Background - Methods - Results - Characteristics of Included Studies - References - Data Tables & Graphs
Dr. Linda Genen
Literature search and identification of trials
Evaluation of methodological quality
Data collection
Verification of data
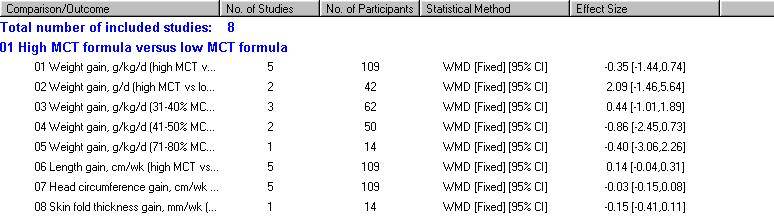
There was no evidence of difference in short term growth parameters when high and low MCT formulas were compared. The meta-analysis of weight gain based on five studies yielded a WMD of -0.35 g/kg/d (95% CI -1.44, 0.74). Similarly, meta-analysis of weight gain in g/d based on two studies showed no evidence of difference (WMD 2.09 g/d, 95% CI -1.46, 5.64). Length gain, based on five studies, showed a non-significant WMD of 0.14 cm/wk (95% CI -0.04, 0.31). Head circumference gain, based on data from five studies, showed a non-significant WMD -0.03 cm/wk (95% CI -0.15, 0.08). Only one study reported skin fold thickness gain, with a mean difference -0.15 mm/wk (95% CI -0.41, 0.11), again not significant.
Subgroup analyses according to % MCT in the high MCT formula, by 10% intervals, showed no evidence of effect of high MCT on short term weight gain within any subgroup.
There are conflicting data (two studies) as to formula tolerance.
There is no evidence of effect on incidence of necrotizing enterocolitis (NEC), based on small numbers in two trials.
No studies were located addressing long term growth parameters or neurodevelopmental outcomes.
Dietary energy is essential for promoting growth in the preterm infant. Fat is an integral energy source, and is also needed for cell membranes and proper brain development. Fat comprises 40-50% of calories in human milk or formula (Hamosh 1991a). Long chain triglycerides (LCT) contain long chain fatty acids which make up 75-80% of all fatty acids in human milk. The long chain polyunsaturated fatty acids (a subset of long chain fatty acids) are higher in preterm as compared to term human milk. Medium chain triglycerides (MCT) comprise 10% of all lipids in human milk for full term babies and 17% of human milk for preterm infants (Bitman 1983). The absorption of LCT requires pancreatic lipase, mixed micelles, chylomicrons, and carnitine. Since the amounts of pancreatic lipase and bile salts may be limited in early life, lingual and gastric lipases have an important role in hydrolyzing MCT to free fatty acids. This allows for direct gastric and intestinal absorption into the serum without micelles. The medium chain fatty acids are then transported via serum albumin directly to the liver. They may enter the mitochondria for beta oxidation without the help of carnitine (Jensen 1992).
Infant formula is composed of fat in the form of LCT or MCT in varying percentages. The range is from less than 10% of fat as MCT (greater than 90% of fat as LCT) to over 80% of fat as MCT (less than 20% of fat as LCT). For the purposes of this review, high MCT formula contains 40% or more by weight of fat as MCT while low MCT formula contains 20% or less of fat as MCT. The decision to utilize a high or low MCT formula is a difficult one. The significance of LCT lies in a greater resemblance to human milk fatty acids than MCT. Long chain polyunsaturated fatty acids are important in the development of the retina and visual acuity (Carlson 1993, Uauy 1990). However, the long chain polyunsaturated fatty acids make up a small proportion of the total LCT in the majority of preterm formulas. On the other hand, absorption of MCT in the preterm neonate may be easier than LCT due to the alternative route of digestion utilizing lingual and gastric lipases. Thus MCT can act as an easily accessible fuel source, but may also stimulate the production of ketone bodies by the liver (Jensen 1992).
One common clinical way of answering such nutritional value questions is based on growth parameters. Besides growth, issues of adverse outcomes are important. Whether preterm infants may tolerate high or low MCT formula better or have a higher risk of necrotizing enterocolitis (NEC) with high or low MCT formula has not been extensively addressed in the literature. However, several reviews of human and animal research note the easier absorption of MCT for the preterm infant through gastric and lingual lipase which circumvent the more complicated processes LCT must go through to be digested (Bach 1982, Borum 1992, Jensen 1992, Odle 1997). Thus MCT are recommended for malabsorptive processes (Bach 1982, Jensen 1992). An added issue complicating replacement of one type of triglyceride over the other is the slight difference in caloric density, such that MCT is 8.1 kcal/g and LCT is 9.3 kcal/g (Whyte 1986).
This systematic review addressed the question of the effects of high versus low MCT formula on growth, adverse effects, and neurodevelopmental sequelae in the preterm infant. In addition, since MCT is especially useful in preterm infants with underdeveloped digestive systems, the reviewers postulated that subtle differences in weight gain might have been uncovered if infants were to be stratified by birth weight, since lower birth weight infants might utilize MCT to a greater extent. Exclusively formula fed infants were chosen, because exposure to human milk can decrease incidence of NEC and may improve gastrointestinal tolerance, two important possible adverse effects (Lucas 1990, Vohr 1999). Since varying amounts of MCT in formulas exist, the question of whether a particular percentage of MCT in formula affected weight gain was also investigated.
Primary outcomes included increases in head circumference, length, skin fold thickness, and overall rate of weight gain over at least seven days. Secondary outcomes were to include neurodevelopmental assessment and weight gain less than the intrauterine rate (15 gm/kg/d). Incidence of adverse effects defined as gastrointestinal intolerance or NEC were recorded. Two subgroup analyses for effect on weight gain were planned based on stratifying by birth weight and percentage of MCT within formulas.
EXCLUSION: Any history of surgery, major congenital malformations, pre-existing major illnesses (including necrotizing enterocolitis or sepsis), requirement for ventilatory assistance or supplemental oxygen (at the time of enrollment), gestational age greater than or equal to 37 weeks. Studies including infants fed human milk during or before study initiation were excluded since human milk could affect gastrointestinal tolerance and NEC incidence, two important possible adverse effects (Lucas 1990, Vohr 1999).
Secondary outcomes:
• Weight gain less than the intrauterine growth rate, 15 g/kg/d, over
the course of the study
• Neurodevelopmental assessment
• Long term growth
Adverse events assessed over at least one week:
• Gastrointestinal intolerance
• NEC
MEDLINE search including the years 1966 to January, 2002 with the following limitations: human, randomized control trial, infant, English. Search terms included title word=medium chain triglycerides or long chain triglycerides or subject heading=triglycerides. In addition, a search of the Cochrane Controlled Trials Register (The Cochrane Library, Issue 4, 2001), CINAHL (including the years 1982 to January 2002), conference proceedings (American and European Societies for Pediatric Research, 1980-2001; American Dietetic Association, 1989-2001; American Society for Parenteral and Enteral Nutrition, 1985-2001; and North American Society for Pediatric Gastroenterology and Nutrition, 1994-2001) and the articles' bibliographies were done.
Two reviewers separately searched for eligible studies, assessed the quality of each study, and extracted data. The two reviewers together assessed agreement and resolved disagreement by consensus.
Clinical trials were assessed for randomization and the completeness of follow up. Blinding of randomization, blinding of the intervention from the clinical team and researchers, and blinding of the outcome assessment were also evaluated.
Subgroup analysis by birth weight and by percentage of MCT in formulas against rate of weight gain were to be done.
Statistics were to include relative risk and risk difference for categorical outcomes and weighted mean difference for continuous data. A 95% confidence interval was used. The effect and variance estimators from analyses of both periods combined were used for two-period cross-over trials. For meta-analysis, a fixed effect model was used.
Study Eligibility
Nineteen possibly eligible studies were identified. Eight randomized
control trials met inclusion criteria for this review (Hamosh
1989, Hamosh 1991b, Huston
1983, Okamoto 1982, Sulkers
1992, Sulkers 1993a, Whyte
1986, Wu 1993). Three of these were randomized
cross-over trials (Hamosh 1989; Hamosh
1991b; Whyte 1986); the remainder were parallel-group
trials. All eight trials compared short term growth of preterm infants
receiving an exclusive diet of either high or low MCT formula. The percentage
of MCT within the formulas varied from study to study. Data eligible for
the review were extractable from all included studies except Wu
1993.
Eleven studies were excluded. Four studies were excluded because it was not clear that they were randomized (Brooke 1980, Sulkers 1993b, Roy 1975, Van Aerde 1985). Three studies (Bustamante 1987, Spencer 1986, Spencer 1992) were excluded as there were infants in the studies who were exposed to varying amounts of human milk, which could possibly impact on tolerance and incidence of NEC (Lucas 1990, Vohr 1999). Another study (Telliez 1998) was excluded because it studied growth for only three days rather than at least a week. Finally, three studies were excluded because they used MCT formulations which were not high enough to meet our criterion for high MCT (Carnielli 1996, Lucas 1997, Vanderhoof 1999).
Participants
All eight trials described the participants as preterm infants who
were free from disease. Mean gestational ages for the infants included
in the eight trials ranged between 29 and 32 weeks and mean birth weights
ranged from 1.010 kg to 1.476 kg. The average postnatal age of the infants
upon study entry was highly variable between the eight trials and ranged
from one to six weeks. The participants were clearly stated to be AGA infants
in four studies (Hamosh 1989, Hamosh
1991b, Huston 1983, Okamoto
1982). Sulkers 1992 utilized a standard
deviation score (SDS) which subtracts the mean birth weight for gestational
age from the actual birth weight and then divides by one standard deviation
for that gestation (-2.1+/-1.9 MCT vs. -1.9+/-1.5 LCT); this study (Sulkers
1992) includes small for gestation infants (SGA) of unknown number.
The other studies did not mention size for gestational age.
Interventions
There was considerable variability between trials in the percentage
of MCT contained within each formula. It was assumed that MCT+LCT=100%
lipid to determine percentages that were not detailed in certain studies.
When different types of MCT percentages were reported, percentage by weight
was used. Six trials (Hamosh 1989, Hamosh
1991b, Huston 1983, Sulkers
1992, Sulkers 1993a, Whyte
1986) compared short term growth of infants receiving two formulas,
a high MCT (38-50%) and a low MCT (0%-14%) formula. The two studies which
used more than two formulas were Okamoto 1982
(<10%, 40%, 80% MCT) and Wu 1993 (5%, 17%, 30%,
43% MCT). For Okamoto 1982, we used the group
fed the highest percentage MCT formula as the high MCT group in the analyses
comparing high MCT vs low MCT. Hamosh 1991b
and Okamoto 1982 were the only trials that
were unclear if percentages of MCT cited were percentages by weight.
Study duration for the majority of the included trials was about one week of full feeds (Hamosh 1989, Hamosh 1991b, Sulkers 1993a, Whyte 1986, Wu 1993). Two studies included infants on full feeds for greater than one week (Huston 1983, Okamoto 1982). Sulkers 1992 used a study period of about two weeks of full feeds, but weight gain was based on the second week only.
Consent for one protocol was stated as obtained only from parents who had previously made the decision not to breast feed (Whyte 1986). The remainder of the studies did not state that human milk was never part of the infants' diet, but it was assumed that this was the case.
Outcomes
Primary outcomes of interest for meta-analysis were short term growth
parameters, reported in seven studies (Hamosh 1989,
Hamosh
1991b, Huston 1983, Okamoto
1982, Sulkers 1992, Sulkers
1993a, Whyte 1986). Wu
1993 reported starting and ending weights but no growth rates. Analyses
of effects on short term weight gain according to percentage of MCT formula
(grouped by 10 percentage points) compared to high LCT formula were done.
Secondary outcomes of tolerance of formula (emesis, transit time) or incidence
of NEC were described to varying degrees in four studies (Okamoto
1982,
Sulkers 1992, Whyte
1986,
Wu 1993). No studies addressing long term
growth or neurodevelopmental outcomes were located in the search.
Random allocation was claimed in all included studies, but the technique used for sequence generation was not described in any of the studies. Two trials described allocation concealment which in both cases was via opaque envelopes (Huston 1983, Whyte 1986). Short term follow up for all studies was complete, and all babies were accounted for.
Blinding of interventions and outcomes was rarely described. More often, blinding was mentioned, but not clearly how or of whom. Whyte 1986 describes special alphabetical codes for the formula, blinding both the clinical team and investigators of the intervention (outcome blinding is not clear). Hamosh 1989 and Hamosh 1991b mention blinding caretakers but not the methodology involved, and do not mention blinding intervention/outcome from researchers. Okamoto 1982 also refers to the blinding of the clinical team for intervention (without describing the method employed) and then clearly states that the researchers were not blinded (suggesting no blinding of outcomes). Wu 1993 labels the study as "blinded", but does not detail the methods of blinding or whether intervention, outcome, or both were blinded. No description or mention of blinding occurred in the three remaining trials (Huston 1983, Sulkers 1992, Sulkers 1993a).
There were 182 infants from eight randomized trials included in the present analysis of short term growth parameters. Effects on the rate of weight gain were analyzed by high versus low MCT formula and by percentage of MCT. Effects on clinical tolerance and NEC were assessed. Effects on neither neurodevelopmental nor long term growth were assessed in the included studies. Planned subgroup analysis to assess effect on rate of weight gain by birth weight was not done, since only a single study (Whyte 1986) included individual birth weights (but not corresponding individual rates of growth) while the remainder only reported mean birth weights and mean weight gain. The adverse outcome of growth less than or equal to intrauterine growth, 15 g/kg/d, could not be analyzed since all rates of weight gain recorded were greater than 15 g/kg/d. No metabolic data were analyzed as such data were not deemed to be clinically significant to the initial question.
Short term growth parameters
Weight gain (g/kg/d): Five small trials report this outcome (Huston
1983, Okamoto 1982, Sulkers
1992, Sulkers 1993a, Whyte
1986). No individual trial found a statistically significant effect.
The meta-analysis shows no evidence of effect of high MCT formula on weight
gain (WMD -0.35 g/kg/d, 95% CI -1.44, 0.74). There was no evidence of statistical
heterogeneity of treatment effect among these five trials.
Subgroup analysis was done according to %MCT (by 10 percentage point intervals). Three trials assessed effect on weight gain (g/kg/d) of 31-40% MCT formula compared to a low MCT formula (Okamoto 1982, Sulkers 1992, Sulkers 1993a). Two trials assessed the effect on weight gain of 41-50% MCT (Huston 1983 and Whyte 1986). One trial reported the effect on weight gain of a 71-80% MCT formula (Okamoto 1982). None of the individual trials found a statistically significant effect on weight gain and the respective meta-analyses showed no evidence of effect. There was no evidence of statistical heterogeneity of treatment effect within these meta-analyses.
Weight gain (g/d): Two small trials report this outcome (Hamosh 1989, Hamosh 1991b). Of note, Hamosh 1989 reported weight gain once within the text as g/kg/d, but in Table 5 and the abstract, the reported unit of weight gain was g/d. In this review, the unit was assumed to be g/d. Neither trial found a statistically significant effect. The meta-analysis shows no evidence of effect of high MCT formula on weight gain (WMD 2.09 g/d, 95% CI -1.46, 5.64 g/d). There was no evidence of statistical heterogeneity of treatment effect among the two trials.
Length gain (cm/wk): Five small trials report this outcome, using units of either cm/d (Hamosh 1991b, Huston 1983, Whyte 1986) or cm/wk (Okamoto 1982, Sulkers 1992). When length was cited in cm/d, this number was converted to cm/wk by multiplication by seven. No individual trial found a statistically significant effect. The meta-analysis shows no evidence of effect of high MCT formula on length gain (WMD 0.14 cm/wk, 95% CI -0.04, 0.31). There was no evidence of statistical heterogeneity of treatment effect among the five trials.
Head circumference gain (cm/wk): The same small five trials that report length increase also report this outcome (Hamosh 1991b, Huston 1983, Okamoto 1982, Sulkers 1992, Whyte 1986). As with length, head circumference increase is reported in either cm/d or cm/wk (converted here to cm/wk by multiplication by seven). No individual trial found a statistically significant effect. The meta-analysis shows no evidence of effect of high MCT formula on head circumference increase (WMD -0.03 cm/wk, 95% CI -0.15, 0.08). There was no evidence of statistical heterogeneity of treatment effect among these five trials.
Skin fold thickness gain (mm/wk): One small trial assessed this outcome (Okamoto 1982) and did not find a statistically significant effect. The meta-analysis shows no evidence of effect of high MCT formula on skin fold thickness increase (MD -0.15 mm/wk, 95% CI -0.41, 0.11).
Indirect growth measurements: One small trial reports growth indirectly (Wu 1993). This study reports means for starting and ending weights (gm), lengths (cm), head circumferences (cm), and study duration. No measures of variance for any of these data are reported, so the data could not be used in meta-analysis in this review. However, Wu 1993 reported no statistically significant effect on growth of any of four different MCT% formulas.
Gastrointestinal Tolerance
Clinical signs of intolerance: Two small studies report clinical signs
of intolerance (Okamoto 1982, Wu
1993). Okamoto 1982 found that 10 of 11
infants assigned to either 40% or 80% MCT (versus one of 10 infants assigned
to the low MCT formula) demonstrated at least one of the following symptoms:
"tense abdominal distension, loose stools, vomiting, gastric aspirates
that were bilious or contained occult blood". Wu 1993
found that residual aspirates, vomiting, and abdominal distension were
similarly uncommon across the four formulas (5% MCT, 17%, 30%, and 43%MCT).
Of the 60 infants included in Wu 1993, two demonstrated
formula intolerance (one, who was from the lowest percentage of MCT formula
group, was diagnosed with sepsis and NEC; and the second, who was from
the 17% MCT formula group, demonstrated abdominal distension and aspirates).
Stool transit time (hours): One small study reports this outcome (Okamoto 1982). This trial did not find a statistically significant effect. However, a trend of higher mean carmine red transit time for higher MCT formulas (21.6 hours for the control group, 32.1 hours for 40% MCT, and 32.4 hours for 80% MCT formula) was noted.
Fecal output (g/kg/d): One small trial reports this outcome (Sulkers 1992). This trial did not find a statistically significant effect, although fecal output was slightly higher in the low MCT group (2.6+/-0.84 high MCT vs. 3.6+/-1.4 g/kg/d low MCT).
NEC
Case occurrence: Two small trials report the occurrence of NEC (Whyte
1986, Wu 1993). Wu 1993
noted one infant with NEC in the low MCT formula group and Whyte
1986 withdrew one infant for the same reason after enrollment but prior
to study initiation. Based on these small numbers, there appears to be
no evidence of difference in NEC incidence.
Neurodevelopmental assessment
No eligible data were found
Long term growth
No eligible data were found
Data on adverse effects were limited and mostly descriptive in nature. There was no evidence of difference in the incidence of NEC, but an effect may not have been detected given the small numbers of infants enrolled. Although there was no statistically significant difference with either stool transit time or fecal output, there were trends toward higher stool output and faster transit time in the low MCT formula groups. These trends, however, are probably not clinically significant. Furthermore, there does seem to be conflicting evidence regarding tolerance between Okamoto 1982 who found evidence of intolerance for high MCT as opposed to Wu 1993 who found no difference.
Other clinically important outcomes such as neurodevelopmental outcomes or long term growth were not able to be evaluated due to the lack of data on these outcomes. The planned subgroup analysis of weight gain by birth weight was not able to be done. Birth weights were reported individually in one study (Whyte 1986), but not individual weight gain. Effect on poor growth, less than the intrauterine rate of 15 g/kg/d, was also not able to be evaluated since all included trials report mean weight gain above 15 g/kg/d.
All of the eight included trials reported randomized allocation, but none described the sequence generation methods. Only two trials (Huston 1983, Whyte 1986) described allocation concealment which in both cases was by use of opaque, sealed envelopes. In addition, many of the included trials referred to blinding, but did not explain explicitly the methods of blinding or whether intervention or outcome assessment or both were blinded. Although this might not affect objective measures like weight gain to a significant degree, it potentially may have a large impact on clinical ascertainment of tolerance (as one possible explanation for the difference between Okamoto 1982 and Wu 1993). Another methodology issue was the cross over design utilized by several of the studies (Hamosh 1989, Hamosh 1991b, Whyte 1986). Those trials have the potential for the "wash-in/out" phenomenon as they did not explicitly describe a wash-out period between the first and second exposure periods.
There was no evidence of statistical heterogeneity of treatment effect in any of the meta-analyses.
This review has several major limitations. One limitation is that all eight included trials had very small numbers of infants. The small study populations are evidenced by the wide confidence intervals. Such small numbers may not allow high enough power to detect differences in, for example, NEC incidence. Another issue is that the decision to only include studies in English may result in study selection bias and further restrict numbers of infants included.
| Study | Methods | Participants | Interventions | Outcomes | Notes | Allocation concealment |
| Hamosh 1989 | Randomized two-period cross-over design. Sequence generation: can't tell. Allocation concealment: can't tell. Blinding of intervention: for clinical caretakers, yes, for research team, can't tell. Blinding of outcomes: can't tell. Complete follow-up. | Inclusion: AGA and entered when 110-120kcal/k/d of enteral diet. No GI disturbances or disease at time of enrolment. BW=1010+/-71g. GA=28.7+/-0.5wk. PNA=6.08+/-0.81wk. | Enfamil 3242H (HMCT formula): 42%MCT (n=12). Enfamil 3242 (LMCT formula):
7%MCT (n=12).
All fed 130+/-3.58 cc/kg/d. 1 week for each formula. |
Gastric lipolysis, lipase activity, fat absorption, and short term growth. | Weight gain described in g/d in abstract and Table 5 of report (but used gm/kg/d in text). Assumed weight gain was in terms of g/d in this review. Not clear if any parenteral nutrition given. Assume no human milk fed, but not clearly stated. | B |
| Hamosh 1991b | Randomized two-period cross-over design (only first part of study included here). Sequence generation: can't tell. Allocation concealment: can't tell. Blinding of intervention: for clinical caretakers, yes, for research team, can't tell. Blinding of outcomes: can't tell. Complete follow-up. | Inclusion: AGA infants were enrolled once their enteral intake was >/=100kcal/kg/d. No significant GI or other disease at time of study noted. BW=1157+/-110g. GA=29.1+/-0.88wk. PNA=3.13+/-0.71wk. | HMCT formula 50% MCT (n=9).
LMCT formula 14% MCT (n=9). Intake was at least 100kcal/kg/day upon entry. 1 week for each formula. |
Lipase activity in gastric aspirates, fat absorption, fat accretion, and short term growth. | Study#2 was not included in this review since it is a full term formula with LCT (therefore besides different fat, overall different composition, thereby too variable to be included here). It was assumed (but not clearly addressed in study) infants had received no human milk, only formula exclusively. Not clear if infants received parenteral nutrition. Assumed but not clearly stated that percentages of MCT were by weight. | B |
| Huston 1983 | Randomized in parallel design. Sequence generation: can't tell. Allocation concealment: yes (by envelopes). Blinding of intervention: can't tell. Blinding of outcome: can't tell. Complete follow-up. | Inclusion: AGA, BW<1500g, began PO feeding prior to DOL 7. None had requirement of assisted ventilation, congestive heart failure, or developmental abnormalities. BW=1.28+/-0.13 (HMCT), 1.20+/-0.11kg (LMCT). GA=30.4+/-1.4 (HMCT), 29.9+/-1.2wk (LMCT). PNA (at full feeds)=18+/-4 (HMCT), 14+/-2d (LMCT). [BW, GA not significantly different between study groups, but PNA at full feeds was significantly different]. | HMCT formula: 50% MCT (n=10).
LMCT formula: 0% MCT (n=10). Feedings advanced to 150cc/kg/d (120kcal/kg/d). Study period lasted 11d (one week + 4d balance period). |
Absorption and retention of major minerals and nutrients (Ca, PO4, fat, N, Na, 25-OH -D). Short term growth. | All infants received parenteral nutrition with multivitamins, vit D 200 IU, 2% amino acids, 10% or 13% dextrose while below 120 cc/k/d. Parenteral lipids were received by 4 infants on the HMCT formula and 1 infant on LMCT formula. Assumed but not stated that no human milk administered. Two infants withdrawn (1 from each group), 1 with CHF and 1 with GI hypomotility. Significant differences included age of 140cc/kg/d of PO feeds 18+/-4(HMCT) vs. 14+/-2d(LMCT) and age of initiation of balance study 26+/-3d(HMCT) vs. 21+/-2d(LMCT) felt to be due to one infant with persistent lung disease and 2 infants with gastric hypomotility. | A |
| Okamoto 1982 | Randomized in parallel design. Sequence generation: can't tell. Allocation concealment: can't tell. Blinding of intervention: clinical caretakers, yes, research team, no. Blinding of outcome: can't tell. Complete follow-up. | Inclusion: AGA with no illness which could prevent infants from reaching full feeds by 3wk PNA. BW=1476 (LMCT), 1444 (40%MCT), 1478g (80% MCT). GA=31.7 (LMCT), 31.6 (40% MCT), 31.0wk (80% MCT). PNA=12.5 (LMCT), 16.6 (40%MCT), 16.8d (80%MCT). | 80% MCT formula (n=4). 40% MCT formula (n=7). LMCT formula (Similac PM 60/40, some supplemented with taurine of unspecified amounts)=<10%MCT (n=10). Feeds advanced to 120kcal/kg/d. Mean study period= 26.4 (LMCT), 25.7 (40% MCT), 28.8 d (80% MCT) with a range of 12-43d. | GI tolerance to feeds (ie. aspirates), absorption of fat, N, Ca, and Mg, short term growth, and transit time. | Not clear how many infants had the taurine supplement or if this might affect results. Not clear whether or not parenteral nutrition ever given. Human milk not mentioned, but was assumed never to be part of participants' diet. Assumed but not stated that percentages of MCT were in terms of percentage by weight (since molar percentages were also reported). Prior to study, 7 infants had gotten over RDS and 1 of these had required an exchange transfusion for Rh incompatibility. | B |
| Sulkers 1992 | Randomized in parallel design. Sequence generation: can't tell. Allocation concealment: can't tell. Blinding of intervention: can't tell. Blinding of outcome: can't tell. Complete follow-up. | Inclusion: BW<1600gm and no metabolic derangements, congenital abnormalities, or O2 requirement at the time of initiation of feedings. BW=1129+/-218 (HMCT), 1271+/-165g (LMCT). GA=31+/-1.9 (HMCT), 32+/-1.8wk (LMCT). SDS (Standard deviation score) based on actual BW compared to mean BW for GA=-2.1+/-1.9 (HMCT), -1.9+/-1.5 (LMCT). All infants randomized before enteral feeding at PNA 7d. One infant excluded from the LMCT group due to problems with the calorimeter. | HMCT formula 38%MCT (n=15).
LMCT formula 6%MCT (n=12). All received parenteral nutrition for first wk of life, then enteral feeds were started and increased to 150cc/kg/d by PNA 16-19d. Study period was 2 weeks, but weight gain was based on data from one week (fourth week of life). |
N and fat accretion, absorption of Ca, PO4, Mg, serum levels of AP, PTH, and 1,25-(OH)2D, and short term growth. | Since randomized prior to oral feeds, assume no human milk in diet. May have been SGA infants in study, unclear how many. Both formulas contained 4.5g fat/100 ml. | B |
| Sulkers 1993a | Randomized in parallel design. Sequence generation: can't tell. Allocation concealment: can't tell. Blinding of intervention: can't tell. Blinding of outcomes: can't tell. Complete follow-up. | Inclusion: BW<1600g and no metabolic issues, O2 requirement, or congenital anomalies. BW=1.2+/-0.24 (HMCT), 1.2+/-0.16kg (LMCT). GA=31+/-1 (HMCT), 32+/-2wk (LMCT). PNA (reported as median day of study)=22 (HMCT), 24d (LMCT). | HMCT formula 38% MCT (n=9).
LMCT formula 6% MCT (n=9). Feedings started at PNA 7d with a goal of 150 cc/kg/d and metabolic studies occurring at least 3 d later. Exact study period for weight gain was unclear, but appears to be approximately one week (median day of study was 22d for HMCT and 24 for LMCT and metabolic studies occured at 4 weeks of age). |
Glucose metabolism, fat accretion, metabolic rate, and short term growth. | This study is felt to be separate from the Sulkers 1992 study since both the formulas in this study used 6.8g fat/100ml (as opposed to 4.5g/100 in Sulkers 1992). It is not clear whether the infants were on full enteral feeds of at least one week prior to end of study. Whether or not the infants received parenteral nutrition or human milk is not detailed, but assumed no human milk. | B |
| Whyte 1986 | Randomized two-period cross-over design. Sequence generation: can't tell. Allocation concealment: yes (by envelopes). Blinding of intervention: yes (both clinical caretakers and research team). Blinding of outcomes: can't tell. Complete follow-up. | Inclusion: Birth weight (BW) <1800gm, age<2wks, consistent weight gain 3d prior to study, parental decision against human milk diet, and no disease requiring O2, ventilatory support, or IV therapy. BW=1.38+/-0.34kg. GA=31+/-2wk. PNA=15+/-4d. (N=15) | Formula A (HMCT): 46%MCT (n=15).
Formula B (LMCT): 4%MCT (n=15). Intake was 150 cc/kg/d. Each study period was 5 d of formula followed by 3 d balance period. |
Energy and nitrogen balance, coefficients of digestibility and metabolizability, and short term growth. | Parenteral nutrition not mentioned. 1 infant stopped due to NEC and 5 had incomplete balance data (therefore only 15 described in study). Prior to study initiation, all infants fed Special Care Infant Formula for 3d. | A |
| Wu 1993 | Randomized in parallel design. Sequence generation: can't tell. Allocation concealment: can't tell. Blinding of intervention: can't tell. Blinding of outcome: can't tell. (This study was "blinded" but did not describe how, of what, or of whom.) Complete follow-up. | Inclusion: BW </=1500gm, normal serum albumin, and no PO feeds prior to study initiation, major congenital anomalies, surgery, sepsis, blood group incompatability, neurological disease, or metabolic derangement. BW=1240+/-60 (5% MCT), 1220+/-40 (17% MCT), 1200+/-50 (30% MCT), 1250+/-60 g (43%MCT). GA=31+/-1 (5% MCT), 30+/-1 (17% MCT), 31+/-1 (30% MCT), 31+/-1 wk (43% MCT), PNA=5.9+/-1.8 (5% MCT), 6.3+/-1.8 (17% MCT), 4.7+/-1.2 (30% MCT), 5.7+/-1.7d(43% MCT). | 43% MCT (n=15), 30% MCT (n=14), 17% MCT (n=15), 5% MCT (n=16). Balance studies x2d when first 9-12 infants per formula had reached at least 100 kcal/kg/d. Mean duration of study period 18-22d, but mean time in study on full feeds was one week (7.0+/-0, 5%MCT; 6.8+/-0.1, 17%MCT; 6.6+/-0.2, 30%MCT; 6.9+/-0.1d, 43%MCT). | Short term growth, GI intolerance (ie. emesis), fat absorption, ketogenesis (or the presence of ketone bodies), serum glucose and carnitine levels. | Data on growth not reported in a form which permits use in meta-analysis in this review. Carnitine and taurine added to all formulas. Infants only received a formula diet, but parenteral nutrition not mentioned. Since randomized prior to enteral feeds, assumed no use of any human milk in diet. 4 infants left study unrelated to formula intolerance. 2 of 60 did have formula intolerance (1 from 5%MCT with sepsis and NEC, 1 from 17% MCT with abdominal distension and aspirates). | B |
| Study | Reason for exclusion |
| Brooke 1980 | No randomization. |
| Bustamante 1987 | This study used human milk to initiate enteral feeding. Although once the study was started the infants were fed exclusively formula, the human milk may affect NEC incidence or tolerance. |
| Carnielli 1996 | The high MCT formula in this study is 34.1% by weight (47.1 mol%) and is therefore not high enough to reach the 40% by weight cut-off for high MCT used in this review. |
| Lucas 1997 | This is a comparison of different types of LCT based formulas. None of the three formulas used contain MCT concentrations (3%, 6%, and 3%) high enough to meet the 40% by weight cut-off for high MCT used in this review. |
| Roy 1975 | No mention of randomization. |
| Spencer 1986 | Some infants had been fed human milk prior to study. This might affect NEC incidence as well as tolerance. |
| Spencer 1992 | Throughout the study babies were also able to have human milk. Although only the weeks in which infants were fed exclusively their pre-assigned formula were used for analysis (i.e. excluding times when infants were exclusively or partially fed human milk), the results for NEC incidence and tolerance may be significantly impacted. |
| Sulkers 1993b | No mention of randomization. |
| Telliez 1998 | Weight gain recorded over only 3 days. |
| Van Aerde 1985 | No mention of randomization. |
| Vanderhoof 1999 | This study looked at a long chain polyunsaturated fatty acid supplemented formula vs. control without polyunsaturated fatty acid supplementation or human milk. Neither of the two formulas used have MCT concentrations (14% in both) which qualify for the high MCT criterion (at least 40% by weight) used in this review. |
Hamosh M, Bitman J, Liao T, et al. Gastric lipolysis and fat absorption in preterm infants: Effect of medium-chain triglyceride or long-chain triglyceride-containing formulas. Pediatrics 1989;83:86-92.
Hamosh 1991b {published data only}
Hamosh M, Mehta NR, Fink CS, et al. Fat absorption in premature infants: Medium-chain triglycerides and long-chain triglycerides are absorbed from formula at similar rates. J Pediatr Gastroenterol Nutr 1991;13:143-149.
Huston 1983 {published data only}
Huston RK, Reynolds JW, Jensen C, et al. Nutrient and mineral retention and Vitamin D absorption in low-birth-weight infants: Effect of medium-chain triglycerides. Pediatrics 1983;72:44-48.
Okamoto 1982 {published data only}
Okamoto E, Muttart CR, Zucker CL, et al. Use of medium-chain triglycerides in feeding the low-birth-weight infant. Am J Dis Child 1982;136:428-431.
Sulkers 1992 {published data only}
* Sulkers EJ, Van Goudoever JB, Leunisse C, et al. Comparison of two preterm formulas with or without addition of medium-chain triglycerides (MCTs). I: Effects on nitrogen and fat balance and body composition changes. J Pediatr Gastroenterol Nutr 1992;15:34-41.
Sulkers EJ, Lafeber HN, Degenhart HJ, et al. Comparison of two preterm formulas with or without addition of medium-chain triglycerides (MCTs). II: Effects on mineral balance. J Pediatr Gastroenterol Nutr 1992;15:42-47.
Sulkers 1993a {published data only}
Sulkers EJ, Lafeber HN, Van Goudoever JB, et al. Decreased glucose oxidation in preterm infants fed a formula containing medium-chain triglycerides. Pediatr Res 1993;33:101-105.
Whyte 1986 {published data only}
Whyte RK, Campbell D, Stanhope R, et al. Energy balance in low birth weight infants fed formula of high or low medium-chain triglyceride content. J Pediatr 1986;108:964-971.
Wu PY, Edmond J, Morrow JW, et al. Gastrointestinal tolerance, fat absorption, plasma ketone and urinary dicarboxylic acid levels in low-birth-weight infants fed different amounts of medium-chain triglycerides in formula. J Pediatr Gastroenterol Nutr 1993;17:145-152.
Brooke OG. Energy balance and metabolic rate in preterm infants fed with standard and high-energy formulas. Br J Nutr 1980;44:13-23.
Bustamante 1987 {published data only}
Bustamante SA, Fiello A, Pollack PF. Growth of premature infants fed formulas with 10%, 30%, or 50% medium-chain triglycerides. Am J Dis Child 1987;141:516-519.
Carnielli 1996 {published data only}
Carnielli VP, Rossi K, Badon T, et al. Medium-chain triacylglycerols in formulas for preterm infants: Effect on plasma lipids, circulating concentrations of medium-chain fatty acids, and essential fatty acids. Am J Clin Nutr 1996;64:152-158.
Lucas 1997 {published data only}
Lucas A, Quinlan P, Abrams S, et al. Randomised controlled trial of a synthetic triglyceride milk formula for preterm infants. Arch Dis Child 1997;77:F178-184.
Roy 1975 {published data only}
Roy CC, Ste-Marie M, Chartrand L, et al. Correction of the malabsorbtion of the preterm infant with a medium-chain triglyceride formula. J Pediatr 1975;86:446-450.
Spencer 1986 {published data only}
Spencer SA, Stammers JP, Hull D. Evaluation of a special low birth weight formula, with and without medium chain triacylglycerols. Early Hum Dev 1986;13:87-95.
Spencer 1992 {published data only}
Spencer SA, McKenna S, Stammers J, et al. Two different low birth weight formulae compared. Early Hum Dev 1992;30:21-31.
Sulkers 1993b {published data only}
Sulkers EJ, Van Goudoever JB, Carnielli VP, et al. Influence of medium-chain triglycerides (MCT) on fat balance and growth in extremely low birth weight (ELBW) infants. Pediatr Res 1993;33:311A.
Telliez 1998 {published data only}
Telliez F, Bach V, Dewasmes G, et al. Effects of medium- and long-chain triglycerides on sleep and thermoregulatory processes in neonates. J Sleep Res 1998;7:31-39.
Van Aerde 1985 {published data only}
Van Aerde J, Sauer P, Heim T, et al. The effect of diet composition on energy metabolism, substrate utilisation and growth in the VLBW infant (abstract). Pediatr Res 1985;19:1085.
Vanderhoof 1999 {published data only}
Vanderhoof J, Gross S, Hegyi T, et al. Evaluation of a long-chain polyunsaturated fatty acid supplemented formula on growth, tolerance, and plasma lipids in preterm infants up to 48 weeks postconceptional age. J Pediatr Gastroenterol Nutr 1999;29:318-326.
* indicates the primary reference for the study
Bach AC, Babayan VK. Medium-chain triglycerides: An update. Am J Clin Nutr 1982;36:950-962.
Bitman J, Wood L, Hamosh M, et al. Comparison of the lipid composition of breast milk from mothers of term and preterm infants. J Clin Nutr 1983;38:300-312.
Borum PR. Medium-chain triglycerides in formula for preterm neonates: Implications for hepatic and extrahepatic metabolism. J Pediatr 1992;120:S139-145.
Carlson SE, Werkman SH, Rhodes PG, et al. Visual-acuity development in healthy preterm infants: effect of marine-oil supplementation. Am J Clin Nutr 1993;58:35-42.
Ehrenkranz RA, Younes N, Lemons JA, et al. Longitudinal growth of hospitalized very low birth weight infants. Pediatrics 1999;104:280-289.
Hack M, Breslau N, Weissman B, et al. Effect of very low birth weight and subnormal head size on cognitive abilities at school age. N Engl J Med 1991;325:231-237.
Hamosh, M. Lipid metabolism. In: Hay, WW, editor(s). Neonatal Nutrition and Metabolism. St. Louis: Mosby Year Book, Inc., 1991:122-142.
Jensen GL, Jensen RG. Specialty lipids for infant nutrition. II. Concerns, new developments, and future applications. J Pediatr Gastroenterol Nutr 1992;15:382-394.
Kuschel CA, Harding JE. Fat supplementation of human milk for promoting growth in preterm infants (Cochrane Review). In: The Cochrane Library, Issue 4, 1999. Oxford: Update Software.
Lucas A, Cole TJ. Breast milk and neonatal necrotising enterocolitis. Lancet 1990;336:1519-1523.
Lucas A, Morley R, Cole TJ. Randomised trial of early diet in preterm babies and later intelligence quotient. BMJ 1998;317:1481-1487.
Odle J. New insights into the utilization of medium-chain triglycerides by the neonate: Observations from a piglet model.. J Nutr 1997;127:1061-1067.
Pereira GR, Baumgart S, Bennett MJ, et al. Use of high-fat formula for premature infants with bronchopulmonary dysplasia: Metabolic, pulmonary, and nutritional studies. J Pediatr 1994;124:605-611.
Uauy RD, Birch DG, Birch EE, et al. Effect of dietary omega-3 fatty acids on retinal function of very-low-birth-weight neonates. Pediatr Res 1990;28:485-492.
Vohr BR, Bier JB, McKinley L. Human milk and health outcomes: Infancy and later. In: Human Milk for Very-Low-Birth-Weight Infants. Report of the 108th Ross Conference on Pediatric Research. Columbus: Ross Products Division, Abbott Laboratories, 1999:185-199.