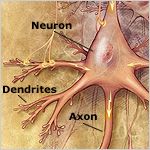
The healthy human brain is made up of billions of different kinds of nerve cells (neurons) that are connected through a diverse array of chemical and electrical signals. A typical neuron has a nucleus in a cell body, an axon, and many dendrites. Neuronal function is supported by other kinds of cells called glial cells.
The nucleus contains the cell's genetic blueprint and helps regulate the cell's activities in response to signals from outside and inside the cell. The axon transmits messages to other neurons. Dendrites receive messages from axons of other nerve cells or from specialized sense organs.
The survival of neurons depends on the healthy functioning of several interdependent processes:
- Communication. When a neuron receives enough messages from surrounding cells, an electrical charge is generated that travels down to the end of the axon. Here, it triggers the release of special chemicals, called neurotransmitters, that move across a gap, called a synapse, to the dendrites of neighboring neurons. Scientists estimate that the typical neuron has up to 15,000 synapses. The neurotransmitters bind to specific receptor sites on the other dendrites, triggering chemical changes and building up new electrical charges.
- Metabolism. This process encompasses all the chemical reactions that take place in the cell. Efficient metabolism requires adequate blood circulation to supply the cells with oxygen and glucose, the brain's major fuel.
- Repair. Neurons are programmed to live a long time—even more than 100 years—so they must constantly maintain, repair, and remodel themselves.
How Does AD Affect the Brain?
In healthy aging, most types of brain neurons are not lost in large numbers. In AD, however, many nerve cells stop functioning, lose connections with other nerve cells, and die because communication, metabolism, and repair are disrupted.
At first, AD destroys neurons in parts of the brain that control memory, including the entorhinal cortex, the hippocampus, and related structures. AD later attacks the areas responsible for language and reasoning. Eventually, many other areas of the brain are damaged and the person becomes helpless and unresponsive to the outside world.
What are the Main Characteristics of the Brain in AD?
Many changes take place in the brain of a person with AD. The three major characteristics that reflect the pathology caused by the disease are:
- Amyloid plaques. Plaques are found in the spaces between neurons. They consist of largely insoluble deposits of a protein fragment called beta-amyloid peptide, together with other proteins, remnants of neurons, degenerating dendrites and axons, glia, and other cellular material. Scientists used to think that plaques caused the damage to neurons seen in AD. Now, however, many think that earlier, more soluble forms of beta-amyloid may be the major culprits (see "How Does AD Begin, and What Causes it to Progress?" for more details on the plaque formation process).
- Neurofibrillary tangles (NFTs). NFTs, which are found inside neurons, are abnormal collections of a protein called tau. Healthy neurons are internally supported in part by structures called microtubules, which help guide nutrients and molecules from the cell body to the ends of the axon and back. Tau, which normally has a certain number of phosphate molecules attached to it, binds to microtubules and stabilizes them. In AD, an abnormally high number of additional phosphate molecules attach to the tau. As a result, tau disengages from the microtubules and begins to clump together with other threads of tau, eventually forming NFTs. When this happens, the microtubules disintegrate and the neuron's transport system collapses.
- Loss of connections between cells and cell death. This feature of AD likely results from the accumulation of beta-amyloid and abnormal tau. When neurons lose their connections, they cannot function properly and eventually they die. As neuronal death spreads through the brain, affected regions begin to shrink in a process called brain atrophy. By the final stage of AD, damage is widespread and brain tissue has shrunk significantly.
What Causes AD?
In a very few families, people develop AD in their 30s, 40s, and 50s. These people have a mutation in one of three genes that they have inherited from a parent. We know that mutations in these genes cause AD in these "early-onset" cases.
More than 90 percent of AD develops in people older than 65. This form of AD is called "late-onset" AD, and its development and pathology are very similar to that of early-onset AD. We don't yet completely understand the causes of late-onset AD, but they probably include genetic, environmental, and lifestyle factors. The importance of these factors in increasing or decreasing the risk of developing AD differs from person to person. Scientists hope that what they learn about early-onset AD also can be applied to the late-onset form of the disease.
Perhaps the greatest mystery is why AD largely strikes the elderly. Why does it take 30 to 50 years for people to develop signs of the disease? Research on how the brain changes normally as people age will help provide answers to this important question in AD.
How is AD Diagnosed?
 Clinicians today use a range of tools to diagnose "possible AD" (dementia could also be due to another condition) or "probable AD" (no other cause of dementia can be found). These tools include a medical history; physical exam; tests that measure memory, language skills, and other abilities related to brain functioning; and usually, brain scans. Knowledge about the clinical and behavioral characteristics of the disease also helps in diagnosing AD. In specialized research facilities, clinicians can now diagnose AD with up to 90 percent accuracy. At this time, however, AD can be diagnosed conclusively only by an autopsy of the brain of a person with dementia.
Clinicians today use a range of tools to diagnose "possible AD" (dementia could also be due to another condition) or "probable AD" (no other cause of dementia can be found). These tools include a medical history; physical exam; tests that measure memory, language skills, and other abilities related to brain functioning; and usually, brain scans. Knowledge about the clinical and behavioral characteristics of the disease also helps in diagnosing AD. In specialized research facilities, clinicians can now diagnose AD with up to 90 percent accuracy. At this time, however, AD can be diagnosed conclusively only by an autopsy of the brain of a person with dementia.
Early, accurate diagnosis is crucial because it tells people not only whether they do or do not have AD but also whether they have something else instead, such as a stroke, tumor, Parkinson's disease, or side effects of medications. It also helps families plan for the future while the person with AD can still participate in making decisions. Researchers are making progress in developing accurate diagnostic tests and techniques that may one day be used in general medical practice to detect the disease early, ideally even before symptoms emerge.
How is AD Treated?
AD treatments are needed to control cognitive loss as well as behavioral and psychiatric problems that occur as AD progresses. Four FDA-approved medications are used to treat AD symptoms. Donepezil (Aricept), rivastigmine (Exelon), and galantamine (Reminyl) are prescribed to treat mild to moderate AD symptoms. Donepezil was recently approved to treat severe AD as well. These drugs act by stopping or slowing the action of acetylcholinesterase, an enzyme that breaks down acetylcholine (a neurotransmitter that helps in memory formation). The drugs maintain some patients' abilities to carry out activities of daily living; may maintain some thinking, memory, or speaking skills; and can help with certain behavioral symptoms. However, they will not stop or reverse AD and appear to help patients only for months to a few years.
The newest AD medication is memantine (Namenda), which is prescribed to treat moderate to severe AD symptoms. This drug appears to work by regulating levels of glutamate, another neurotransmitter involved in memory function. Like the cholinesterase inhibitors, memantine will not stop or reverse AD.
In addition to these medications, physicians use drug and non-drug approaches to treat behavioral and psychiatric problems. These problems include agitation, verbal and physical aggression, wandering, depression, sleep disturbances, and delusions.
<< Back | Next >>
