, the use of parenteral nutrition, the presence of a central venous catheter, and the use of histamine receptor subtype 2 antagonists (Huang 1998; Saiman 2000). Inter-unit variation in the incidence of invasive fungal infection is likely to be due to all or some of these population characteristics and clinical practices. The reported mortality rates of greater than 25% are higher than those attributed to nosocomial invasive bacterial infection in very low birth weight infants (Stoll 1996; Saiman 2000; Makhoul 2002; Stoll 2002). Invasive fungal infection is also associated with short and long term morbidity, including adverse neurodevelopmental outcomes (Friedman 2000; Saiman 2000).
The clinical presentation of invasive fungal and bacterial infection is similar. The diagnosis may be delayed due to an inability to consistently recover the organism from blood, cerebrospinal fluid, or urine. A high index of suspicion and the use of additional laboratory and clinical tests, including retinal examination, echocardiography, and renal ultrasonography, may be needed to confirm the suspected diagnosis (Benjamin 2003).
Given the difficulty in establishing an early diagnosis and the high level of associated morbidity and mortality, there is a need to assess the effect of strategies to prevent invasive fungal infection in very low birth weight infants. Prophylactic topical or oral non-absorbed antifungal agents (commonly, nystatin and/or miconazole) can prevent fungal colonisation. However, the currently available data are insufficient to conclude that topical/oral prophylaxis reduces the incidence of invasive fungal infection or mortality (Austin 2002). Over the past few years, the prophylactic use of systemic antifungal agents, principally the azole agent fluconazole, has been adopted as routine practice in some neonatal centres (Burwell 2006). This review sought to determine whether evidence exists that this practice prevents invasive fungal infection, and reduces mortality and morbidity, in very low birth weight infants. A further major consideration is the potential for antimicrobial prophylaxis to drive the emergence of drug resistance (Brion 2007).
Objectives
To assess the effect of prophylactic systemic antifungal therapy on mortality and adverse neurodevelopmental outcomes in very low birth weight infants.
The effects of the following interventions were examined:
1. Systemic antifungal prophylaxis versus placebo or no drug
2. Systemic antifungal agent versus oral/topical antifungal prophylaxis
3. One systemic antifungal agent versus another agent or dose regimen
The following subgroup analyses were pre-specified:
1. Extremely low birth weight infants (less than 1000 grams)
2. Infants with fungal colonisation at trial entry
Criteria for considering studies for this review
Types of studies
1. Controlled trials using random or quasi-random patient allocation.
2. Cluster randomised trials, where the unit of randomisation is the neonatal nursery.
Types of participants
Very low birth weight (birth weight less than 1500 grams) infants, with or without evidence of fungal colonisation, but without evidence of invasive fungal infection at study entry, cared for in a hospital setting.
Types of interventions
Trials comparing systemic antifungal prophylaxis with placebo or no drug, or oral/topical antifungal prophylaxis, or another systemic antifungal agent or dose regimen. The drug may have been given by the intravenous or enteral route.
Types of outcome measures
Primary outcomes:
1. Death prior to hospital discharge.
2. Neurodevelopmental outcomes during infancy and beyond using validated assessment tools: neurological evaluations, developmental scores, and classifications of disability, including auditory and visual disability.
3. Confirmed invasive fungal infection as determined by:
a. culture of fungus from a normally sterile site: cerebrospinal fluid, blood, urine, bone or joint, peritoneum, pleural space
b. findings on autopsy examination consistent with invasive fungal infection
c. findings on ophthalmological examination consistent with fungal ophthalmitis or retinitis
d. pathognomonic findings on renal ultrasound examination: "renal fungal balls"
Secondary outcomes:
1. Emergence of organisms resistant to antifungal agents: as detected in individual infants enrolled in the study, or, in the case of cluster-randomised studies, on surveillance of other infants in the same unit in the study centre (including infants who are admitted to the unit following completion of the study).
2. Adverse drug reactions attributed to the antifungal agent, such as rash (including Stevens-Johnson reactions), gastrointestinal disturbance, abnormal hepatic or renal function, cardiac arrhythmias, thrombophlebitis, seizures and anaphylaxis.
Search strategy for identification of studies
The standard search strategy of the Cochrane Neonatal Review Group was used. This included electronic searches of the Cochrane Controlled Trials Register (The Cochrane Library, Issue 2, 2007), MEDLINE (1966 - May 2007) and EMBASE (1980 - May 2007). The search strategy used the following text words and MeSH subject headings: Infant-Newborn, Infant-Low Birth Weight, Infant-Premature, infan$, neonat$, newborn, premature, low birth weight, LBW, fungi, fungemia, fungaemia, candidiasis, Candida albicans, anti fungal agents, fluconazole, azoles, amphotericin B, flucytosine. The searches were limited with the relevant filter for clinical trials. No language restriction was applied.
The references in studies identified as potentially relevant were examined. The abstracts from the Society for Pediatric Research and the European Society for Pediatric Research from 1980 until 2007 were searched. In 2003, all of the manufacturers of antifungal agents that are listed in the 2002 edition of the British National Formulary (BNF 2002): Bristol-Myers Squibb Pharmaceuticals Limited, Cambridge Laboratories, Elan Pharma Limited, Gilead Sciences Limited, ICN Pharmaceuticals Limited, Pfizer Limited were contacted. None provided any data that were unavailable from other sources.
Methods of the review
1. The reviewers screened the title and abstract of all of the studies identified by the above search strategy, and the full text of the report of each study identified as of potential relevance. These independent assessments followed pre-specified guidelines for inclusion. The decision to include or exclude a specific study was made by consensus of the reviewers.
2. The criteria and standard methods of the Cochrane Neonatal Review Group were used to assess the methodological quality of the included trials. Trial quality in terms of allocation concealment, blinding of parents or caregivers and assessors to intervention, and completeness of assessment in all randomised individuals was evaluated.
3. A data collection form to aid extraction of relevant information and data from each included study was used. Each reviewer extracted the data separately. These data were compared and differences were resolved by consensus.
4. The standard method of the Cochrane Neonatal Review Group was used to analyse and synthesize the data. The fixed effect model was used for meta-analysis. The effects were expressed as relative risk and 95% confidence interval and risk difference and 95% confidence interval for categorical data.
5. Heterogeneity between trial results was examined by inspecting the forest plots and quantifying the impact of heterogeneity in any meta-analysis using a measure of the degree of inconsistency in the studies' results (I2 statistic). If statistical heterogeneity was detected, the review authors explored the possible causes (for example, differences in study quality, participants, intervention regimens, or outcome assessments) using post hoc subgroup analyses.
Description of studies
Seven eligible trials were identified (Cabrera 2002; Kaufman 2001; Kaufman 2005; Kicklighter 2001; Manzoni 2007a; Manzoni 2007b; Violaris 1998; see Table, Characteristics of Included Studies). Two of the studies have been reported as an abstracts only (Cabrera 2002; Violaris 1998).
1. Four trials compared systemic antifungal prophylaxis versus placebo or no drug (Cabrera 2002; Kaufman 2001; Kicklighter 2001; Manzoni 2007a).
2. One trial compared systemic antifungal prophylaxis versus oral/topical antifungal therapy (Violaris 1998).
3. Two trials compared different dose regimens of systemic antifungal prophylaxis (Kaufman 2005; Manzoni 2007b).
Participants:
All of the trials have been undertaken in tertiary perinatal centres in North American or Europe within the past 10 years. In total, 638 infants participated. The participants were very low birth weight infants (Kicklighter 2001; Cabrera 2002; Manzoni 2007a; Manzoni 2007b; Violaris 1998), or extremely low birth weight infants (Kaufman 2001; Kaufman 2005). Documented fungal colonisation was an entry criterion for Cabrera 2002, but was not an entry criteria for the other trials.
Interventions:
1. Four trials compared intravenous antifungal prophylaxis (fluconazole in all cases) with placebo. 536 infants participated in total. Infants were enrolled within the first few days after birth. Kicklighter 2001 assigned treatment for 28 days. The drug or placebo was given intravenously until the infants tolerated enteral intake and then administered via an orogastric tube. Kaufman 2001 assigned the treatment for six weeks but discontinued administration when intravenous access was no longer available. Cabrera 2002 administered the drug intravenously initially then enterally when intravenous access was no longer in place. Manzoni 2007a assigned infants to the fluconazole or placebo from birth until 30 days after birth, or 45 days after birth for extremely low birth weight infants.
2. One small trial (N = 21) compared systemic antifungal prophylaxis (fluconazole) with oral/topical antifungal prophylaxis (nystatin) (Violaris 1998).
3. Two trials compared different dose regimens. Kaufman 2005 compared two regimes of prophylaxis with fluconazole (regimen A: 3 mg/kg body weight, every third day for the first two weeks, then every second day during the third and fourth weeks, then daily during the fifth and sixth weeks; regimen B: 3 mg/kg bodyweight twice weekly for six weeks). Infants were assigned to intervention for six weeks, or until intravenous access discontinued. Manzoni 2007a randomly allocated infants in the fluconazole group to either 3 mg/kg per 48 hours (regimen A) or 6 mg/kg per 48 hours (regimen B) for 30 days after birth (or 45 days for extremely low birth weight infants).
Outcomes:
The primary outcomes of the trials were fungal colonisation and invasive fungal infection. Data on deaths prior to hospital discharge were provided for six of the trials (Kaufman 2001; Kicklighter 2001; Kaufman 2005; Manzoni 2007a; Manzoni 2007b; Violaris 1998). Three of the studies monitored hepatic function with weekly assessments of the plasma levels of aspartate aminotransferase, alanine aminotransferase, total bilirubin, or alkaline phosphatase (Kaufman 2001; Kicklighter 2001; Kaufman 2005). These studies also monitored the fluconazole minimal inhibitory concentrations of fungal isolates (from both surface colonisation and from invasive infection) during the surveillance period. In Kaufman 2001 and Kaufman 2005, weekly surveillance cultures were collected during the period of prophylaxis. In Kicklighter 2001, surveillance began with the start of prophylaxis, and continued for four weeks after completing the prophylaxis. Cabrera 2002 collected surveillance cultures from day seven at weekly intervals until six weeks and began prophylaxis once surveillance cultures were positive. Only one trial assessed developmental outcomes (Kaufman 2001). These data have been published in abstract form only.
Excluded studies:
Six studies were excluded (see Table, Characteristics of Excluded Studies). These were single centre retrospective observational studies that compared outcomes for cohorts of very low birth weight or extremely low birth weight infants cared for in an epoch immediately prior to the introduction of intravenous antifungal prophylaxis (fluconazole in all studies) versus infants cared for in the epoch after this intervention was adopted (Aghai 2006; Bertini 2005; Dutta 2005; Healy 2005; Manzoni 2006; Uko 2006). All of these studies reported statistically significant reductions in the incidence of invasive fungal infection associated with the use of fluconazole prophylaxis. Only one study found a statistically significant difference in mortality rates (Aghai 2006). Although Aghai 2006 reported a lower rate of all cause mortality in infants treated with fluconazole prophylaxis, these infants also had statistically higher rates of exposure to antenatal corticosteroids and exogenous surfactant therapy.
Methodological quality of included studies
Quality assessments are included in the table, Characteristics of Included Studies. The included trials were generally of good methodological quality. In most studies, allocation was concealed by separating the randomisation process from recruitment and enrolment. Caregivers, investigators and assessors were all blind to the intervention. Follow-up appears to be complete for the outcomes reported.
Results
SYSTEMIC ANTIFUNGAL AGENT VERSUS PLACEBO OR NO DRUG (COMPARISON 01):
Four trials are included in this analysis (Cabrera 2002; Kaufman 2001; Kicklighter 2001;Manzoni 2007a):
Primary outcomes:
Death prior to hospital discharge (Outcome 01.01):
Data were reported by the three larger trials (Kaufman 2001; Kicklighter 2001; Manzoni 2007a). There was no statistically significant differences in the incidence of death prior to hospital discharge in any of the individual trials, or in a meta-analysis of data [typical relative risk: 0.61 (95% confidence interval 0.37, 1.03); typical risk difference: -0.05 (95% confidence interval -0.11, -0.00)]. There was no statistical heterogeneity in this meta-analysis.
Neurodevelopmental outcome:
Neurodevelopmental outcomes were reported by only one trial. Kaufman 2001 reported no significant differences in the incidence of developmental delay (modified Gesell test) or motor or sensory neurological impairment in infants assessed at a median age of 16 months. These findings were reported in abstract form only. When further data are available, these will be included in an update of this review.
Confirmed invasive fungal infection (Outcome 01.02):
Kaufman 2001 and Manzoni 2007a reported statistically significantly lower incidences of invasive fungal infection in the fluconazole group. Kicklighter 2001 and Cabrera 2002 did not find any statistically significant differences. Meta-analysis of data from the four trials found a statistically significantly lower incidence of invasive fungal infection in the fluconazole group [typical relative risk: 0.23 (95% confidence interval 0.11, 0.46); typical risk difference: -0.11 (95% confidence interval -0.16, -0.06); number needed to treat: 9 (95% confidence interval 6, 17)]. There was no statistical heterogeneity in this meta-analysis.
Secondary outcomes:
Emergence of organisms resistant to antifungal agents:
Kaufman 2001 did not find any statistically significant changes in the minimal inhibitory concentration of fluconazole for fungal isolates during the 30 months study period. The data were not presented separately for isolates from infants in the fluconazole and placebo groups. Kicklighter 2001 did not find any statistically significant differences in the minimal inhibitory concentration of fluconazole for fungal isolates (Candida albicans isolates only assessed) between the fluconazole and placebo groups during the treatment period or for four weeks after discontinuation of the study drug. Manzoni 2007a stated that "patterns of sensitivity to fluconazole remained the same". This was reported in abstract form only. If further data become available, these will be included in an update of this review.
Adverse drug reactions attributed to the antifungal agent:
There were no clinically significant adverse reactions attributed to fluconazole in the included studies. No infants were withdrawn from the trials because of adverse effects of fluconazole.
Subgroup analyses:
Infants with birth weight less than 1000 grams:
Kaufman 2001 and Kaufman 2005 enrolled only infants with birth weight less than 1000 grams. Manzoni 2007a stated that there was a statistically significantly lower incidence of invasive fungal infection in the subgroup of infants of birth weight less than 1000 grams. This was reported in abstract form only and no numerical data were presented. The abstract made no comment on mortality rates in extremely low birth weight infants. When these data become available, they will be included in an update of this review. Kicklighter 2001 enrolled infants with birth weight less than 1500 grams. A subgroup analysis of extremely low birth weight infants has not been possible.
Infants with fungal colonisation at entry to study:
Only the smallest trial restricted participation to infants with fungal colonisation (Cabrera 2002). Subgroup analysis of infants with fungal colonisation was not possible with the available data from the other trials.
SYSTEMIC ANTIFUNGAL AGENT VERSUS ORAL OR TOPICAL ANTIFUNGAL THERAPY (COMPARISON 02):
One trial is included in this analysis Violaris 1998)
Primary outcomes:
Death prior to hospital discharge (Outcome 02.01):
Violaris 1998 found no significant difference in death prior to hospital discharge [relative risk: 0.17 (95% confidence interval 0.01, 2.84); risk difference: -0.31 (95% confidence interval -0.62, 0.01)].
Confirmed invasive fungal infection (Outcome 02.02):
Violaris 1998 found no significant difference in confirmed invasive fungal infection [relative risk: 0.17 (95% confidence interval 0.01, 2.84); risk difference: -0.31 (95% confidence interval -0.62, 0.01)].
No other outcomes were reported by Violaris 1998. If further data become available these will be included in an update of this review.
Subgroup analyses:
Infants with birth weight less than 1000 grams: This analysis was not possible.
Infants with fungal colonisation at entry to study: This analysis was not possible.
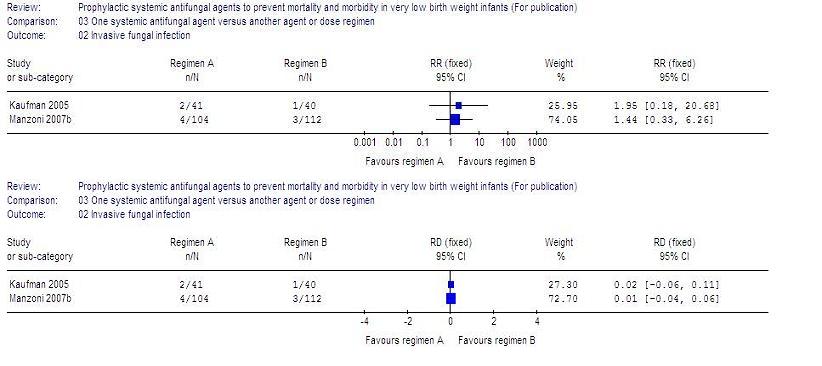
ONE SYSTEMIC ANTIFUNGAL AGENT VERSUS ANOTHER AGENT OR DOSE REGIMEN (COMPARISON 03):
Two trials are included in this analysis (Kaufman 2005; Manzoni 2007a):
Primary outcomes:
Death prior to hospital discharge (Outcome 03.01):
Kaufman 2005 found no statistically significant difference between the two dose regimens [relative risk: 0.98 (95% confidence interval 0.34, 2.77); typical risk difference 0.00 (95% confidence interval -0.16, 0.15)].
Manzoni 2007a found no statistically significant difference between the two dose regimens [relative risk: 1.08 (95% confidence interval 0.44, 2.61); typical risk difference 0.01 (95% confidence interval -0.07, 0.08)].
Neurodevelopmental outcome: Not reported by either trial.
Confirmed invasive fungal infection (Outcome 03.02):
Kaufman 2005 found no statistically significant difference in confirmed invasive fungal infection [relative risk 1.95 (95% confidence interval 0.18, 20.68); risk difference 0.02 (95% confidence interval -0.06, 0.11)].
Manzoni 2007a: found no statistically significant difference [relative risk 1.44 (95% confidence interval 0.33, 6.26); risk difference 0.01 (95% confidence interval -0.04, 0.11)].
Secondary outcomes:
Emergence of organisms resistant to antifungal agents:
Kaufman 2005 did not find any statistically significant difference in the mean minimal inhibitory concentration of fluconazole for fungi isolated from surveillance cultures of infants during the first 12 months versus the second 12 months of the study.
Manzoni 2007a stated that "patterns of sensitivity to fluconazole remained the same". This was reported in abstract form only. If further data become available, these will be included in an update of this review.
Adverse drug reactions attributed to the antifungal agent:
There were no clinically significant adverse reactions attributed to fluconazole, and no infants were withdrawn from either study.
Subgroup analyses:
Infants with birth weight less than 1000 grams:
All participants in Kaufman 2005 were of birth weight less than 1000 grams.
Manzoni 2007a: Subgroup analyses for extremely low birth weight infants are not possible with the currently reported data. When further data are available, these will be included in an update of this review.
Infants with fungal colonisation at entry to study: This analysis was not possible.
Discussion
The available data suggest that prophylactic systemic antifungal therapy reduces the incidence of invasive fungal infection in very low birth weight infants. The pooled effect size estimates that treating nine infants with prophylactic fluconazole would prevent one extra case on invasive fungal infection. The included trials were generally of good methodological quality and the absence of statistical heterogeneity in the meta-analysis suggests that the estimate is robust. However, this finding should be interpreted and applied with caution for several reasons.
In the trials that contributed most weight to the pooled estimate of effect size (Kaufman 2001; Manzoni 2007a), the reported incidences of invasive fungal infection in the placebo groups were much higher than in other large cohort studies (Karlowicz 2002; Kossoff 1998; Clerihew 2006). Applying this finding to units with lower incidences of invasive fungal infection would require treatment of a much larger number of infants to prevent a single extra case of invasive fungal infection.
Secondly, the diagnostic sensitivity of microbiological culture for invasive fungal infection is lower in infants receiving systemic antifungal treatment (Schelonka 2003). This may cause selective under-diagnosis in the treatment group and over-estimation of the effect size. For that reason, mortality was included as a primary outcome for this review, since ascertaining this outcome is not likely to be affected by bias. Furthermore, as it is often difficult to define precisely the cause of death in very low birth weight infants, and since invasive fungal infection is not always diagnosed, all-cause mortality rather than death attributed to fungal infection was pre-specified. The review did not find a statistically significant effect of prophylactic systemic antifungal therapy on all-cause mortality. The mortality rates in the placebo cohorts were similar to rates in large cohort studies of very low birth weight infants cared for in similar settings (Horbar 2002). However, the 95% confidence interval around this estimate of effect is wide (63% risk reduction to 3% risk increase). When data from further trials are available, these may be included in this meta-analysis to provide a more precise estimate of the effect on mortality.
Regarding the potential adverse effects of prophylactic fluconazole, there were no clinically significant drug-related adverse events reported in these trials, nor was any infant withdrawn from any study because of unacceptable adverse reactions. To date, fluconazole has appeared to be a safe treatment for newborn infants with invasive fungal infection. Only mild and transient elevation of plasma levels of hepatic enzymes has been described as a common side effect (Huttova 1998). However, there are rare but important side effects such as toxic epidermal necrolysis and Stevens-Johnson syndrome reported in other populations of patients. If fluconazole exposure becomes more widespread through use as prophylaxis, then these side effects may be observed in newborn infants. Additionally, widespread use of prophylactic fluconazole may increase the risk of potential drug interactions with medications that are prescribed for very low birth weight infants, including theophylline, and thiazide diuretics (Neely 2001).
There is concern that widespread use of systemic antifungal prophylaxis may lead to the emergence of antifungal resistance. A meta-analysis of trials of fluconazole prophylaxis in immunosuppressed adults found evidence of an increased risk for colonization, but not invasive infection, with fungi partially or completely resistant to fluconazole (Brion 2007). Although the data available from the trials identified in this review are reassuring in terms of the emergence of fluconazole resistance, the follow-up periods of the trials are probably insufficient to detect clinically significant changes in the resistance profile of fungal isolates. There is a need for continuing mycological surveillance in neonatal units where systemic antifungal prophylaxis is used.
Limiting prophylaxis to infants at highest risk may help delay the emergence of antifungal resistance. Since invasive fungal infection is about twice as common in extremely low birth weight than very low birth weight infants, targeting prophylaxis to this population reduces the number of infants who need to be exposed to fluconazole. A subgroup analysis of extremely low birth weight infants was planned, but the data are not available from the published reports of the two largest trials (Kicklighter 2001; Manzoni 2006). If these data become available, they will be included in a future update of the review. Even within the extremely low birth weight population, the burden of invasive fungal infection is confined to the smallest and least mature infants (Clerihew 2006). Invasive fungal infection is three time more common in infants born before 26 weeks' gestation, or with birth weight less than 750 grams, than in infants of birth weight 750 grams to less than 1000 grams. Evidence exists that clinicians who use systemic antifungal prophylaxis already target the smallest and least mature infants with additional risk factors for invasive fungal infection (Burwell 2006). It may be appropriate to focus future research efforts on this risk high population.
Similarly, a planned subgroup analysis of outcomes for infants who were colonised with fungi at trial entry was not possible. Colonisation, especially heavy gastrointestinal colonisation, has been suggested as a risk factor for invasive infection by some (PappuKatikaneni 1990), but not other (Huang 1998; Saiman 2000) observational studies. The subgroup data for only those infants colonised at trial entry were not available in the published reports of the largest studies (Kaufman 2005; Kicklighter 2001; Manzoni 2007a). As only about 10% of all of the participating infants were colonised at trial entry, it is unlikely that the analysis of these small numbers will provide clinically useful findings.
Finally, it is plausible that limiting the exposure of infants to systemic antifungal prophylaxis by using less intensive dose regimens may help in limiting the emergence of antifungal resistance. Two trials compared "standard" dosing regimens to less intensive/lower dose regimens (Kaufman 2005; Manzoni 2007b). Neither found statistically significant differences on mortality before hospital discharge or incidence of invasive fungal infection. However, the 95% confidence intervals were wide and further trials are need to identify the most appropriate dosing regimen for this intervention.
Reviewers' conclusions
Implications for practice
There is some evidence that prophylactic systemic antifungal agents reduce invasive fungal infection in very low birth weight infants, but the currently available data do not find a statistically significant effect on mortality, and there are only limited data on long term neurodevelopmental outcomes. Lower dose regimens appear to be as effective at preventing invasive fungal infection as more frequently administered prophylaxis, but the 95% confidence intervals for these estimates are wide.
Implications for research
Further randomised controlled trials of systemic antifungal prophylaxis are needed to provide more precise estimates of effect size. Because most neonatologists who currently use systemic antifungal prophylaxis target infants thought to be at greatest risk, mainly extremely low birth weight or extremely preterm infants with additional risk factors, a trial restricted in this population of infants, or perhaps even smaller or lower gestation infants, may be appropriate and acceptable (Burwell 2006). Systemic antifungal prophylaxis may be compared with placebo, or with topical/oral prophylaxis. Any trial should aim to assess long-term outcomes, particularly disability-free survival, as well as the effect on invasive fungal infection. Finally, although randomised controlled trials may attempt to measure the effect of prophylaxis on antifungal resistance, there is also a need for on-going local and national surveillance to detect the emergence of resistant organisms, particularly if prophylactic use of fluconazole becomes more widespread.
Acknowledgements
We thank Dr David Kaufman and Dr Stephen Kicklighter for providing clarification on some aspects of their studies. We are grateful to Bristol-Myers Squibb Pharmaceuticals Limited, Cambridge Laboratories, Elan Pharma Limited, Gilead Sciences Limited, ICN Pharmaceuticals Limited, and Pfizer Limited for searching their respective databases for unpublished data.
Potential conflict of interest
William McGuire was the principal investigator in a national prospective surveillance study in the United Kingdom of invasive fungal infection in very low birth weight infants. This study was partly supported by Pfizer, the manufacturer of fluconazole.
Characteristics of included
studies
| Study | Methods | Participants | Interventions | Outcomes | Notes | Allocation concealment |
| Cabrera 2002 | Blinding of randomisation: Yes Blinding of intervention: Yes Complete follow-up: Yes Blinding of outcome measurement: Yes | 11 infants of birthweight less than 1500 g with fungal colonisation demonstrated on rectal, oro-pharyngeal, or tracheal weekly surveillance cultures.
Medical School of Georgia, Augusta, before 2002. | Fluconazole (N=6) 6 mg / kg body weight, versus placebo (N=5). The dosage interval is not known. The study drug was given intravenously until intravenous access was no longer otherwise required, when oral study drug was given. The total duration of treatment with the study drug, or of follow up is not clear. | Invasive fungal infection. | Published in abstract form only (additional data obtained from authors). | D |
| Kaufman 2001 | Blinding of randomisation: Yes Blinding of intervention: Yes Complete follow-up: Yes Blinding of outcome measurement: Yes | 100 infants less than five days old, and of birthweight less than 1000 g. Infants with evidence of liver failure were not eligible for inclusion.
University of Virginia School of Medicine, Charlottesville.
1998- 2000. | Fluconazole (N=50) 3 mg / kg body weight, every third day for the first two weeks, then every second day during the third and fourth weeks, then daily during the fifth and sixth weeks versus normal saline placebo (N=50). Assigned to intervention for six weeks, or until intra-venous access discontinued. | Fungal colonisation and invasive infection. Emergence of fluconazole resistance.
Adverse drug reactions.
Incidence of bacterial infections, necrotising enterocolitis, isolated intestinal perforation, ligation of patent ductus arteriosus, retinopathy of prematurity, abnormal findings on cranial ultrasonography.
Death prior to hospital discharge.
| Kaufman 2001 reported that 13 of the 50 infants in the placebo group developed invasive fungal infection. Ten episodes were detected during the six weeks period when the intervention was administered, and three episodes occurred following discontinuation of the intervention. There were no episodes of invasive fungal infection in the fluconazole group during the six weeks intervention period. One case occurred following discontinuation of the intervention.
In the report of the outcomes in abstract form
(published in Pediatric Research), the investigators state that invasive fungal infection occurred in nine, rather than 10, infants in the placebo group during the six-weeks treatment period, and in two, rather than three, infants in the control group. These differences were related to less information being available at the time that the first (abstract) report was prepared (personal communication Dr Kaufman).
| A |
| Kaufman 2005 | Blinding of randomisation:
YesBlinding of intervention: Yes Complete follow-up: Yes Blinding of outcome measurement: Yes
| 81 infants of birthweight less than 1000 grams, less than 5 days old, and with either an endotracheal tube or central venous catheter in situ. | Regimen A (N=41): Fluconazole 3 mg/kg body weight, every third day for the first two weeks, then every second day during the third and fourth weeks, then daily during the fifth and sixth weeks
Regimen B (N=40): Fluconazole 3mg/kg bodyweight twice weekly for 6 weeks.
Assigned to intervention for six weeks, or until intravenous access discontinued. | Fungal colonisation and invasive infection. Mortality (all cause) was reported as a secondary outcome. | | A |
| Kicklighter 2001 | Blinding of randomisation: Yes Blinding of intervention: Yes Complete follow-up: Yes Blinding of outcome measurement: Yes
| 103 infants less than three days old, and of birthweight less than 1500 g. Infants with evidence of liver failure, congenital heart disease, or congenital defects needing surgery were not eligible for inclusion.
University of Medical University of South Carolina.
1998- 1999. | Fluconazole (N=53) 6 mg / kg body weight (N=112), or fluconazole 3 mg/kg (N=104), or placebo (N=106) every second day from birth until the 30th day after birth (or 45th day in infants of birth weight less than 1000 grams). Administered intravenously and then oro-gastrically when tolerated. | Fungal colonisation and invasive infection. Emergence of fluconazole resistance.
Adverse drug reactions.
Death prior to hospital discharge was also reported. | | A |
| Manzoni 2007a | Blinding of randomisation: Yes Blinding of intervention: Yes Complete follow-up: Yes Blinding of outcome measurement: Yes
| 322 infants of birthweight less than 1500 grams.
Eight level III neonatal units in Turin, Rome, Milan, or Pavia, Italy (2004-2006). | Fluconazole 3 mg/kg or 6 mg/kg body weight, every second day from birth for 30 days, or 45 days for extremely low birth weight infants (N=216) versus placebo (N=106). | Fungal colonisation and invasive infection. Emergence of fluconazole resistance.
Death prior to hospital discharge was also reported. | | A |
| Manzoni 2007b | Blinding of randomisation: Yes Blinding of intervention: Yes Complete follow-up: Yes Blinding of outcome measurement: Yes
| 216 infants of birthweight less than 1500 grams.
Eight level III neonatal units in Turin, Rome, Milan, or Pavia, Italy (2004-2006). | Fluconazole 3 mg/kg (N=104) versus fluconazole 6 mg/kg (N=112), every second day from birth for 30 days, or 45 days for extremely low birth weight infants. | Fungal colonisation and invasive infection. Emergence of fluconazole resistance.
Death prior to hospital discharge was also reported. | This population forms the intervention cohort in Manzoni 2007a. | A |
| Violaris 1998 | Blinding of randomisation: Can't tell Blinding of intervention: No Complete follow-up: Yes Blinding of outcome measurement: No
| 21 infants of birthweight less than 1500 grams.
Place and time not stated.
| Fluconazole (4mg/kg) orally (N=8) versus nystatin (100,000 units/kg/day) in each side of the mouth (N=13), beginning on day five after birth. Medications were continued until full oral feedings were attained or systemic fungal infection was diagnosed.
| Invasive fungal infection and mortality. | Published in abstract form only. | B |
Characteristics of excluded studies
| Study | Reason for exclusion |
| Aghai 2006 | Not a randomised controlled trial. Observational study of extremely low birth weight infants cared for in pre-and post- fluconazole prophylaxis epochs at Cooper University Hospital, New Jersey, USA (1998-2005). |
| Bertini 2005 | Not a randomised controlled trial. Observational study at Careggi University Hospital, Florence, Italy. Compared outcomes for very low birth infants during a baseline period (1998-2000) with infants cared for during a study period (2001-2003) when infants received fluconazole prophylaxis. |
| Dutta 2005 | Not a randomised controlled trial. Retrospective observational study in Chandigarh, India. Compared incidences of invasive fungal infection in newborn infants cared for in a level III neonatal unit during pre- and post-fluconazole prophylaxis epochs. |
| Healy 2005 | Not a randomised controlled trial. Observational study of extremely low birth weight infants cared for in the Women's Hospital of Texas, USA prior to the introduction of fluconazole prophylaxis (2000-2001) and after the introduction of prophylaxis (2002-2004). |
| Manzoni 2006 | Not a randomised controlled trial. Retrospective cohort study of very low birth weight infants in Santa'Anna, Torino, Italy (2000-2005). Outcomes compared between two epochs pre- and post- fluconazole prophylaxis. |
| Uko 2006 | Not a randomised controlled trial. Observational study of very low birth weight infants cared for in pre-and post- fluconazole prophylaxis epochs at the Children's Hospital at Montefiore, New York, USA (2001-2004). |
References to studies
References to included studies
Cabrera 2002 {published data only}Cabrera C, Frank M, Carter D, Bhatia J. Fluconazole prophylaxis against systemic candidiasis after colonization: a randomized, double-blinded study. In: Journal of Perinatology. Vol. 22. 2002:604.
Kaufman 2001 {published data only}
* Kaufman D, Boyle R, Hazen KC, Patrie JT, Robinson M, Donowitz LG. Fluconazole prophylaxis against fungal colonization and infection in preterm infants. New England Journal of Medicine 2001;345:1660-6.
Kaufman D, Boyle R, Hazen KC, Robinson M, Donowitz LG. Effectiveness of fluconazole prophylaxis in the prevention of colonization and invasive infection in preterm infants. Pediatric Research 2001;50:309A.
Kaufman D, Boyle R, Robinson M, Grossman LB. Long-term safety of intravenous prophylactic fluconazole use in preterm infants less than 1000 grams. In: Pediatric Academic Societies. PAS2003:53:2735.
Kaufman 2005 {published data only}
Kaufman D, Boyle R, Hazen K, Patrie J, Robinson M, Grossman LB. Twice weekly fluconazole for prophylaxis for prevention of invasive fungal infection in high-risk infants of <1000g birthweight. Journal of Pediatrics 2005;147:172-9.
Kicklighter 2001 {published data only}
* Kicklighter SD, Springer SC, Cox T, Hulsey TC, Turner RB. Fluconazole for prophylaxis against candidal rectal colonization in the very low birth weight infant. Pediatrics 2001;107:293-8.
Kicklighter SD, Springer SC, Phaller MA, Messer S, Cox T, Hulsey TC, Turner RB. Fluconazole for prophylaxis against fungal rectal colonization in the very low birth weight infant. Pediatric Research 2000;47:342A.
Manzoni 2007a {published data only}
Manzoni P, Stolfi I, Pugni L, Decembrino L, Magnani C, Vetrano G, et al. A multicenter, randomized trial of prophylactic fluconazole in preterm neonates. New England Journal of Medicine 2007;356:2483-95.
Manzoni 2007b {published data only}
Manzoni P, Stolfi I, Pugni L, Decembrino L, Magnani C, Vetrano G, et al. A multicenter, randomized trial of prophylactic fluconazole in preterm neonates. New England Journal of Medicine 2007;356:2483-95.
Violaris 1998 {published data only}
Violaris K, Doraiswamy B, Olawepo O, Gulrajani-LaCorte M. Fluconazole versus nystatin prophylaxis for fungal infection in very low birth weight (VLBW) infants. In: Pediatric Research. Vol. 44. 1998:254A.
References to excluded studies
Aghai 2006 {published data only}Aghai ZH, Mudduluru M, Nakhla TA, Amendolia B, Longo D, Kemble N, Kaki S, Sutsko R, Saslow JG, Stahl GE. Fluconazole prophylaxis in extremely low birth weight infants: association with cholestasis. Journal of Perinatology 2006;26:550-5.
Bertini 2005 {published data only}
Bertini B, Perugi S, Dani C, Filipp L, Pratesi S, Rubaltelli F. Fluconazole prophylaxis prevents invasive fungal infection in high-risk very low birthweight infants. Journal of Pediatrics 2005;147:162-5.
Dutta 2005 {published data only}
Dutta S, Murki S, Varma S, Narang A, Chakrabarti A. Effects of cessation of a policy of neonatal fluconazole prophylaxis on fungal resurgence. Indian Pediatrics 2005;42:1226-30.
Healy 2005 {published data only}
Healy CM, Baker CJ, Zaccaria E, Campbell JR. Impact of fluconazole prophylaxis on incidence and outcome of invasive candidiasis in a neonatal intensive care unit. Journal of Pediatrics 2005;147:166-71.
Manzoni 2006 {published data only}
Manzoni P, Agrisio R, Mostert M, Leonessa M, Farina D, Latino M, Gomirato G. Prophylactic fluconazole is effective in preventing fungal colonization and fungal systemic infections in preterm neonates: a single-center, 6-year retrospective cohort study. Journal of Pediatrics 2006;117:e22-e32.
Uko 2006 {published data only}
Uko S, Soghier LM, Vega M, Marsh J, Reinersman GT, Herring L, Dave VA, Nafday S, Brion LP. Targeted short-term fluconazole prophylaxis among very low birth weight and extremely low birth weight infants. Pediatrics 2006;117:1243-52.
* indicates the primary reference for the study
Other references
Additional references
Austin 2002Austin NC, Darlow B. Prophylactic oral anti-fungal agents to prevent systemic candida infection in preterm infants. Cochrane Database of Systematic Reviews 2003, Issue 4.
Benjamin 2003
Benjamin DK Jr, Poole C, Steibach WJ, Rowen JL, Walsh TJ.. Neonatal candidemia and end-organ damage: a critical appraisal of the literature using meta-analytic techniques. Pediatrics 2003;112:634-40.
Benjamin 2006
Benjamin DK Jr, Stoll BJ, Fanaroff AA, McDonald SA, Oh W, Higgins RD et al. Neonatal candidiasis among extremely low birth weight infants: risk factors, mortality rates, and neurodevelopmental outcomes at 18 to 22 months. Pediatrics 2006;117:84-92.
BNF 2002
Joint Formulary Committee. British National Formulary. 43 edition. London, UK: British Medical Association and Royal Pharmaceutical Society of Great Britain, 2002.
Botas 1995
Botas CM, Kurlat I, Young SM, Sola A. Disseminated candidal infections and intravenous hydrocortisone in preterm infants. Pediatrics 1995;95:883-7.
Brion 2007
Brion LP, Uko SE, Goldman DL. Risk of resistance associated with fluconazole prophylaxis: Systematic review. Journal of Infection 2007:Epub ahead of print.
Burwell 2006
Burwell LA, Kaufman D, Blakely J, Stoll BJ, Fridkin SK. Antifungal prophylaxis to prevent neonatal candidiasis: a survey of perinatal physician practices. Pediatrics 2006;118:e1019-26.
Clerihew 2006
Clerihew L, Lamagni TL, Brocklehurst P, McGuire W. Invasive fungal infection in very low birthweight infants: national prospective surveillance study. Archives of Disease in Childhood 2006;91:F188-92.
Friedman 2000
Friedman S, Richardson SE, Jacobs SE, O'Brien K. Systemic candida infection in extremely low birth weight infants: short term morbidity and long term neurodevelopmental outcome. Pediatric Infectious Diseases Journal 2000;19:499-504.
Horbar 2002
Horbar JD, Badger GJ, Carpenter JH, Fanaroff AA, Kilpatrick S, LaCorte M, Phibbs R, Soll RF; Members of the Vermont Oxford Network. Trends in mortality and morbidity for very low birth weight infants, 1991–1999. Pediatrics 2002;110:143-51.
Huang 1998
Huang YC, Li CC, Lin TY. Association of fungal colonization and invasive disease in very low birth weight infants. Pediatric Infectious Diseases Journal 1998;17:819-22.
Huttova 1998
Huttova M, Hartmanova I, Kralinsky K, Filka J, Uher J, Kurak J, Krizan S, Krcmery V Jr. Candida fungemia in neonates treated with fluconazole: report of forty cases, including eight with meningitis. Pediatric Infectious Diseases Journal 1998;17:1012-5.
Karlowicz 2002
Karlowicz MG, Rowen JL, Barnes-Eley ML, Burke BL, Lawson ML, Bendel CM, Shattuck KE, Horgan M, Albritton WL. The role of birth weight and gestational age in distinguishing extremely low birth weight infants at high risk of developing candidemia from infants at low risk: a multicenter study. Pediatric Research 2002;51:301A.
Kossoff 1998
Kossoff EH, Buescher ES, Karlowicz MG. Candidemia in a neonatal intensive care unit: trends during fifteen years and clinical features of 111 cases. Pediatric Infectious Diseases Journal 1998;17:504-8.
Makhoul 2002
Makhoul IR, Sujov P, Smolkin T, Lusky A, Reichman B. Epidemiological, clinical, and microbiological characteristics of late-onset sepsis among very low birth weight infants in Israel: a national survey. Pediatrics 2002;109:34-9.
Marr 2000
Marr KA, Seidel K, White TC, Bowden RA. Candidemia in allogeneic blood and marrow transplant recipients: evolution of risk factors after the adoption of prophylactic fluconazole. Journal of Infectious Diseases 2000;181:309-16.
Neely 2001
Neely MN, Schreiber JR. Fluconazole prophylaxis in the very low birth weight infant: not ready for prime time. Pediatrics 2001;107:404-5.
PappuKatikaneni 1990
Pappu-Katikaneni LD, Rao KP, Banister E. Gastrointestinal colonization with yeast species and Candida septicemia in very low birth weight infants. Mycoses 1990;33:20-3.
Pfaller 2002
Pfaller MA, Diekema DJ, Jones RN, Messer SA, Hollis RJ; SENTRY Participants Group. Trends in antifungal susceptibility of Candida spp. isolated from pediatric and adult patients with bloodstream infections: SENTRY Antimicrobial Surveillance Program, 1997 to 2000. Journal of Clinical Microbiology 2002;40:352-6.
Saiman 2000
Saiman L, Ludington E, Pfaller M, Rangel-Frausto S, Wiblin RT, Dawson J, Blumberg HM, Patterson JE, Rinaldi M, Edwards JE, Wenzel RP, Jarvis W. Risk factors for candidemia in neonatal intensive care unit patients. The National Epidemiology of Mycosis Survey Study Group. Pediatric Infectious Diseases Journal 2000;19:319-24.
Schelonka 2003
Schelonka RL, Moser SA. Time to positive culture results in neonatal Candida septicemia. Journal of Pediatrics 2003;142:564-5.
Stoll 1996
Stoll BJ, Gordon T, Korones SB, Shankaran S, Tyson JE, Bauer CR, Fanaroff AA, Lemons JA, Donovan EF, Oh W, Stevenson DK, Ehrenkranz RA, Papile LA, Verter J, Wright LL. Late-onset sepsis in very low birth weight neonates: a report from the National Institute of Child Health and Human Development Neonatal Research Network. Journal of Pediatrics 1996;129:63-71.
Stoll 2002
Stoll BJ, Hansen N, Fanaroff AA, Wright LL, Carlo WA, Ehrenkranz RA, Lemons JA, Donovan EF, Stark AR, Tyson JE, Oh W, Bauer CR, Korones SB, Shankaran S, Laptook AR, Stevenson DK, Papile LA, Poole WK. Late-onset sepsis in very low birth weight neonates: the experience of the NICHD Neonatal Research Network. Pediatrics 2002;110:285-91.
Vohr 2000
Vohr BR, Wright LL, Dusick AM, Mele L, Verter J, Steichen JJ, Simon NP, Wilson DC, Broyles S, Bauer CR, Delaney-Black V, Yolton KA, Fleisher BE, Papile LA, Kaplan MD. Neurodevelopmental and functional outcomes of extremely low birth weight infants in the National Institute of Child Health and Human Development Neonatal Research Network, 1993-1994. Pediatrics 2000;105:1216-26.
Other published versions of this review
McGuire 2004McGuire W, Clerihew L, Austin N. Prophylactic intravenous antifungal agents to prevent mortality and morbidity in very low birth weight infants. Cochrane Database of Systematic Reviews 2004, Issue 1.
Comparisons and data
| Comparison or outcome |
Studies |
Participants |
Statistical method |
Effect size |
| 01 Systemic antifungal agent versus placebo
or no drug |
| 01 Death prior to hospital discharge |
3 |
525 |
RR (fixed), 95% CI |
0.61 [0.37, 1.03] |
| 02 Invasive fungal infection |
4 |
536 |
RR (fixed), 95% CI |
0.23 [0.11, 0.46] |
| 02 Systemic antifungal agent versus oral/topical
antifungal prophylaxis |
| 01 Death prior to hospital discharge |
1 |
21 |
RR (fixed), 95% CI |
0.17 [0.01, 2.84] |
| 02 Invasive fungal infection |
1 |
21 |
RR (fixed), 95% CI |
0.17 [0.01, 2.84] |
| 03 One systemic antifungal agent versus another
agent or dose regimen |
| 01 Death prior to hospital discharge |
|
|
RR (fixed), 95% CI |
No total |
| 02 Invasive fungal infection |
|
|
RR (fixed), 95% CI |
No total |
01 Systemic antifungal agent versus placebo or no drug
01.01 Death prior to hospital discharge
01.02 Invasive fungal infection
02 Systemic antifungal agent versus oral/topical antifungal prophylaxis
02.01 Death prior to hospital discharge
02.02 Invasive fungal infection
03 One systemic antifungal agent versus another agent or dose regimen
03.01 Death prior to hospital discharge
03.02 Invasive fungal infection
Contact details for co-reviewers
Dr Nicola Austin
Neonatologist
NICU
Christchurch Womens Hospital
Christchurch Womens Hospital
Christchurch
NEW ZEALAND
Telephone 1: 640303644699
Facsimile: 6433644883
E-mail: nicola.austin@cdhb.govt.nz
Dr Linda Clerihew, MRCPCH
Specialist Registrar
Tayside Institute of Child Health
Ninewells Hospital and Medical School
Dundee
UK
DD1 9SY
Telephone 1: +44 1382 632179
E-mail: l.clerihew@dundee.ac.uk
| This review is published as a Cochrane review in The Cochrane Library,
Issue 4, 2007 (see http://www.thecochranelibrary.com for information).
Cochrane reviews are regularly updated as new evidence emerges and in response
to feedback. The Cochrane Library should be consulted for the most recent
version of the review. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}