Systemic fungal infection accounts for about 10% of all cases of sepsis diagnosed in infants more than 72 hours old. The estimated attributable mortality is about 25%, much higher than that associated with invasive bacterial infection (Stoll 1996, Saiman 2000, Makhoul 2002, Stoll 2002). Systemic fungal infection is also associated with increased short and long term morbidity in preterm infants. In particular, fungal infection of the central nervous system has a significant impact on long term neurodevelopmental outcome (Friedman 2000).
The clinical presentation of invasive fungal and bacterial infection is similar, and this may lead to a delay in diagnosis and treatment. In addition to fungaemia, infants may present with pneumonia, meningitis, renal tract infection, ophthalmitis, osteomyelitis, endocarditis, liver abscesses, and skin abscesses. The diagnosis may be further delayed due to an inability to consistently recover the organism from blood, cerebro-spinal fluid, or urine. A high index of suspicion and the use of additional laboratory and clinical tests, including retinal examination, echocardiography, and renal ultrasonography, may be needed to confirm the suspected diagnosis. Given the high mortality and difficulty in establishing an early diagnosis, systemic antifungal therapy is often given prior to the establishment of a confirmed diagnosis. In some centres, prophylactic antifungal therapy is given to preterm infants at high risk of invasive fungal infection. The evidence of effect of this practice has been evaluated in other Cochrane reviews (Austin 2002, McGuire 2002).
A number of antifungal drugs are available for treating preterm infants with invasive fungal infection. Prescribing practice varies between neonatal units (Rowen 1998). The most commonly used drug is amphotericin B, a polyene antifungal agent that reacts with sterols in cell membranes to cause cell lysis. Amphotericin B is poorly absorbed via the enteral route and is only available as an intravenous preparation. Drug toxicity, particularly nephrotoxicity, is a significant problem as amphotericin B also damages mammalian cell membranes. These adverse effects limit the total dose that may be given. The newer lipid complex formulations of amphotericin B deliver the active drug directly to the site of action on the fungal cell membrane. Because the lipid complex is more stable in mammalian cells, toxicity is reduced. Consequently, amphotericin B lipid complex can be given at higher total doses. There is good evidence of reduced nephrotoxicity with the lipid complex formulations compared with conventional amphotericin B in some groups of patients, for example, cancer patients with neutropaenia (Johansen 2002a). There are also some observational data to suggest less toxicity in preterm infants (Weitkamp 1998, Juster-Reicher 2000, Adler-Shohet 2001). However, the lipid complex formulations are very much more expensive than conventional amphotericin B. In current neonatal practice use is often restricted to infants who are intolerant of, or do not respond to, conventional amphotericin B (Rowen 1998).
Amphotericin B is highly protein bound and does not achieve good penetration into extra-cellular fluid spaces, including cerebro-spinal fluid. Another drug is often used instead of, or in addition to, amphotericin B to treat preterm infants with suspected or confirmed fungal meningitis (Rowen 1998). The most commonly used additional agent is 5-fluorocytosine (flucytosine), a fluorinated pyrimidine anti-metabolite that competitively inhibits nucleic acid synthesis. 5-fluorocytosine achieves very good penetration into the cerebro-spinal fluid (Hill 1974). Since monotherapy is thought to increase the risk of the development of stable antifungal resistance, 5-fluorocytosine is usually prescribed with amphotericin B or another antifungal agent. Amphotericin B and 5-fluorocytosine are not antagonistic, but the evidence for synergism is inconsistent, and depends on the laboratory assessment method used (Keele 2001, Te Dorsthorst 2002). 5-fluorocytosine is very well absorbed via the enteral route. Oral and intravenous preparations are available. The known side effects of 5-fluorocytosine include hepatic toxicity and transient neutropaenia, although more significant bone marrow suppression has also been reported (Vermes 2000).
The other major class of antifungal agents available for treating preterm infants with invasive fungal infection is the azole group of drugs. These include the triazoles (fluconazole, itraconazole) and the imidazoles (miconazole, ketoconazole). These drugs bind preferentially to the fungal cytochromes P450 and interfere with ergosterol synthesis in the cell membrane. There are two potential advantages of using an azole drug compared with amphotericin B. The first advantage is that the azoles are well absorbed after enteral administration. A prolonged treatment course can therefore be given without the presence of an intravenous catheter, a potential risk factor for invasive fungal infection (Saiman 2000). Secondly, evidence from systematic reviews of randomised controlled trials in adult populations suggests that the azole drugs are less toxic than conventional amphotericin B (Kontoyiannis 2001, Johansen 2002b). However, these findings may have been biased by methodological flaws in some of the included trials.
There appears to be limited experience with the systemic use of imidazole drugs in preterm infants, although there are reports of apparent treatment success (Tuck 1980, Hensey 1982), and of apparent treatment failure (McDougall 1982). However, the triazoles, particularly fluconazole, are increasingly used in neonatal practice (Rowen 1998). Fluconazole has appeared to be a safe treatment for preterm infants with invasive fungal infection, including fungal meningitis. The only relatively common side effect is mild and transient elevation of plasma levels of creatinine or hepatic enzymes, described in about 5% of preterm infants treated with fluconazole (Huttova 1998). There are, however, rare important side effects, such as Stevens-Johnson syndrome, reported in other populations of patients (Gussenhoven 1991). Additionally, as highlighted by other authors (Neely 2001), there is a potential risk of adverse effects as a result of drug interactions with medications that are prescribed for preterm infants, including cisapride, theophylline, and thiazide diuretics.
A major consideration with antimicrobial drug use is the potential for the emergence of stable resistance to the antimicrobial agent. Some species of fungi, for example Candida glabrata or Candida krusei, are intrinsically resistant to fluconazole (Rogers 1995). There has been some concern, although not any definite evidence, that fluconazole is poorer than amphotericin B in eradicating these non-albicans Candida species in adults (Kontoyiannis 2001). The potential clinical consequences at the population level of altering the pattern of antifungal resistance must be considered. However, these consequences are difficult to define in controlled trials that do not use a neonatal nursery/unit/centre as the unit of randomisation.
Given the potential for the choice of systemic antifungal therapy to affect outcomes for preterm infants with invasive fungal infection, we reviewed the available evidence to determine if there are any implications for current practice or for future research.
We planned to examine the following intervention comparisons:
1. Amphotericin B lipid complex versus amphotericin B. We intended to undertake subgroup analyses of the individual lipid complex formulations (for example, "AmBisome", "Abelcet", "Amphocil").
2. Azole antifungal agents versus amphotericin B (including amphotericin
B lipid complex). We intended to undertake subgroup analyses of:
(a) the individual azole drugs (fluconazole, itraconazole, ketoconazole,
miconazole)
(b) conventional and lipid formulations of amphotericin B
3. Amphotericin B plus 5-fluorocytosine versus amphotericin B alone. We intended to undertake subgroup analyses of the trials that only included infants treated for confirmed or suspected fungal meningitis.
For all of the above, we intended to undertake subgroup analyses of trials that specifically recruited only infants with confirmed invasive fungal infection (defined in types of participants).
2. Cluster randomised trials, where the unit of randomisation is the neonatal nursery/unit/centre.
We defined "confirmed" invasive fungal infection as:
a. culture of fungus from a sterile site- cerebrospinal fluid, blood, urine,
bone or joint, peritoneum, pleural space. Blood cultures should have been
obtained from peripheral sites, not from indwelling catheters. Urine samples
should have been obtained from sterile urethral catheterisation or suprapubic
aspiration of the bladder, not from indwelling catheters or from urine "bag"
samples (since organisms isolated from these may represent perineal contamination).
b. findings on ophthalmological examination consistent with fungal ophthalmitis
or retinitis
c. pathognomonic findings on renal ultrasound examination: "renal fungal
balls"
We defined "suspected" invasive fungal infection pragmatically as an individual clinician's choice to prescribe a systemic antifungal agent based on the clinical suspicion of invasive fungal infection, but in the absence of a confirmed diagnosis as described above.
We did not include trials of antifungal prophylaxis, or trials where systemic antifungal therapy is given to treat superficial mucosal or skin infection.
1. Amphotericin B
2. Amphotericin B lipid complex formulations (for example, "AmBisome", "Abelcet",
"Amphocil").
3. Azole antifungal agents (for example, fluconazole, itraconazole, ketoconazole,
miconazole)
4. Amphotericin B plus 5-fluorocytosine
Primary outcomes:
1. Death (all cause) prior to hospital discharge. We did not use death attributed
to fungal infection as an outcome measure, as this information may be unreliable
and prone to bias.
2. Neurodevelopmental outcomes during infancy and beyond using validated
assessment tools such as Bayley Scales of Infant Development, and classifications
of disability, including auditory and visual disability. Severe neurodevelopmental
disability was defined as any one or combination of the following: non-ambulant
cerebral palsy, developmental delay (developmental quotient less than 70),
auditory and visual impairment.
Secondary outcomes:
1. Clinically significant adverse reactions attributed to the antifungal
agent that resulted in discontinuation of the therapy, for example:
a. abnormal hepatic function
b. abnormal renal function
c. gastrointestinal disturbance such as diarrhoea, feeding intolerance,
or necrotising enterocolitis that results in cessation of enteral feeding
d. hypokalaemia
e. cardiac dysrhythmias
f. thrombophlebitis
g. rash (including Stevens-Johnson reactions)
h. seizures
i. anaphylaxis
2. Emergence of organisms resistant to anti-fungal agents, as detected in infants enrolled in the study, or, in cluster-randomised studies, on surveillance of other infants in the same unit in the study centre (including infants who are admitted to the unit following completion of the study).
We examined references in previous reviews and in studies identified as potentially relevant. We hand searched the abstracts presented at Society for Pediatric Research and European Society for Pediatric Research, published in the journal Pediatric Research between 1984 and 2002 inclusive. Trials that have been reported only as abstracts were eligible if sufficient information was available from the report, or from contact with the authors, to fulfill the inclusion criteria.
We undertook a search of Science Citation Index from 1996 until 2003 to try to identify any potentially relevant trials that cited the included study (Driessen 1996). We did not identify any further trials with this search.
We contacted all of the manufacturers of anti-fungal agents that are listed in the current edition of the British National Formulary (BNF 2003): Bristol-Myers Squibb Pharmaceuticals Limited, Cambridge Laboratories, Elan Pharma Limited, Gilead Sciences Limited, ICN Pharmaceuticals Limited, Pfizer Limited). We did not obtain any information on any relevant reports that were not already available from public sources.
2. We used the criteria and standard methods of the Cochrane Neonatal Review Group to assess the methodological quality of the included trials. The quality of the trials was evaluated in terms of allocation concealment, blinding of parents or carers and assessors to intervention, and completeness of assessment in all randomised individuals. We requested additional information from the authors of each trial to clarify methodology and results as necessary.
3. We used a data collection form to aid extraction of relevant information and data from each included study. Each reviewer extracted the data separately, compared data, and resolved differences by consensus.
4. We used the standard methods of the Cochrane Neonatal Review Group to analyse and synthesize the data. For categorical data, we have expressed effects as relative risk, risk difference, and number needed to treat, with respective 95% confidence intervals. For continuous data, we planned to express the effects as weighted mean difference and 95% confidence interval.
5. We contacted the author to establish the outcomes of the preterm infants included in the study.
The study was undertaken between June 1992 to June 1993 in two tertiary neonatal centres in South Africa. Infants with proven fungal septicaemia, aged less than 3 months of age, were eligible for inclusion. Infants were randomised to receive either fluconazole or amphotericin B or, if meningitis was present, either fluconazole or amphotericin B plus 5-fluorocytosine. Treatment was continued in both groups until cultures were negative for one week and there was no laboratory evidence of infection.
Twenty-four infants were enrolled to the study. Thirteen infants were randomised to receive Fluconazole. The trial investigators excluded one infant in this group as the infant was found not to have invasive fungal infection. Of the remaining 12 infants in the fluconazole group, we excluded one term infant from the analysis for this review. Of the 11 infants randomised to receive Amphotericin, 10 were preterm. Death before hospital discharge was reported. Eight of 22 preterm infants enrolled in the study died, but one of these infants died after hospital discharge.
There were not any longer term data on outcomes after discharge. Data on adverse reactions to treatment including gastro-intestinal disturbance or thrombophlebitis were recorded throughout the study period. The investigators monitored the infants' renal, hepatic, and haematological function weekly throughout the study period.
Randomisation was computer generated independently for the two centres and via a sealed envelope system for individual case allocation. Both preterm infants and term infants were eligible for inclusion in the trial, and these groups were not randomised separately.
There were not any statistically significant differences between treatment groups in infant characteristics at trial entry. Follow-up was complete. The carers and assessors were blinded to randomisation. However, due to differences in the drug preparations, the carers and investigators were likely to be aware which drug each infant received.
Primary outcomes:
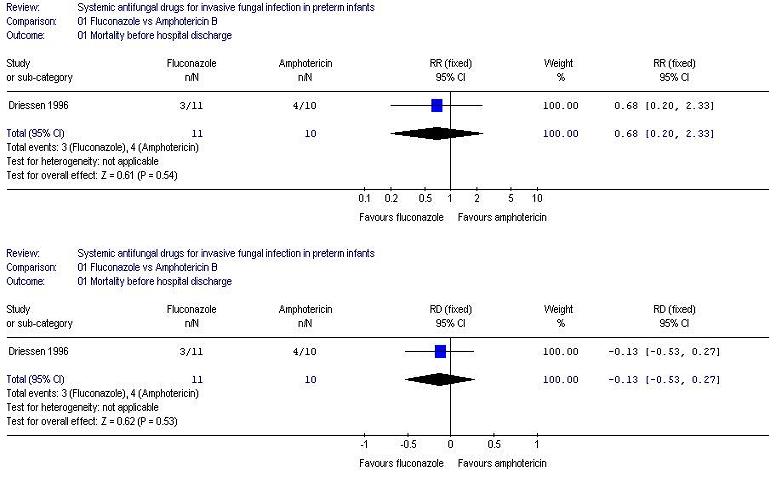
1. Death prior to hospital discharge: three of the 11 preterm infants in the fluconazole group died before discharge versus four of 10 in the amphotericin group: Relative risk (RR) 0.68 (95% confidence interval 0.20, 2.33), Risk Difference -0.13 (95% confidence interval -0.53, 0.27).
2. Neurodevelopmental outcome is not reported by this study.
Secondary outcomes:
1. This study reports adverse reactions. However, none of these resulted in discontinuation of treatment.
a. Hepatic function: There was not any statistically significant difference
in the plasma levels of liver enzymes gamma-glutamyl transpeptidase, aspartate
aminotransferase and alanine aminotransferase between the fluconazole and
amphotericin groups at the end of treatment.
b. Thrombophlebitis: One infant in the fluconazole group and five infants
in the amphotericin group had evidence of thrombophlebitis resulting in skin
abscesses (but not in discontinuation of treatment): RR 0.17 (95% CI 0.02,
1.24), Risk Difference -0.38 (95% confidence interval -0.71, -0.05). This
analysis includes the two term infants recruited in the trial.
c. Gastrointestinal disturbance: One infant in the fluconazole group had
severe vomiting. However this infant also had a disorder of branch chain amino
acid metabolism.
2. Emergence of antifungal resistance is not reported in this study
We were unable to undertake subgroup analysis of the azole antifungals, Amphotericin B versus lipid complex, or drugs in combination. We were also unable to analyse data for subgroups of confirmed versus suspected invasive fungal infection.
We identified only one eligible study. The included trial compared fluconazole with amphotericin B as treatment for preterm infants with invasive fungal infection. Although the study was of good methodological quality, the trial was very small (total of 22 preterm infants) and it is not possible to draw meaningful conclusions from the data. We did not find any studies which compared the use of amphotericin B with liposomal amphotericin B. Consequently, we do not know if treating preterm infants with invasive fungal infection with the newer antifungal agents compared with conventional amphotericin B improves clinical outcomes. In the particular case of suspected or confirmed fungal meningitis, the use of another agent which is known to cross the blood brain barrier should still be considered instead of or in combination with Amphotericin B.
Our pre-specified outcomes did not include any specific measure of convenience of drug administration or of the cost of the treatment course, although these may be related to the incidences of side-effects that result in discontinuation of therapy. The incidence of thrombophlebitis was statistically significantly lower in the group treated with fluconazole compared to amphotericin B, but this complication did not result in discontinuation of treatment. In the included study, there were no other instances of adverse events resulting in discontinuation of therapy. The trial also found that there were not any statistically significant differences in duration of treatment, days in hospital after enrollment to the study, or duration of need for a central venous line. However, the mean duration of intravenous antifungal therapy was statistically significantly lower for the fluconazole group (which is well absorbed orally and was prescribed enterally for part of the treatment course) compared with amphotericin B.
| Study | Methods | Participants | Interventions | Outcomes | Notes | Allocation concealment |
| Driessen 1996 | Blinding of randomisation: Yes
Blinding of intervention: No Complete follow-up: Yes Blinding of outcome measurement: |
22 preterm infants with invasive fungal infection, aged less than
3 months old. June 1992 to June 1993 in two tertiary neonatal centres in Witwatersrand, South Africa. |
Fluconazole 10mg/kg intra-venously or orally then 5mg/kg once
daily (N=10), versus Amphotericin B 1mg/kg/day infused intravenously over 4 to 6 hours (N=10). Treatment continued until fungal cultures negative for one week and no laboratory evidence of infection. |
Death before hospital discharge. Haematological, renal, hepatic functions; monitored weekly. Adverse reactions, convenience of use. |
24 infants were recruited to the study; Fluconazole 13, Amphotericin 11. In the fluconazole group, one infant was excluded by the investigators as the infant did not have invasive fungal infection. For this review, we have excluded one infant in the fluconazole group as the infant was born at term (this infant died). In the Amphotericin group, we excluded one infant from the analysis as the infant was born at term. | A |
Driessen M, Ellis JB, Cooper PA, Wainer S, Muwazi F, Hahn D, Gous H, De Villiers FP. Fluconazole versus amphotericin B for the treatment of neonatal fungal septicemia: a prospective randomized trial. Pediatr Infect Dis J 1996;15:1107-12.
* indicates the primary reference for the study
Adler-Shohet F, Waskin H, Lieberman JM. Amphotericin B lipid complex for neonatal invasive candidiasis. Arch Dis Child Fetal Neonatal Ed 2001;84:F131-3.
Austin NC, Darlow B. Prophylactic oral anti-fungal agents to prevent systemic candida infection in preterm infants (protocol for a Cochrane review). In: The Cochrane Library, Issue 4, 2002. Oxford: Update Software.
Joint Formulary Committee. British National Formulary. Vol. 43. London: British Medical Association and Royal Pharmaceutical Society of Great Britain, 2002.
Dupont B. Overview of the lipid formulations of amphotericin B. J Antimicrob Chemother 2002;49(Suppl 1):31-6.
Friedman S, Richardson SE, Jacobs SE, O'Brien K. Systemic candida infection in extremely low birth weight infants: short term morbidity and long term neurodevelopmental outcome. Pediatr Infect Dis J 2000;19:499-504.
Gotzsche PC, Johansen HK. Routine versus selective antifungal administration for control of fungal infections in patients with cancer (Cochrane review). In: The Cochrane Library, Issue 4, 2002. Oxford: Update Software.
Gussenhoven MJ, Haak A, Peereboom-Wynia JD, van 't Wout JW. Stevens-Johnson syndrome after fluconazole. Lancet 1991;338:120.
Hensey OJ, Cooke RW. Systemic candidiasis. Arch Dis Child 1982;57:962.
Hill HR, Mitchell TG, Matsen JM, Quie PG. Recovery from disseminated candidiasis in a premature neonate. Pediatrics 1974;53:748-52.
Huttova M, Hartmanova I, Kralinsky K, Filka J, Uher J, Kurak J, Krizan S, Krcmery V Jr. Candida fungemia in neonates treated with fluconazole: report of forty cases, including eight with meningitis. Pediatr Infect Dis J 1998;17:1012-5.
Johansen HK, Gotzsche PC. Amphotericin B lipid soluble formulations vs amphotericin B in cancer patients with neutropenia (Cochrane review). In: The Cochrane Library, Issue 4, 2002. Oxford: Update Software.
Johansen HK, Gotzsche PC. Amphotericin B versus fluconazole for controlling fungal infections in neutropenic cancer patients (Cochrane review). In: The Cochrane Library, Issue 4, 2002. Oxford: Update Software.
Juster-Reicher A, Leibovitz E, Linder N, Amitay M, Flidel-Rimon O, Even-Tov S, Mogilner B, Barzilai A. Liposomal amphotericin B (AmBisome) in the treatment of neonatal candidiasis in very low birth weight infants. Infection 2000;28:223-6.
Karlowicz MG, Rowen JL, Barnes-Eley ML, Burke BL, Lawson ML, Bendel CM, Shattuck KE, Horgan M, Albritton WL. The role of birth weight and gestational age in distinguishing extremely low birth weight infants at high risk of developing candidemia from infants at low risk: a multicenter study. Pediatr Res 2002;51:301A.
Keele DJ, DeLallo VC, Lewis RE, Ernst EJ, Klepser ME. Evaluation of amphotericin B and flucytosine in combination against Candida albicans and Cryptococcus neoformans using time-kill methodology. Diagn Microbiol Infect Dis 2001;41:121-6.
Kontoyiannis DP, Bodey GP, Mantzoros CS. Fluconazole vs. amphotericin B for the management of candidaemia in adults: a meta-analysis. Mycoses 2001;44:125-35.
Kossoff EH, Buescher ES, Karlowicz MG. Candidemia in a neonatal intensive care unit: trends during fifteen years and clinical features of 111 cases. Pediatr Infect Dis J 1998;17:504-8.
Makhoul IR, Sujov P, Smolkin T, Lusky A, Reichman B. Epidemiological, clinical, and microbiological characteristics of late-onset sepsis among very low birth weight infants in Israel: a national survey. Pediatrics 2002;109:34-9.
McDougall PN, Fleming PJ, Speller DC, Daish P, Speidel BD. Neonatal systemic candidiasis: a failure to respond to intravenous miconazole in two neonates. Arch Dis Child 1982;57:884-6.
McGuire W, Austin N. Prophylactic intravenous antifungal agents to prevent mortality and morbidity in very low birth weight infants (protocol for a Cochrane review). In: The Cochrane Library, Issue 4, 2002. Oxford: Update Software.
Neely MN, Schreiber JR. Fluconazole prophylaxis in the very low birth weight infant: not ready for prime time. Pediatrics 2001;107:404-5.
Rogers TR, Barnes RA, Denning DW, Evans EG, Hay RJ, Prentice AG, Speller DC, Warnock DW, Warren RE. Antifungal drug susceptibility testing. Working Party of the British Society for Antimicrobial chemotherapy. J Antimicrob Chemother 1995;36:899-909.
Rowen JL, Tate JM. Management of neonatal candidiasis. Neonatal Candidiasis Study Group. Pediatr Infect Dis J 1998;17:1007-11.
Saiman L, Ludington E, Pfaller M, Rangel-Frausto S, Wiblin RT, Dawson J, Blumberg HM, Patterson JE, Rinaldi M, Edwards JE, Wenzel RP, Jarvis W. Risk factors for candidemia in neonatal intensive care unit patients. The National Epidemiology of Mycosis Survey Study Group. Pediatr Infect Dis J 2000;19:319-24.
Stoll BJ, Gordon T, Korones SB, Shankaran S, Tyson JE, Bauer CR, Fanaroff AA, Lemons JA, Donovan EF, Oh W, Stevenson DK, Ehrenkranz RA, Papile LA, Verter J, Wright LL. Late-onset sepsis in very low birth weight neonates: a report from the National Institute of Child Health and Human Development Neonatal Research Network. J Pediatr 1996;129:63-71.
Stoll BJ, Hansen N, Fanaroff AA, Wright LL, Carlo WA, Ehrenkranz RA, Lemons JA, Donovan EF, Stark AR, Tyson JE, Oh W, Bauer CR, Korones SB, Shankaran S, Laptook AR, Stevenson DK, Papile LA, Poole WK. Late-onset sepsis in very low birth weight neonates: The experience of the NICHD Neonatal Research Network. Pediatrics 2002;110:285-91.
Te Dorsthorst DT, Verweij PE, Meletiadis J, Bergervoet M, Punt NC, Meis JF, Mouton JW. In vitro interaction of flucytosine combined with amphotericin B or fluconazole against thirty-five yeast isolates determined by both the fractional inhibitory concentration index and the response surface approach. Antimicrob Agents Chemother 2002;46:2982-9.
Tuck, S. Neonatal systemic candidiasis treated with miconazole. Arch Dis Child 1980;55:903-6.
Vermes A, van Der Sijs H, Guchelaar HJ. Flucytosine: correlation between toxicity and pharmacokinetic parameters. Chemotherapy 2000;46:86-94.
Weitkamp JH, Poets CF, Sievers R, Musswessels E, Groneck P, Thomas P, Bartmann P. Candida infection in very low birth-weight infants: outcome and nephrotoxicity of treatment with liposomal amphotericin B (AmBisome). Infection 1998;26:11-5.
01.01 Mortality before hospital discharge
01.02 Presence of thrombophlebitis
| Comparison or outcome | Studies | Participants | Statistical method | Effect size |
|---|---|---|---|---|
| 01 Fluconazole vs Amphotericin B | ||||
| 01 Mortality before hospital discharge | 1 | 21 | RR (fixed), 95% CI | 0.68 [0.20, 2.33] |
| 02 Presence of thrombophlebitis | 1 | 24 | RR (fixed), 95% CI | 0.17 [0.02, 1.24] |
| This review is published as a Cochrane review in
The Cochrane Library 2004, Issue 1, 2004 (see www.CochraneLibrary.net for
information). Cochrane reviews are regularly updated as new evidence emerges
and in response to comments and criticisms, and The Cochrane Library should
be consulted for the most recent version of the Review. |
{kind=link}
{kind=link}