Caffeine may be able to prevent postoperative apnea and bradycardia in preterm babies. Growing babies who were born too early (preterm) and who undergo general anaesthetic for surgery may have complications, including episodes of apnea (pauses in breathing), cyanosis (from lack of oxygen in the blood), and bradycardia (slow heartbeat). Caffeine, which is a methylxanthine drug, is thought to stimulate breathing, and so possibly prevent apnea and subsequent problems. The review found some evidence that caffeine given at the time of surgery reduces apnea, bradycardia, and cyanosis after anaesthetic, but the importance of this is unclear.
Growing ex-preterm infants who undergo general anesthesia for surgery at about term-equivalent age may have episodes of apnea, cyanosis and bradycardia during the early postoperative period. A breathing stimulant such as caffeine, given at the time of operation, might prevent these episodes.
In ex-preterm infants who undergo general anesthesia for surgery, does the prophylactic use of caffeine prevent episodes of apnea, cyanosis and bradycardia during the postoperative period without clinically important side effects?
The standard strategy of the Neonatal Review Group was used. This included searches of the Oxford Database of Perinatal Trials, MEDLINE (1966 - January 2004), EMBASE 1980 - January 2004), CINAHL (1982 - January 2004) and the Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library, Issue 4, 2003. Search terms included text words 'apnea', 'caffeine' and MeSH heading 'infant, premature'. Searches were also made of previous reviews including cross references. Abstracts of the Society for Pediatric Research were hand searched for the years 1996 - 2003 inclusive.
All trials utilising random or quasi-random patient allocation, in which treatment was compared with placebo or no treatment, were included.
The standard methods of the Cochrane Collaboration and its Neonatal Review Group were used to select trials, evaluate quality and to extract data. The methodological quality of each trial was reviewed by the second author blinded to trial authors and institution(s). Each author extracted data separately, compared and resolved differences. Meta-analysis used relative risk and risk difference.
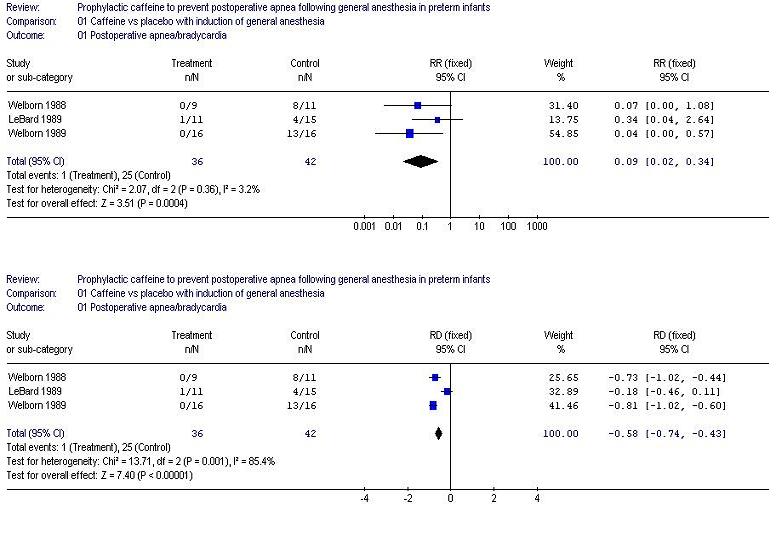
Three eligible trials were found. In each trial apnea/bradycardia occurred in fewer treated than control infants. The typical estimate for relative risk is 0.09 (0.02, 0.34). The typical estimate for absolute risk difference is minus 0.58 (-0.74, -0.43) indicating that fewer than two infants have to be treated with caffeine to expect to prevent one with postoperative apnea. In two trials (Welborn 1989, LeBard 1989) continuous recordings of oxygen saturation detected hypoxaemic episodes (<90 %) in fewer treatment than control infants [RR 0.13 (0.03, 0.63]. No infant in any trial required intubation and mechanical ventilation. No adverse effects were reported.
Implications for practice. Caffeine can be used to prevent postoperative apnea/bradycardia and episodes of oxygen desaturation in growing preterm infants if this is deemed clinically necessary. In view of the small numbers of infants studied in these trials and uncertainty concerning the clinical significance of the episodes, caution is warranted in applying these results to routine clinical practice.
Implications for research. There is a need to determine which infants might benefit most by this treatment. Studies confined to those most at risk of apnea (prior history, younger postmenstrual age) and those that might require mechanical ventilation (chronic lung disease) would be of value.
Growing ex-preterm infants who undergo general anesthesia for surgery at about term equivalent age may have episodes of apnea, cyanosis and bradycardia during the early postoperative period.
The American Academy of Pediatrics defined infant apnea as a pause in breathing of greater than 20 seconds, or one of less than 20 seconds and associated with bradycardia and/or cyanosis (AAP 2003). Recurrent episodes of apnea are common in preterm infants and the incidence and severity increases at lower gestational ages. By term equivalent age infants have usually 'outgrown' their tendency to spontaneous apnea. However, if some additional insult such as infection, or the administration of drugs that depress the central nervous system occurs (such as general anesthetic agents, Liu 1983), apnea and associated oxygen desaturations can recur. Attempts have been made to determine which infants are most at risk (Spear 1992, Welborn 1994, Cote 1995). Factors such as younger postmenstrual age and past history of apnea seem important, although such risk scoring does not detect all infants who develop postanesthesia problems (Cote 1995).
If prolonged, apnea can lead to hypoxemia and reflex bradycardia which may require active resuscitative efforts to reverse. There are clinical concerns that these episodes might be harmful to the developing brain or cause dysfunction of the gut or other organs, although there are no data to support this. Frequent episodes may be accompanied by respiratory failure of sufficient severity as to lead to intubation and the use of intermittent positive pressure ventilation (IPPV).
Methylxanthines such as caffeine are thought to stimulate breathing efforts and have been used in clinical practice to reduce apnea in preterm infants since the late 1970's. The mechanism of their action is not certain. Possibilities include increased chemoreceptor responsiveness (based on increased breathing responses to CO2), enhanced respiratory muscle performance and generalised central nervous system excitation. Other reviews on the effects of methylxanthines such as caffeine on apnea, published in the Cochrane Library, include Henderson-Smart a, Henderson-Smart b, Henderson-Smart c and Henderson-Smart d. A systematic review has also been carried out on the effects of regional versus general anesthesia on postoperative apnea (Craven 2003).
In ex-preterm infants who undergo general anesthesia for surgery, does the prophylactic use of caffeine prevent episodes of apnea, cyanosis and bradycardia during the postoperative period without clinically important side effects?
All trials utilising random or quasi-random patient allocation.
Preterm infants undergoing general anesthesia for surgery at about term equivalent age.
Caffeine given with general anesthesia, compared with control, as prophylaxis for postoperative apnea.
1. Episodes of apnea and bradycardia consistent with clinical apnea (AAP 2003).
2. Episodes of oxygen desaturation (>10% fall)
3. Use of IPPV
4. Side effects
The standard strategy of the Neonatal Review Group was used. This included searches of the Oxford Database of Perinatal Trials, MEDLINE (1966 - January 2004), EMBASE 1980 - January 2004), CINAHL (1982 - January 2004) and the Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library, Issue 4, 2003. Search terms included text words 'apnea', 'caffeine' and MeSH heading 'infant, premature'. Searches were also made of previous reviews including cross references. Abstracts of the Society for Pediatric Research were hand searched for the years 1996 - 2003 inclusive.
The standard methods of the Cochrane Collaboration and its Neonatal Review Group were used to select trials, evaluate quality and to extract data. The methodological quality of each trial was reviewed by the second author blinded to trial authors and institution(s). Each author extracted data separately, compared and resolved differences.
Meta-analysis used the fixed effects model and were displayed as relative risk (RR), risk difference (RD) and number needed to treat which was calculated from 1/RD). The 95% confidence intervals are given in brackets after the point estimate to indicate precision.
Three eligible trials were found. Details are given in the table of included studies. In general, infants were born at 30-32 weeks gestation and studied at 40-44 weeks post-menstrual age. All three trials evaluated caffeine given intravenously in a single dose during general anesthesia. The dosage varied from 5 mg/kg (Welborn 1988) to 10 mg/kg (Welborn 1989, LeBard 1989). In all three trials apnea was defined as any apneic episodes of >15 seconds duration, or shorter ones associated with bradycardia. In two trials, oxygen desaturations (<90%) on pulse oximetry were recorded (Welborn 1989, LeBard 1989).
This is detailed in the table of included studies.
Concealment at randomisation: all used formal randomisation although
the steps taken to fully conceal allocation assignment were not clear.
Blinding of treatment: in each trial a saline placebo was used.
Blinding of outcome assessment: in 2 trials apnea/bradycardia was assessed blindly from a polygraphic recording. Methodology in the third trial (LeBard 1989) needs clarification as this has only been published in abstract form.
Completeness of follow up: not clearly stated.
Three eligible trials were found. In each trial apnea/bradycardia occurred in fewer treated than control infants. The typical estimate for relative risk is 0.09 (0.02, 0.34). Absolute risk difference is minus 0.58 (-0.74, -0.43) indicating that fewer than two infants have to be treated with caffeine to expect to prevent one with postoperative apnea. In two trials (Welborn 1989, LeBard 1989) continuous recordings of oxygen saturation detected hypoxaemic episodes (<90 %) in fewer treatment than control infants [RR 0.13 (0.03, 0.63]. No infant in any trial required intubation and mechanical ventilation. No adverse effects were reported.
Caffeine reduces the occurrence of apnea, bradycardia and oxygen desaturation after general anesthesia, although it has yet to be determined whether these episodes are clinically important. If such episodes are detected by monitors, responded to promptly by nurses and do not lead to a need for mechanical ventilation, then they are of uncertain significance. Apnea and hypoxemia might be more important in infants at particularly high risk of respiratory failure, such as those with chronic lung disease. This has not been evaluated.
One study (Welborn 1990 ) has suggested that apnea is more common following general anesthesia than following spinal anesthesia without premedication in infants having inguinal hernia repair, one of the most common operative procedures in ex-preterm infants. A recent Cochrane Review (Craven 2003) did not find evidence to support that hypothesis.
No adverse effects were reported, although the number of infants studied in these three trials is too small to exclude less common ones.
Caffeine can be used to prevent postoperative apnea/bradycardia and episodes of oxygen desaturation in preterm infants if this is deemed clinically necessary. In view of the small numbers of infants studied in these trials and uncertainty concerning the clinical significance of the episodes, caution is warranted in applying these results to routine clinical practice.
There is a need to determine which infants might benefit most by this treatment. Studies confined to those most at risk of apnea (prior history, younger postmenstrual age) and those that might require mechanical ventilation (chronic lung disease) would be of value.
| Study | Methods | Participants | Interventions | Outcomes | Notes | Allocation concealment |
| LeBard 1989 | Randomisation method not specified, blinded treatment, blinding of assessment and exclusions not specified. | Preterm infants undergoing general anesthesia. | Caffeine 10 mg/kg vs saline placebo IV after induction of anesthesia. | Apnea > 15 sec or with bradycardia < 80 bpm, oxygen desaturations <90% on pulse oximetry. | Abstract only available. | B |
| Welborn 1988 | Randomly assigned by pharmacy, double blind, blind assessment of continuous recordings of apnea/bradycardia, no exclusions mentioned. | Preterm (<38 weeks
gestational age) undergoing general anesthesia for inguinal hernia repair
at 35 - 44 weeks post menstrual age. Infants ineligible if existing cardiac,
neurological or metabolic disease. | Caffeine 5 mg/kg vs saline placebo IV with induction of anesthesia. | Apnea >15 sec and/or bradycardia <100 bmp for 5 sec. | A | |
| Welborn 1989 | Randomly assigned by pharmacy, double blind, blind assessment of continuous recordings of apnea/bradycardia, no exclusions mentioned. | Preterm (<38 weeks gestational age) undergoing general anesthesia for inguinal hernia repair at 35 - 44 weeks post menstrual age. Infants ineligible if existing cardiac, neurological or metabolic disease. | Caffeine 10 mg/kg vs saline placebo IV with induction of anesthesia. | Apnea >15 sec and/or bradycardia <100 bmp for 5 sec, oxygen desaturation <90% during 12 hours post anesthesia. | A |
LeBard SE, Kurth CD, Spitzer AR, Downes JJ. Preventing postoperative apnea by neuromodulator antagonists. Anesthesiology 1989;71:A1026.
Welborn 1988 {published data only}
Welborn LG, De Soto H, Hannallah RS, Fink R, Ruttimann UE, Boeckx R. The use of caffeine in the control of post-anesthetic apnea in former premature infants. Anesthesiology 1988;68:796-8.
Welborn 1989 {published data only}
Welborn LG, Hannallah RS, Fink R, Ruttimann UE, Hicks JM. High-dose caffeine suppresses postoperative apnea in former preterm infants. Anesthesiology 1989;71:347-9.
* indicates the primary reference for the study
American Academy of Pediatrics. Policy statement. Apnea, Sudden Infant Death Syndrome, and home monitoring. Pediatrics 2003;111:914-17.
Cote CJ, Zaslavsky A, Downes JJ, Kurth CD, Welborn LG, Warner LO, Malviya SV. Postoperative apnea in former preterm infants after inguinal herniorrhaphy. Anesthesiology 1995;82:809-22.
Craven PD, Badawi N, Henderson-Smart DJ, O'Brien M. Regional (spinal, epidural, caudal) versus general anaesthesia in preterm infants undergoing inguinal herniorrhaphy in early infancy (Cochrane Review). In: The Cochrane Library, Issue 4, 2003. Oxford: Update Software.
Henderson-Smart DJ , Steer P. Methylxanthine treatment for apnea in preterm infants (Cochrane Review). In: The Cochrane Library, Issue 4, 2003. Oxford: Update software.
Henderson-Smart DJ, Davis PG. Prophylactic methylxanthine for extubation in preterm infants (Cochrane Review). In: The Cochrane Library, Issue 4, 2003. Oxford: Update Software.
Henderson-Smart DJ, Steer PA. Prophylactic methylxanthine for preventing of apnea in preterm infants (Cochrane Review). In: The Cochrane Library, Issue 4, 2003. Oxford: Update Software.
Henderson-Smart DJ, Steer PA. Caffeine versus theophylline for apnea in preterm infants (Cochrane Review). In: The Cochrane Library, Issue 4, 2003. Oxford: Update Software.
Liu LM, Cote CJ, Goudsouzian NG, Ryan JF, Firestone S, Dedrick DF, Liu PL, Todres ID. Life-threatening apnea in infants recovering from anesthesia. Anesthesiology 1983;59:506-10.
Spear RM. Anesthesia for premature and term infants: perioperative complications. Journal of Pediatrics 1992;120:165-76.
Welborn LG, Rice LJ, Hannallah RS, Broadman LM, Ruttimann UE, Fink R. Postoperative apnea in former preterm infants: prospective comparison of spinal and general anesthesia. Anesthesiology 1990;72:838-42.
Welborn LG, Greenspun JC. Anesthesia and apnea. Perioperative considerations in the former preterm infant. Pediatr Clin North Amer 1994;41:181-98.
Henderson-Smart DJ, Steer PA. Prophylactic caffeine to prevent postoperative apnea in preterm infants (Cochrane Review). In: The Cochrane Library, Issue 2, 2001. Oxford: Update Software.
01.01 Postoperative apnea/bradycardia
01.02 Postoperative oxygen desaturations
| Comparison or outcome | Studies | Participants | Statistical method | Effect size |
|---|---|---|---|---|
| 01 Caffeine vs placebo with induction of general anesthesia | ||||
| 01 Postoperative apnea/bradycardia | 3 | 78 | RR (fixed), 95% CI | 0.09 [0.02, 0.34] |
| 02 Postoperative oxygen desaturations | 2 | 58 | RR (fixed), 95% CI | 0.13 [0.03, 0.63] |
| This review is published as a Cochrane review in The
Cochrane Library 2004, Issue 3, 2004 (see www.CochraneLibrary.net for information).
Cochrane reviews are regularly updated as new evidence emerges and in response
to comments and criticisms, and The Cochrane Library should be consulted
for the most recent version of the Review. |
{kind=link}
{kind=link}