Elective high frequency oscillatory ventilation versus conventional
ventilation for acute pulmonary dysfunction in preterm infants
Henderson-Smart DJ, Cools F, Bhuta T, Offringa M
Dates
Date edited: 08/06/2007
Date of last substantive update: 14/05/2007
Date of last minor update: / /
Date next stage expected 14/05/2009
Protocol first published:
Review first published: Issue 1, 1997
Contact reviewer
Prof David J Henderson-Smart
Director
NSW Centre for Perinatal Health Services Research
Queen Elizabeth II Research Institute
Building DO2
University of Sydney
Sydney
NSW AUSTRALIA
2006
Telephone 1: +61 2 93517318
Telephone 2: +61 2 93517728
Facsimile: +61 2 93517742
E-mail: dhs@mail.usyd.edu.au
Contribution of reviewers
An earlier version of this review was developed by Bhuta and Henderson-Smart and published in 1996. Both authors were involved at all stages in the review. In 1999 the review was reformatted by Henderson-Smart with inclusion of two new reviewers, Cools and Offringa. Each author evaluated the trials and extracted data independently. Henderson-Smart entered the data and wrote the text while all the co-reviewers contributed to data checking and editing. The current update included a search by Henderson-Smart and Cools who both evaluated and extracted the data from 4 new trials. Henderson-Smart entered the data and edited the review. The review was evaluated by all authors.Internal sources of support
Royal Prince Alfred Hospital, Sydney, AUSTRALIA
Department of Neonatology, Royal North Shore Hospital, Sydney, AUSTRALIA
Department of Neonatology, Academic Medical Centre, Amsterdam, NETHERLANDS
Centre for Perinatal Health Services Research, University of Sydney, AUSTRALIA
External sources of support
NoneWhat's new
This updates the review 'Elective high frequency oscillatory ventilation versus conventional ventilation for acute pulmonary dysfunction in preterm infants' published in The Cochrane Library, Issue 1, 2003 (Henderson-Smart 2003). As a result of a search update to Novemer 2006, data from four trials have been added. One new trial is still awaiting assessment and another is yet to be published.
Additional subgroup analyses have been added to explore heterogeneity.
Dates
Date review re-formatted: 30/08/1999
Date new studies sought but none found: 24/04/2007
Date new studies found but not yet included/excluded: 28/10/2006
Date new studies found and included/excluded: 28/10/2006
Date reviewers' conclusions section amended: 28/10/2006
Date comment/criticism added: / /
Date response to comment/criticisms added: / /
Text of review
Synopsis
Insufficient evidence exists to support the routine use of high frequency oscillatory ventilation (HFOV) instead of conventional ventilation for preterm infants with lung disease who are given positive pressure ventilation.
High frequency oscillatory ventilation is a way of providing artificial ventilation of the lungs that theoretically may produce less injury to the lungs and therefore reduce the rate of chronic lung disease. This review of the evidence from fifteen randomised controlled trials showed variable results between studies and no clear overall benefit or harm resulting from HFOV.
Abstract
Background
Respiratory failure due to lung immaturity is a major cause of mortality in preterm infants. Although the use of intermittent positive pressure ventilation (IPPV) in neonates with respiratory failure saves lives, its use is associated with lung injury and chronic lung disease (CLD). Conventional IPPV is provided at 30-80 breaths per minute, while a newer form of ventilation called high frequency oscillatory ventilation (HFOV) provides 'breaths' at 10 - 15 cycles per second. This has been shown to result in less lung injury in experimental studies.
Objectives
The objective of this review is to determine the effect of the elective use of high frequency oscillatory ventilation (HFOV) as compared to conventional ventilation (CV) in preterm infants who are mechanically ventilated for respiratory distress syndrome (RDS), on the incidence of chronic lung disease, mortality and other complications associated with prematurity and assisted ventilation.
Search strategy
Searches were made of the Oxford Database of Perinatal Trials, MEDLINE, EMBASE, previous reviews including cross references, abstracts, conferences and symposia proceedings, expert informants, journal hand searching by the Cochrane Collaboration, mainly in the English language. The search was updated in April 2007.
Selection criteria
Randomised controlled trials comparing HFOV and CV in preterm or low birth weight infants with pulmonary dysfunction, mainly due to RDS, who were given IPPV. Randomisation and commencement of treatment needed to be as soon as possible after the start of IPPV and usually in the first 12 hours of life.
Data collection & analysis
The methodological quality of each trial was independently reviewed by the various authors. The standard effect measures are relative risk (RR) and risk difference (RD). From 1/RD the number needed to treat (NNT) to produce one outcome were calculated. For all measures of effect, 95% confidence intervals were used. In subgroup analyses the 99% CIs are also given for summary RRs in the text. Meta-analysis was performed using a fixed effects model. Where heterogeneity was over 50%, the random effects RR is also given.
Main results
Fifteen eligible studies of 3,585 infants were included. Meta-analysis comparing HFOV with CV revealed no evidence of effect on mortality at 28 - 30 days of age or at approximately term equivalent age. These results were consistent across studies and in subgroup analyses. The effect of HFOV on CLD in survivors at term equivalent gestational age was inconsistent across studies and the reduction was of borderline significance overall. Subgroups of trials showed a significant reduction in CLD with HFOV when high volume strategy for HFOV was used, when piston oscillators were used for HFOV, when lung protective strategies for CV were not used, when randomisation occurred at two to six hours of age, and when inspiratory:expiratory ratio of 1:2 was used for HFOV. In the meta-analysis of all trials, pulmonary air leaks occurred more frequently in the HFOV group.
In some studies, short-term neurological morbidity with HFOV was found, but this effect was not statistically significant overall. The subgroup of two trials not using a high volume strategy with HFOV found increased rates of Grade 3 or 4 intraventricular haemorrhage and of periventricular leukomalacia. An adverse effect of HFOV on long-term neurodevelopment was found in one large trial but not in the five other trials that reported this outcome. The rate of retinopathy of prematurity is reduced overall in the HFOV group.
Reviewers' conclusions
There is no clear evidence that elective HFOV offers important advantages over CV when used as the initial ventilation strategy to treat preterm infants with acute pulmonary dysfunction. There may be a small reduction in the rate of CLD with HFOV use, but the evidence is weakened by the inconsistency of this effect across trials and the overall borderline significance. Future trials on elective HFOV should target those infants who are at most risk of CLD (extremely preterm infants), compare different strategies for generating HFOV and CV, and report important long-term neurodevelopmental outcomes.
Background
Pulmonary disease continues to be the major cause of morbidity and mortality in very preterm infants. Although assisted ventilation with intermittent positive pressure ventilation (IPPV) has decreased mortality, morbidity from lung injury is high. Acute injury such as pulmonary air leak was common prior to the availability of surfactant. Chronic lung disease (CLD) develops in up to one third of preterm infants with the respiratory distress syndrome (RDS) who receive IPPV (Northway 1992; Ehrenkrantz 1992). In addition to immaturity, over distention of the lung and oxygen toxicity are thought to be important factors in the pathogenesis of CLD (Jobe 2000).
In order to avoid distortion of the lung caused by the large swings in pulmonary pressures during conventional ventilation (CV) at rates of 30 - 80, high frequency oscillatory ventilation (HFOV) at rates of 600 - 800 per minute was developed. In animal models, the use of HFOV results in more uniform lung inflation, improves oxygenation and reduces the severity of lung pathology produced by IPPV (Truog 1984; de Lemos 1987).
As discussed by Clark 2000, there are strategies that reduce lung injury with both HFOV and CV. Animal studies show that lung volume maintenance with HFOV prevents lung injury (McCulloch 1988). The effectiveness of HFOV might also be enhanced by the use of more powerful piston driven ventilators compared with those that generate the oscillations by flow interruption (Jouvet 1997), and even by certain settings with the same type of ventilator (inspiratory/expiratory ratio of 1/1 versus 1/2, Pillow 1999). Various strategies with CV appear to reduce acute lung injury. These include avoiding high tidal volumes, using positive end expiratory pressure (PEEP) and using short inspiratory times and faster rates. Allowing carbon dioxide to rise (permissive hypercapnoea) rather than increasing ventilation may also reduce lung injury in preterm infants (Woodgate 2006). Many of these treatment strategies and their effects on lung injury are based on pathophysiological studies in animal models (increased cytokine release with higher tidal volumes and reduced PEEP, Meredith 1989) or trials in adults with RDS (Petrucci 2006). There is evidence in preterm infants that strategies to synchronise ventilation (higher rates and patient triggered ventilation) reduce the rate of pneumothorax and the duration of ventilation (Greenough 2003), although there is no evidence that these strategies reduce CLD at 36 weeks postmenstrual age.
Objectives
The objective of this review is to determine the effect of the elective use of high frequency oscillatory ventilation (HFOV) when compared to conventional ventilation (CV) in preterm infants who are mechanically ventilated for RDS on the incidence of chronic lung disease, mortality and other complications associated with prematurity and assisted ventilation.
The following subgroup analyses pre-specified:
(1) Management of HFOV: A strategy to maintain lung volume has the potential for better alveolar recruitment compared to a strategy to maintain one of low volume, and thus might result in better outcomes in terms of CLD. A 'high volume strategy' (HVS) with HFOV was defined as one in which two or more of the following treatment approaches were explicitly stated in the methods: initial use of a higher mean airway pressure than on CV; initial weaning of fractional inspired oxygen before mean airway pressure; and use of alveolar recruitment manoeuvres.
(2) Surfactant replacement: Surfactant replacement therapy would increase alveolar recruitment, attenuate RDS, and lead to less lung injury and CLD. A similar pulmonary benefit could occur in infants whose mothers received antenatal corticosteroids.
(3) Birth weight and gestational age: Outcomes might differ in groups of infants born at different weights and gestational ages. Infants born at very low gestation and/or with very low birth weight have a higher incidence of CLD and may benefit more from HFOV. On the other hand, these infants are more susceptible to neurological complications such as intraventricular haemorrhage (IVH) and periventricular leukomalacia (PVL).
In order to explain persisting heterogeneity in the meta-analyses in previous versions of this review, the following subgroup analyses were added for the 2007 update:
(4) Type of HFOV ventilator: True (piston) HFO ventilators might be more effective in maintaining lung volume and lead to different effects compared with those that use flow interruption. Also, differences in inspiratory:expiratory times on HFOV may affect lung injury.
(5) Management of CV: Lung protective strategies on CV (short inspiratory times, rates of ≥60/minute, PEEP of 4 - 6 cms H20, limiting tidal volume, patient triggering or permissive hypercapnoea) may affect the differences between HFOV and CV.
(6) Duration of ventilation prior to randomization or age at randomization: The treatment that infants receive prior to randomisation could alter outcomes and this could be measured by duration of ventilation prior to randomisation and/or age at randomisation.
Criteria for considering studies for this review
Types of studies
Randomised or quasi-randomised controlled trials.
Types of participants
Preterm or low birth weight infants with pulmonary dysfunction, mainly due to RDS, who were considered to require IPPV.
Types of interventions
Elective HFOV vs. CV, with randomisation early in the course of RDS soon after mechanical ventilation was begun. Such trials were classified as ' elective'. Trials were classified as 'rescue', and therefore excluded from this review, when patients were randomised after failure to adequately ventilate on CV or when complications of CV developed or were likely to develop. The use of HFOV as rescue therapy and the use of elective high frequency jet ventilation are the subjects of other reviews (Bhuta 2005; Bhuta 2003). Trials were not eligible if cross-over of interventions were mandatory.
Types of outcome measures
Outcomes from trials were not eligible if there was a 20% or greater rate of missing or unreported data.
Primary
1. Mortality at 28 - 30 days and at term equivalent age
2. Chronic lung disease
Oxygen dependency at 28 - 30 days (with and without chest x-ray changes)
Oxygen dependency or use of assisted ventilation at 36 - 37 weeks postmenstrual age (PMA) or discharge
3. Death or chronic lung disease
Secondary
4. Failure of allocated treatment to maintain gas exchange, leading to cross over to alternate treatment
5. Pulmonary air leak syndromes - all [including pulmonary interstitial emphysema - (PIE) and gross extrapulmonary air leak (such as pneumothorax)]
6. Intraventricular haemorrhage
All grades
Grades 3 (ventricles distended with blood) or 4 (parenchymal involvement)
7. Periventricular leukomalacia
8. Retinopathy of prematurity (ROP) - grade 2 or more
9. Use of hospital resources (length of hospital stay, duration of IPPV)
10. Long term growth and neurodevelopment
Search strategy for identification of studies
Searches were made of the Oxford Database of Perinatal Trials, Cochrane Controlled Trials Register (CENTRAL, The Cochrane Library Issue 2, 2007, MEDLINE and EMBASE (using MeSH headings 'high-frequency-ventilation' and 'infant, preterm' from 1983 to April 2007), previous reviews including cross references, abstracts, conferences and symposia proceedings, expert informants, journal hand searching by the Cochrane Collaboration, mainly in the English language. Expert informant's search in the Japanese language was made by Prof. Y. Ogawa in 1996. Abstracts of the annual meetings of Society for Pediatric Research (1996 - 2006 inclusive) were also searched.
Methods of the review
The standard methods of the Cochrane Collaboration and the Cochrane Neonatal Review Group (CNRG) were used to evaluate the methodological quality of each trial. Trials were reviewed independently by each author for eligibility. Data were extracted separately by each author, then compared and any differences resolved.
Additional information was obtained from Ogawa 1993; Gerstmann 1996; Rettwitz-Volk 1998; Thome 1998; Plavka 1999; Moriette 2001 and Johnson 2002 regarding trial methodology. Schreiber 2003 re-analysed their trial data on use of nitric oxide to evaluate outcomes related to HFOV/CV to which the infants were also randomised. Clark 1992 and Plavka 1999 provided information on infants excluded post-randomisation, which allowed for an intention to treat analysis. Plavka 1999; Moriette 2001 and Van Reempts 2003 provided additional outcome information from their trials (see Table of Included Studies for details).
Results for outcomes requiring survival to a given age are reported with survivors as the denominator (IPPV, CLD ). Survival was used as the denominator for ROP, where the number examined was not given (HIFI 1989; Schreiber 2003, Van Reempts 2003).
The standard method of the CNRG was used to analyse the data. Treatment effects were expressed using relative risk (RR) and risk difference (RD). From 1/RD the number needed to treat (NNT) to produce one outcome was calculated. For each measure the 95% confidence intervals (CI) are routinely given. In subgroup analyses the 99% CIs are also given for summary RRs in the text. Meta-analysis was performed using a fixed effects model. Where heterogeneity was over 50%, the random effects RR is also given.
Description of studies
Overall, 20 randomised controlled trials of HFOV vs. CV were found, of which 15 met eligibility criteria and full trial data were available. Details of each of these included studies (HIFI 1989; Clark 1992; Ogawa 1993; Gerstmann 1996; Rettwitz-Volk 1998; Thome 1998; Plavka 1999; Moriette 2001; Durand 2001; Courtney 2002; Johnson 2002; Van Reempts 2003; Craft 2003; Schreiber 2003; Vento 2005) are given in the Table of Included Studies.
The study by Froese 1987 has not been included because after randomisation of infants (unknown gestation range) with presumed RDS, 5 of 11 in the HFOV group and an unknown number from the CV group were excluded from the comparisons between treatments. Only data on infants < 29 weeks with RDS were reported. Lombert 1996 has been excluded because there was 22% loss after randomisation. Cambonie 2003 was not included as the trial only examined haemodynamic status during HFOV compared to CV and clinical outcomes were not reported.
Two other studies have been excluded from the review. HiFO 1993 was excluded since HFOV was used as rescue therapy. This study is included in a separate review of HFOV (Bhuta 2005). The study by Ramanathan 1995, which has only been published in abstract form, was excluded because there was a mandatory crossover from HFOV to CV at 96 hours of age. Some information from these latter two trials concerning rates of IVH is considered in the discussion.
Participants
All but three (Clark 1992; Plavka 1999; Van Reempts 2003) of the included studies were multicentre. The total number of infants randomised in each study varied from 40 (Craft 2003) to 673 (HIFI 1989). All studies included preterm infants, although the upper limit for birth weight or gestation differed. This upper limit for birth weight was 1001 g in one (Craft 2003) 1200 g in two (Courtney 2002; Durand 2001) 1500 g in two (Rettwitz-Volk 1998; Plavka 1999), 1750 g in one (Clark 1992), 2000 g in two (HIFI 1989, Ogawa 1993). Upper gestational age limits were 35 weeks in one (Gerstmann 1996), 34 weeks in one (Schreiber 2003), 32 weeks in one (Van Reempts 2003), 30 weeks in two (Thome 1998, Moriette 2001) and 29 weeks in one (Johnson 2002). The average age at randomisation varied from less than one hour (Thome 1998; Johnson 2002) to 12 hours (Schreiber 2003). Each trial stratified infants at randomisation by weight or gestational age, although few data are reported by these subgroups.
Prenatal corticosteroid use was not reported in two trials (HIFI 1989; Ogawa 1993); they were used in a minority of women in two trials (Clark 1992; Gerstmann 1996) and used in 50 - 92% of women in the remaining seven trials.
Interventions
Different ventilators were used to deliver HFOV. Four trials used the Sensormedics 3100 (Clark 1992; Gerstmann 1996; Plavka 1999; Courtney 2002), two used the Hummingbird (HIFI 1989; Ogawa 1993), one used a Stephan piston oscillator (Rettwitz-Volk 1998), one used an Infant Star ventilator (Thome 1998), one used a French piston oscillator (Moriette 2001), one (Van Reempts 2003) used either Sensormedics 3100 (71%) or Infant Star (29%) and one (Johnson 2002) used a variety of ventilators (Sensormedics, SLE, Draeger). HFOV was delivered at 10-15 Hz in 12 trials and at 15-20 Hz in one (Rettwitz-Volk 1998).
The three criteria used to define a high volume strategy (HVS) with HFOV are given in the objectives. All 13 trials with a HVS used a higher mean airway pressure (MAP) on HFOV than on CV. In addition, two trials (Thome 1998; Moriette 2001) used both alveolar recruitment manoeuvres and weaning of FiO2 prior to weaning MAP, while Gerstmann 1996; Clark 1992 and Van Reempts 2003 used weaning of FiO2 first and Ogawa 1993 used alveolar recruitment manoeuvres. Two trials (HIFI 1989; Rettwitz-Volk 1998) did not use a HVS for HFOV.
In all trials, CV was administered using time cycled, pressure limited ventilators. There was a large variation in the specific methods of administration of CV that might provide lung protection. Details are given in the Table of Included Studies.
Surfactant therapy with animal derived extracts was used as therapy for RDS in the majority of participants in all but two trials (HIFI 1989; Clark 1992).
Postnatal corticosteroids for CLD were used in 41 - 61% of infants in three trials (Rettwitz-Volk 1998; Thome 1998, Courtney 2002), in 20% of infants in one trial (Johnson 2002) and in less than eight per cent of infants in two trials (Moriette 2001; Van Reempts 2003). Plavka 1999 reported cumulative dosage and Courtney 2002 reported mean days of therapy in infants in each group. In all studies, the usage of postnatal steroids was similar in the two treatment groups. In the Vento 2005 trial, corticosteroids were administered to 35% of survivors in the HFOV group and to 60% of survivors in the CV group.
In Durand 2001 and Courtney 2002 prophylactic indomethacin was given routinely to all infants.
Outcomes
Not all outcomes were reported in each study. The definitions of CLD 'at 28 days' differed between studies. CLD was assessed at 28 days of age in six studies (HIFI 1989; Ogawa 1993; Rettwitz-Volk 1998; Thome 1998; Moriette 2001; Van Reempts 2003; Schreiber 2003) and 30 days of age in the other two (Clark 1992; Gerstmann 1996). In five studies, the definition of CLD at 28 days of age was based on oxygen therapy alone (Rettwitz-Volk 1998; Thome 1998; Plavka 1999; Moriette 2001; Schreiber 2003) while in the remainder both oxygen therapy and an abnormal chest x-ray were required.
'Late' CLD at term equivalent age varied from 36 weeks PMA (Clark 1992; Thome 1998; Plavka 1999; Moriette 2001; Courtney 2002; Johnson 2002) or 37 weeks PMA (Rettwitz-Volk 1998) to 'at discharge' [Gerstmann 1996, mean PMA 37.1 (36.5, 37.9) weeks in HFOV group and 37.5 (36.6, 38.0) weeks in CV group]. The criteria for CLD at term equivalent age was based on use of oxygen therapy in nine trials, on clinical score (oxygen plus signs) in one trial (Plavka 1999), on oxygen or use of assisted ventilation in two trials (Courtney 2002; Van Reempts 2003) and on oxygen use plus an abnormal chest Xray in one trial (Schreiber 2003).
In each trial, cross-over to the other treatment was allowed when pre-determined failure criteria were reached. These criteria (hypoxaemia and/or hypercarbia) were similar in each trial and for each treatment group, but the decision to cross over was left to the clinician. In two trials (Clark 1992; Rettwitz-Volk 1998), the additional criterion for cross-over of severe pulmonary interstitial emphysema was applied only to the CV group. Because of the variable definition of 'failure of assigned treatment' between treatment groups, this outcome has not been included in the meta-analysis. When cross-over occurred, the subjects were analysed the groups as randomised.
Methodological quality of included studies
Details of the methodological quality of each study are available in the Table of Included Studies.
Randomisation: there were adequate efforts to conceal treatment assignment in each study.
Blinding of treatment: not possible in any study.
Exclusions after randomisation: minimal for primary outcomes (all less than 8%).
Blinding of outcome assessment: variable between outcomes and studies. Assessment of chest x-rays for the diagnosis of CLD was blinded as to treatment group in studies by Clark 1992; Ogawa 1993; Plavka 1999 and Moriette 2001; Schreiber 2003. Blinded head ultrasound assessments were carried out in the HIFI 1989, Clark 1992, Ogawa 1993, Moriette 2001; Durand 2001;Courtney 2002; Johnson 2002; Van Reempts 2003 and Schreiber 2003 trials.
Results
Fifteen trials involving 3585 infants were included.
Mortality
There were no significant differences in the rates of mortality by 28 - 30 days [outcome 01-01, 2060 infants in nine trials, summary RR 1.09 (95% CI 0.88, 1.35)] or in the rates of mortality by 36 - 37 weeks PMA or discharge [Comparison 01-06, 2820 infants in 13 trials, summary RR 0.98 (95% CI 0.83, 1.14)], either in any individual trial or in the overall analyses . Subgroup analyses including use of volume recruitment on HFOV, routine use of surfactant , use of piston oscillators, use of lung protective strategies on CV and inspiratory:expiratory ratio on HFOV also failed to show any significant differences in mortality rates.
Chronic lung disease at 28-30 days
The use of oxygen therapy at 28 - 30 days was reported for 1043 infants in six trials. There was no significant difference between the HFOV and CV groups in the individual trials, or in the meta-analysis [Comparison 01-03, summary RR 0.98 (95% CI 0.88, 1.10)].
CLD in survivors at 28-30 days of age, based on the use of oxygen or mechanical ventilation and the presence of an abnormal chest x-ray, was reported for 820 infants in four trials (outcome 01-04). Two trials (Clark 1992; Gerstmann 1996) showed a significantly lower incidence of this outcome in the HFOV group and there was a trend towards a reduced incidence in the overall analysis [summary RR 0.86 (95% CI 0.74, 1.01)]. This latter meta-analysis showed significant heterogeneity (I2 = 71.3% ) and when a random effects model was used the summary RR is 0.66 (95% CI 0.41, 1.07).
Five trials involving 1160 infants reported both mortality and CLD at 28 - 30 days (outcome 01-05). Two showed a significant decrease of this combined outcome in the HFOV group (Clark 1992; Gerstmann 1996). In the overall analysis, there was a non-significant trend towards a reduced risk of 'death or CLD at 28-30 days' in the HFOV group [summary RR 0.94 (95% CI 0.85, 1.04)] .
CLD at 36 - 37 weeks postmenstrual age (PMA) in survivors
CLD in survivors at 36 - 37 weeks PMA or at discharge was reported for 2310 infants in 13 trials (outcome 01- 07). Four trials (Clark 1992; Gerstmann 1996; Durand 2001; Vento 2005) found a significant decrease in the HFOV group. In the overall analysis using a fixed effects model, there was a reduction of CLD in the HFOV group [summary RR 0.89 (95% CI 0.81, 0.99), RD 0.04 (95% CI -0.08, -0.01)] of borderline significance. There was significant heterogeneity in this meta-analysis (I2 = 63.2%) and using a random effects model gave a summary RR of 0.83 (95% CI 0.68, 1.03), which is not significant.
Subgroup analyses
The analysis of the subgroup of 12 trials (2223 infants) using a high volume strategy (HVS) on HFOV (outcome 02-02) did not differ from the overall analysis because only one trial reporting CLD at 36 weeks PMA did not use a HVS, and it had no cases of CLD to contribute to the overall analysis.
In the subgroup analysis by use of routine surfactant, (outcome 03-02) only one small trial of 51 infants (Clark 1992) reporting CLD at 36 weeks did not use surfactant. This trial showed a significant reduction in the HFOV group [RR 0.23 (95% CI 0.07, 0.73)]. This result was significantly different from the subgroup analysis of the 12 trials involving 2259 infants in which surfactant was used. The latter result is similar to the overall analysis of CLD at 36 weeks PMA [summary fixed effects RR 0.91 (95% CI 0.82, 1.01)] with persisting heterogeneity (I2 =58.5%).
Subgroups by use of different types of oscillator (flow interrupters, true piston oscillators or both) showed no statistical difference (overlapping 95% confidence intervals) between the summary RRs of the subgroups (outcome 04-02). For the subgroup of eight trials of 1353 infants that used of HF piston oscillators, there was a significant reduction in CLD in the HFOV group [summary RR 0.76 (95% CI 0.65, 0.90), RD -0.13 (95% CI -0.23, -0.02), NNT 8 (95% CI 4, 54)]. The summary RR remained significantly reduced when the 99% CI was used (99% CI 0.65, 0.95). There was significant heterogeneity (I2 = 68.2%). Using a random effects model, the RR was still significantly reduced [summary RR 0.67 (95% CI 0.47, 0.94)] but not when both random effect model and 99% CI was used [summary RR 0.67 (99% CI 0.42, 1.05)].
Some subgroups based on lung protective strategies (LPS) on CV (outcome 05-02) were different (95% confidence intervals do not overlap) between the summary RRs when a fixed effects model was used. Three of the four subgroups showed a moderate amount of heterogeneity (I2 greater than 50%). Using a random effects model no significant difference between the groups was demonstrated. In the two trials of 174 infants in which there was 'definitively no LPS on CV' criteria, there was a significant reduction in CLD in the HFOV group with moderate heterogeneity [summary RR 0.48 (95% CI 0.31, 0.75), RD -0.42 (95% CI -0.08, -0.01), I2 = 53.5%]. The difference remained significant when the 99% CI was used (99% CI 0.26, 0.87), but not when a random effects model was used due to wider confidence intervals [summary RR 0.42 (95% CI 0.18, 1.02)].
Subgroups by age at randomisation (less than 2 hrs, 2 - 6 hrs, greater than 6 hrs) showed no statistical difference (overlapping 95% confidence intervals) between the summary RRs of the subgroups (Comparison 06 - 02). The group of four trials of 782 surviving infants who were randomised at two to six hours of age showed a significant overall reduction in the risk of CLD with minimal heterogeneity [summary RR 0.72 (95% CI 0.59, 0.87), (99% CI 0.56, 0.92), I2 =23.3%].
Subgroups by inspiratory:expiratory time ratio on HFOV (I:E = 1:1, 1:2 or variable / unknown) showed no statistical difference (overlapping 95% confidence intervals) between the summary RRs of the subgroups (Comparison 07 - 02). The group of six trials of 829 surviving infants who were given HFOV using an I:E of 1:2 showed a significant overall reduction in the risk of CLD but with considerable heterogeneity [fixed effects summary RR 0.76 (95% CI 0.64, 0.90), (99% CI 0.61, 0.95), I2 =73.6%]. The random effects summary RR was also significantly reduced in the HFOV group at the 95% CI level (95% CI 0.41, 0.95) but not at the 99% level (99% CI 0.36, 1.09).
Death or CLD at 36 weeks postmenstrual age
There was a small reduction of the risk of the combined outcome of 'death or CLD at 36-37 weeks PMA or discharge' in the HFOV group [outcome 01-08, summary RR 0.93 (95% CI 0.86, 1.00)] which is of borderline significance using the fixed effects model. In view of moderate heterogeneity (I2 =57.7%), a random effects model was also used, yielding a nonsignificant difference in the summary RR [0.89 (95% CI 0.77, 1.03)].
Subgroup analyses
There was no statistically significant difference in death or CLD at 36 weeks postmenstrual age between the different categories within each of the subgroups (95% CIs overlap), except the one comparing inspiratory (I:E) ratios on HFOV. In this latter subgroup, the use of an I:E ratio of 1:2 was associated with a significantly lower rate of death or CLD [summary RR 0.08 (0.07, 0.91)] than was seen in the group with variable or unknown I:E ratio [summary RR 1.01 (092, 1.11)], but was not significantly different when compared with the group in which 1:1 ratio was used [summary RR 0.96 (0.72, 1.26)]. Within subgroups, some individual categories show significant effects and these are outlines below.
As for the outcome CLD alone, there was a significant overall reduction in death or CLD in the subgroup of trials using true piston oscillators [fixed effects summary RR 0.83 (95% CI 0.74, 0.94), RD -0.08 (95% CI -0.13, -0.03), NNT 12 (95% CI 8, 34)]. However, there was a persisting moderate heterogeneity (I2 = 56.8%), with a random effects summary RR of 0.78 (95% CI 0.63, 0.97).
In the subgroup of 2 trials of 190 infants with no lung protective strategy on CV, there was a significant reduction of death or CLD with HFOV [summary RR 0.56 (95% CI 0.38, 0.81), summary RD -0.221 (95% CI -0.36, -0.05), NNT 5 (95% CI 3, 19), I2 =0%].
In the subgroup analysis of age at randomisation, in the group of four trials of 944 infants with randomisation occurring at two to six hours of age there was a significant reduction in death or CLD with HFOV [summary RR 0.79 (95% CI 0.68, 0.91), summary RD -0.14 (95% CI -0.24, -0.04), NNT 7 (4, 26)] with nonsignificant heterogeneity (I2 =34.5%). The summary RR remains significantly reduced when the 99% CI was used (99% CI 0.65, 0.95).
In the subgroup of 6 trials involving 984 infants that used an I:E of 1:2 for HFOV, there was a significant reduction of death or CLD in the HFOV group [summary RR 0.80 (95% CI 0.70, 0.91, RD -0.11, (95% CI -0.17, -0.04, NNT 9 (95%CI 5, 23), I2 + 67.1%]. This difference was still significant using a random effects model [summary RR 0.72 (95% CI 0.54, 0.95)]
Duration of oxygen therapy
The duration of oxygen therapy was reported in seven trials. The statistical reporting of this outcome differed substantially between trials so meta-analysis was not undertaken.
Gerstmann 1996 found no significant difference in the duration of oxygen therapy in infants with birth weights of one kilogram or less, but a shorter duration of oxygen therapy in HFOV infants with birth weights over one kilogram [median days (95% CI), 13.2 (6.6, 24.3) vs. 27.6 (14.3, 37.7), P = < 0.05]. Van Reempts 2003 reported mean and standard deviations for days of oxygen that were similar in the two groups [HFOV 23.6 (28.2) vs. CV 22.7 (28.5)]. No significant difference in the median days of oxygen therapy between treatment groups was found in the three other studies [Thome 1998, 36 vs. 39.5; Plavka 1999, 20 (95% CI 1, 86) vs. 29 (95% CI 4, 107); Moriette 2001 22 (IQR 47) vs. 22 (IQR 41). Craft 2003 reported mean (and range) for days of oxygen therapy for the two subgroups by birthweight; 500 - 750 g, HFOV 75.5 (3 - 136) vs. CV 95.1 (3 - 196); 751 - 1000 g, HFOV 59.9 (1 - 119) vs. CV 53.0 (27 - 93). These differences were not statistically different. Vento 2005 reported the mean (SD) hours of oxygen therapy that was significantly lower in the HFOV group [760 (473) ] compared with the CV group [1445 (1297)], P = 0.03.
Use of mechanical ventilation
The use of mechanical ventilation at 28 - 30 days was reported in three studies and was not significantly different in individual trials or in the meta-analysis.
Seven trials reported the total duration of mechanical ventilation (MV). Overall, the trend was for shorter durations of ventilation in the HFOV groups, but no individual trials showed a significant difference. These data have not been combined in meta-analysis because of differences in the statistical reporting between trials.
In the Gerstmann 1996, trial the median (95% confidence intervals) days on MV in those with a birth weight less than 1 kg was 24.7 (95% CI 3.7, 61.4) in the HFOV group and 53.7 (95% CI 28.4, 103) in the CV group, a trend that was not significantly different. In this trial, there was also a similar median duration of MV in infants with birth weights over 1 kg [4.1 days (1.7, 6) in the HFOV group vs. 4.5 days (95% CI 3, 6.1) in the CV group]. Clark 1992 reported medians and ranges for the days on MV for all infants entered in the study that were not significantly different between the HFOV group [16 (95% CI 1.8, 67)] and the CV group [30.3 (0.5, 222)]. Ogawa 1993 reported similar mean (+/- SD) days of mechanical ventilation in the HFOV group (17.3 +/- 24.4) and CV group (13.5 +/- 21). Plavka 1999 reported means with 95% confidence intervals for duration of mechanical ventilation and no difference between HFOV and CV groups [5 (95% CI 1,70) vs. 7 (95% CI 3, 52)] was shown. Moriette 2001 found similar mean (interquartile range, IQR) duration of mechanical ventilation between HFOV and CV groups [9 (17) vs. 9 (16)]. Van Reempts 2003 reported similar mean and standard deviations of days of MV in the two groups [HFOV 7.7 (9.7) vs. CV 4.9 (9.1)]. Craft 2003 reported mean (and range) for days of mechanical ventilation for the two subgroups by birthweight; 500 - 750 g, HFOV 43.3 (1 - 136) vs. CV 59 (3 - 133); 751 - 1000 g, HFOV 37.7 (1 - 83) vs. CV 20.1 (1 - 56). These differences were not statistically different. Vento 2005 reported the mean (SD) hours of mechanical ventilation that were not significantly different between the HFOV group, 310 (313) and the CV group, 656 (981), P 0.15.
Failed treatment
Two trials reported failure to maintain gas exchange with the allocated treatment. Thome 1998 reported a non-significant trend towards more infants failing based on oxygenation index criteria in the HFOV group (7/140 vs. 4/144), while Gerstmann 1996 reported more failures with CV (1/64 vs. 9/64, P = 0.008).
Six trials reported crossover to the alternate treatment, a decision that was left to the judgement of individual clinicians. In the HIFI 1989 trial there was a significant increase of treatment failures (failure to maintain adequate gas exchange) in the HFOV group leading to crossover of treatment (85/346 in the HFOV group and 60/327 in the CV group, P = 0.01). Moriette 2001 reported a switch in ventilator mode for fewer infants assigned to HFOV than to CV [(15% vs. 29%), OR 0.43 (95% CI 0.24, 0.78)]. Johnson 2002 found the same rate of failure of assigned treatment (10% in each group), while Courtney 2002 reported that more infants exited the assigned mode of treatment in the CV group compared to the HFOV group (52/254 vs. 31/244 respectively, P = 0.02). Van Reempts 2003 reported 17 (11.6%) failures in the HFOV group and 10 (6.5%) failures in the CV group, a nonsignificant difference. In Durand 2001, two infants crossed over from HFOV and seven infants crossed over from CV at the discretion of clinicians. In Craft 2003, one infant crossed over from HIFI and none crossed over from SIMV. These data have not been combined in a meta-analysis as there were differences in definitions between trials and possibly in clinician uptake of the option to cross over.
Two trials had the additional failure criterion of PIE in the CV group. These trials reported crossover to be similar between groups (Rettwitz-Volk 1998, 8/46 vs. 9/50) or to be more common in the CV group (Clark 1992, 5/30 vs. 9/26, P = 0.01).
Pulmonary air leak syndromes
Ten trials involving 2726 infants reported 'any pulmonary air leak' (outcome 01-09). Two trials showed a significant increase in any air leak in the HFOV group [Thome 1998, RR 1.38 (95% CI 1.01, 1.89), Schreiber 2003, RR 1.67 (95% CI 1.15, 2.43)]. Overall analysis of the ten trials shows a small but significant increase in the HFOV group [summary RR 1.19 (95% CI 1.05, 1.34), RD 0.05 (95% CI 0.01, 0.08)].
Gross pulmonary air leak (excluding PIE alone) is reported for 1804 infants in nine trials (outcome 01-10). No individual trial showed a difference, but overall there is an increase in the HFOV group of borderline significance with no heterogeneity [summary RR 1.32 (95% CI 1.00, 1.72), RD 0.03 (95% CI 0.00, 0.06), NNT 35 (95% CI 18, 1000), I2 = 0%].
Subgroup analyses of gross pulmonary air leak
In the subgroup of eight trials of 908 infants using a HVS for HFOV, there was a significant increase in gross pulmonary air leak, [summary RR 1.36 (95% CI 1.03, 1.79)] with no heterogeneity (I2 = 0%). This difference did not reach significance when the 99% CI is used (0.94, 1.95). In the other subgroup analyses, there was no significant difference between subgroups (outcome 02-04).
Intraventricular haemorrhage (IVH)
Ten trials involving 2971 infants reported all grades of IVH (outcome 01 - 11). There was no significant difference in the rate of IVH of all grades between the treatment groups in individual trials or in the overall analysis [summary RR 1.05 (95% CI 0.96, 1.15)].
Fifteen trials involving 3585 infants reported the rates of the more severe grades of IVH, Grade 3 or 4 (outcome 01 - 12, subgroup). Two trials reported significantly higher rates in the HFOV group; the large HIFI 1989 study, which contributed most weight in the overall analysis [RR 1.41 (95% CI 1.06, 1.88)], and the trial by Moriette 2001 [RR 1.73 (95% CI 1.04, 2.87)]. Moriette 2001 reported an increased rate of severe IVH in the HFOV group, both in infants born at less than 28 weeks gestation (HFOV 26/81 vs. CV 15/72) and in infants born at 28 or 29 weeks gestation (HFOV 8/58 vs. CV 4/61). Overall, there was no significant difference in the rates of more severe grades of IVH between the HFOV and CV groups [summary RR 1.11 (95% CI 0.95, 1.30)].
In the subgroup the analyses of severe grades 3 or 4 IVH, no statistically significant differences were apparent between any of the categories within the groups. Some individual groups within the subgroup analyses showed increases in the rates of severe IVH. In the subgroup by use of high volume strategy for HFOV (outcome 02 - 05), the two trials (HIFI 1989; Rettwitz-Volk 1998) in which HVS was not used showed a significant increase in the risk of severe IVH [summary RR 1.45 (95% CI 1.09, 1.93), RD 0.074 (95% CI 0.02, 0.13), NNT 14 (95% CI 56, 8)]. The RR is of borderline significance when the 99% CI is used (1.00, 2.11). There was a significant increase in the rate of grade 3 or 4 IVH in the subgroup analysis of two trials (HIFI 1989; Clark 1992) not using surfactant replacement therapy [summary RR 1.36 (95% CI 1.03, 1.79), RD 0.07 (95% CI 0.01, 0.13), NNH 15 (95% CI 143, 8)]. Most of the weight in these latter two analyses was contributed by HIFI 1989.
Periventricular leukomalacia ( PVL)
PVL was reported for 3474 infants in 13 studies. There was a nonsignificant trend towards an increased rate with HFOV in the HIFI 1989 [RR 1.61 (95% CI 0.99, 2.60)], but no significant difference overall [summary RR 1.10 (95% CI 0.85, 1.43)] (outcome 01 - 13).
In the subgroup analyses, there were no significant differences between categories within the subgroups (95% CIs overlap).
In the subgroup by use of high volume strategy for HFOV (outcome 02 - 06), the two trials (HIFI 1989; Rettwitz-Volk 1998) in which HVS was not used show a significant increase in the risk of PVL [summary RR 1.64 (95% CI 1.02, 2.04)]. This was not significant at the 99% CI level (0.88, 3.06).
In the subgroup of 2 trials in which lung protective strategies on CV were not used (HIFI 1989, Gerstmann 1996), there was a significant increase in PVL in the HFOV group [RR 1.57 (95% CI 0.99, 2.48)]. This was not significant at the 99% CI level (0.86, 2.86).
Most of the weight in these latter two analyses was contributed by HIFI 1989.
Retinopathy of prematurity (ROP)
Ten trials with 2367 surviving infants report significant ROP (grade 2 or more). The overall analysis showed a significant decrease in the HFOV group with no heterogeneity [summary RR of 0.85 (95% CI 0.74, 0.99), RD 0.04 (95% CI 0.07, 0.01), NNT 30 (15, 357), I2 = 0%] (outcome 01 - 14).
Pulmonary function tests, symptoms and growth at follow-up.
No significant differences in pulmonary function test results were found during the neonatal period (Abbasi 1991) or at discharge (Gerhardt 1989) in subgroups of infants from individual centres in the HIFI 1989.
Long-term follow-up assessments (in 82% of survivors), including pulmonary function tests (in 43% of survivors from seven of the ten centres), were carried out at nine months corrected age in infants from HIFI 1989 (The HIFI Study Group 1990a). There were no significant differences in respiratory function tests (compliance, resistance, lung volumes) or in the incidence of respiratory tract infections, hospital re-admissions, respiratory symptoms and signs (retractions and episodes of wheezing) or in growth.
Twelve month follow-up of patients in the Ogawa 1993 trial showed persistence of abnormal fibrous or emphysematous shadows on chest x-ray in two of the infants in the HFOV group and four in the CV group.
Eighty seven percent of the infants in Gerstmann 1996 were followed up at a mean age of 6.4 years. Improved respiratory function tests (decreased peak expiratory flow, increased residual lung volume, maldistribution of ventilation) were found in the HFOV group, but there were no significant differences in symptoms (pulmonary illness, asthma, hospitalisation) between the groups.
Of 185 survivors from 12 centres in Johnson 2002, 149 were invited for respiratory function tests and these were successfully carried out in 76 at 11 - 14 months of age (Thomas 2004). No differences were found between the HFOV and CV groups in any of the measures (functional residual capacity, inspiratory and expiratory resistance, respirator rate). Respiratory symptoms, treatments and growth were assessed at two years of age (Marlow 2006) and there were no differences between the HFOV and CV groups.
A two years of age assessment of 138 (82%) of survivors in the NOVA study (Schreiber 2003 - re-analysed by type of ventilation) revealed no difference in the mean height, weight or head circumference between the HFOV and CV groups.
Neurodevelopmental outcomes at follow up.
Neurodevelopmental status at follow-up was reported for six studies (HIFI 1989; Ogawa 1993; Gerstmann 1996; Johnson 2002; Van Reempts 2003; Schreiber 2003). The age and methods of assessment varied between studies so the results are presented in the text and not analysed by meta-analysis.
Neurodevelopmental status was assessed at 16 to 24 months corrected age in 77% of survivors of the HIFI 1989 study (185 HFOV & 201 CV) using Bayley psychometric tests and central nervous system examinations (The HIFI Study Group 1990b). The rate of moderate to severe abnormality (Bayley's scores more than one SD below the mean or neurological abnormality) was higher in the HFOV group [RR 1.28 (95% CI 1.02, 1.60)]. The rate cerebral palsy was 11% in both groups. There was an increase in the rate of hydrocephalus in the HFOV group [RR 2.08 (95% CI 1.07, 4.06)]. Using logistic regression, abnormal neurological status was shown to be associated with the increased rate of severe grades 3 or 4 IVH in this study.
One year follow-up in the trial by Ogawa 1993 showed no significant difference in motor and/or mental development, although the method of neurological assessment was not given.
Gerstmann 1996 reported neurodevelopmental status at a mean of 6.4 years for 87% of the infants. Assessment of mental function, using the Wechsler Scale for Children, and motor function, using the Bruinink-Oseretsky test showed no significant difference in mean scores between the two groups.
Johnson 2002 reported neurodevelopmental outcomes at 22 - 28 months (corrected for prematurity) based paediatric report for 73% of survivors and on parent questionnaires for 49% of survivors. No difference between HFOV and CV groups were found.
Van Reempts 2003 followed up a subgroup of infants who were less than 30 weeks gestation or 1250 grams at birth, or had intracranial lesions on ultrasound. This included 70 infants in the HFOV group and 68 in the CV group, representing 57% and 51% respectively of survivors in the whole trial. Bayley motor and mental developmental indices, as well as motor diagnoses, were assessed at seven to twelve months corrected age. There was no significant difference between the groups, with 60% of HFOV infants and 70% of CV infants being completely normal. Follow-up of only the 'abnormal' infants at 18 - 24 months corrected age revealed none of the infants in the HFOV group and four of the infants in the CV group were persistently abnormal, which was not statistically different.
Schreiber 2003 re-analysed the follow-up data from the NOVA study according to mode of ventilation. Of the 168 survivors to two years of age (84 in each group), data were available for 66 (78.6%) of those in the HFOV group and 72 (85.7%) in the CV group. Based on blinded assessments using Bayley's Scales (mean scores and number with scores < 70) and Pediatric neurological assessment, there were no differences between the groups.
Length of stay and hospital costs
The total hospital costs from a subgroup of patients from one centre in Gerstmann 1996 suggested that the median hospital costs were less in 42 patients randomised to HFOV compared with 41 in the CV group. In this trial, similar differences were found for those infants with birth weights of one kilogram or less and those of more than one kilogram. There were no significant reductions in the median length of hospital stay or in median duration of IPPV in this trial nor in Rettwitz-Volk 1998 and Clark 1992, although the trend in each case was towards a reduction in the HFOV group. Johnson 2002 reported similar median and range of days hospital stay in survivors between treatment groups (HFOV 94, 73-114; CV 89, 70-112 ).
Other outcomes
Outcomes by birth weight and gestational age have been variably reported in the trials. This important subgroup analysis will be attempted in a future update, following author contributions to an individual patient data analysis that is currently underway (principal investigator Filip Cools).
Use of surfactant was not a prespecified outcome in this review. Three trials (Gerstmann 1996; Plavka 1999; Moriette 2001) reported less use of surfactant in the group receiving HFOV. In four trials there was no significant difference in surfactant use (Durand 2001; Courtney 2002; Johnson 2002, Van Reempts 2003).
Discussion
In this review, the search revealed 15 trials that met prespecified eligibility criteria, four trials that were excluded, one new trial awaiting full assessment and another yet to be published. It is possible that there are other trials that have not been published or were published in a language not covered by this systematic review. The reviewers would be most interested in hearing of other published, unpublished or ongoing trials.
Limitations of this review
The studies have been carried out over a long time period (20 years) during which changing obstetric and neonatal practices may have influenced the conditions under study such as RDS, IVH and CLD. Participants in early trials could be up to 34 weeks gestational age or 2000 g birth weight, whereas recent trials have been confined to infants of less than 30 weeks gestational age or less than 1200 g birth weight.
Interventions varied by type of ventilator and strategy used for HFOV and CV. Over time it more likely that HFOV was delivered using a HVS, which would be likely to improve the effect of HFOV, while CV is more likely to be delivered using lung protective strategies, which could reduce the comparative effectiveness of HFOV. Lung protective strategy on CV to prevent CLD is difficult to define. There are variable maneuvers that principally affect acute lung injury rather than CLD. In this review, four categories were used to evaluate trials that used most strategies ('definite LPS') compared with the other extreme of none ('definitively no LPS') and two intermediate groups. This summary data is based on mixed, soft evidence and might be able to be explored further in the proposed individual data analysis currently under way.
The quality of the studies was generally high, as all attempted to conceal the randomisation process. However, the interventions were not blinded in any study and this could be associated with bias regarding the use of co-interventions and the ascertainment of outcomes, such as duration of mechanical intervention and oxygen therapy. Ascertainment of outcomes was generally complete or made so by author clarification. Since the treatment could not be blinded in any study, outcomes that were caregiver dependent, such as the duration of oxygen therapy or diagnosis of CLD, may be less valid.
Pulmonary outcomes
The overall analysis of CLD at 28 - 30 days is dominated by the HIFI 1989 trial, which is the largest. Soon after the completion of this study, it was criticized because the methodology used to apply HFOV did not include methods to recruit lung volume (Froese 1991). This criticism is partly supported by the results of subsequent trials that used a high volume strategy where there was a significant reduction in CLD at 28 - 30 days of age (Clark 1992; Gerstmann 1996). HIFI 1989 did not report the rates of CLD at term equivalent age or discharge and overall analysis of the remaining trials showed no significant reduction in this outcome with HFOV.
The interventions (treatment and control) varied from trial to trial. Jouvet (Jouvet 1997) found that HFOV generated by a ventilator using flow interruption (e.g. Drager Babylog) was less powerful than HFOV generated by a ventilator using a piston (e.g. Sensormedics), so that there was an inability to increase tidal volume when pressure amplitude was increased above 50%. None of the studies using flow interruption rather than piston oscillation found a difference in the incidence of chronic lung disease.
Although there were no statistically significant differences in the other subgroup analyses of CLD, there were some specific groups of trials which showed a significant reduction in CLD with HFOV. The explanations for this may not be clear. For example, randomisation at 2 - 6 hrs of age compared with 0 - 2 hrs may have included infants with more definite lung disease, rather than a mixed group including those with hypoventilation at birth. Many factors may have been interacting, such as use of antenatal corticosteroids, use of surfactant, use of piston oscillators for HFOV, use of high volume strategy, use of lung protective strategies on CV, and use of inspiratory:expiratory ratio of 1:2. Although there may be biological plausibility for these factors more research is required to clarify the effectiveness of HFOV. The individual patient data review could examine these multiple variables.
Although there were no significant differences in any individual trials, overall, pulmonary air leaks occurred more frequently in the HFOV group.
Other reviews of the evidence of effectiveness of HFV (both oscillation and jet ventilation) also found that CLD was not reduced when HVS was not used for HFV and/or LPS was used on CV (Bollen 2003; Thome 2005).
Neurodevelopmental outcomes.
Increases rates of IVH or PVL occurred in some individual trials but not overall. The pathophysiological factors that might have led to an increased rate of IVH or PVL are not certain. The authors of HIFI 1989 suggested that the nearly constant high mean airway pressure during HFOV might restrict venous return, increase intracranial venous pressure, and decrease cerebral blood flow. However, animal studies (Kinsella 1991) and human studies (Laubscher 1996) failed to show these cardiovascular changes. The latter study reported that cardiac output fell when on HFOV. In a single centre involved in the study of Johnson 2002, echocardiography was carried out in 45 infants (Osborn 2003). Superior vena cava flow was reduced (< 50 ml/kg/min) in more HFOV (48%) than CV (20%) infants, but this difference was not significant. Cambonie 2003 examined the haemodynamic changes during HFOV vs. CV and found no difference in cardiac function but did find a lower end diastolic velocity and a higher resistance index in the anterior cerebral artery.
The tendency for higher rates of IVH or PVL found in this review in association with failure to use HVS was also shown in two other reviews of the evidence of effectiveness of HFV (both oscillation and jet ventilation, Bollen 2003; Thome 2005) and in a review of elective jet ventilation vs. CV (Bhuta 2003). Failure to recruit lung volume and the consequent cardiorespiratory instability has been implicated (Froese 1991). Whether it was one of these mechanisms or just lack of experience with a new technology at the time is difficult to say. The large HIFI 1989 dominated this analysis.
In five of the six trials reporting long term neurodevelopmental outcome, no difference was apparent although in some studies there was considerable loss to follow-up.
Research questions raised by this review include:
1. Are there differences in pulmonary outcomes and adverse effects by type of ventilator used to generate HFOV? The question would be answered best by a head to head trial of HFOV using a true oscillator vs. a flow interrupter.
2. What is the long term growth and development of infants treated with HFOV vs. CV? This could be answered by follow-up of infants enrolled in existing trials.
3. Are there differences in the costs compared to benefits of HFOV? One small study (Gerstmann 1996) suggested that HFOV reduced costs of care.
4. Despite increasing the number of subgroup analyses in this update of summary data from trials, marked heterogeneity persists. To further explore the comparison of HFOV and CV, a collaborative study is underway to review individual patient data obtained from the trials using a prespecified protocol for analysis. If you have randomised controlled trial data on this topic and wish to join the collaboration, contact Filip Cools (filip.cools@az.vub.ac.be).
Reviewers' conclusions
Implications for practice
There is no clear evidence that elective HFOV compared with CV offers important advantages when used as the initial ventilation strategy to treat preterm infants with acute pulmonary dysfunction. There is no evidence of a reduction in death rate. There may be a small reduction in the rate of CLD with HFOV use, but the evidence is weakened by the inconsistency of this effect across trials and is not significant overall. Adverse effects on short term neurological outcomes have been observed in some studies, but these effects are not significant overall. Most trials reporting long-term outcome have not identified any difference.
Implications for research
Any future trials on elective HFOV should target those infants who are at most risk of CLD (extremely preterm infants), compare different strategies for generating HFOV, and report important long-term pulmonary and neurodevelopmental outcomes. Economic analysis should also be incorporated.
Acknowledgements
Authors of the following trials Clark 1992; Ogawa 1993; Gerstmann 1996; Rettwitz-Volk 1998; Thome 1998; Plavka 1999; Moriette 2001; Johnson 2002; Van Reempts 2003, kindly provided additional information about their studies. Michael Schreiber kindly re-analysed the data from the NOVA study (Schreiber 2003) and its follow up results according type of ventilation.
Potential conflict of interest
None
Characteristics of included
studies
| Study | Methods | Participants | Interventions | Outcomes | Notes | Allocation concealment |
| Clark 1992 | Concealment of randomisation - yes (blind draw of cards); Blinding of treatment - no; Complete follow up - yes (after additional data from author); blinding of outcome assessment - unknown | Single centre; RDS & gestational age <36 weeks & birth weight <1751 gms & age <24 hrs; stratified by birth weight <1001 / 1001 vs 1750 gms and by age 0 - 12 vs 12 - 24 hrs, in blocks of 5 per category. 152 eligible, 98 (63%) enrolled: 78% inborn; RDS chest Xray score at entry HFOV > CV; 15 post randomisation exclusions in publication - data retrieved from author. | HFOV [Sensormedics 3100, 10 HZ, IT 0.33 (1:2), MAP 1-2 cms > CV]. HVS used (higher MAP, wean FiO2 first)
CV [IT 0.3 - 0.6 sec, 25 - 40/min, PEEP 4-6 cms H2O, PIP 20 - 27 cms H2O]. CO2 target 35 - 55 mmHg.
Mean age at randomisation, HFOV 7 vs CV 9 hrs. | Chronic lung disease (CLD) = oxygen therapy at 30 days + abnormal chest Xray; oxygen therapy at 36 weeks postmenstrual age; failure of assigned treatment to maintain PaO2 >50 mm Hg or PaCO2 < 60 mm Hg or in CV group development of pulmonary air leak; Pulmonary air leak (+/- pneumothorax); All IVH; grades 3 or 4 IVH; mortality at 30 days | No surfactant; prenatal corticosteroids in 12% of HFOV and 13% of CV: additional arm to the trial consisted of HFOV for 72 hrs then switch to CV (not analysed here). | A |
| Courtney 2002 | Concealment of randomisation - yes (central randomization); blinding of treatment - no; complete follow up - yes for early outcomes, 4% loss in HFOV and 2% loss in CV by 36 wks PMA;
blinding of outcome assessment - yes for head ultrasounds, not specified for other outcomes. | Multicentre (26); 494 preterm infants with birth weights of 601 to 1200 gms which were appropriate for gestational age, less than four hrs of age, had received one dose of surfactant, required IPPV, FiO2 0.25 or more, MAP 6 cms H2O or more.
Exclusions - Apgar score at 5 min of less than 4 or base deficit more than 14, congenital abnormality.
HFOV group - 245 randomized, 1 excluded due to cong. heart disease, 10 late exclusions due to parental request (data used for early outcomes).
CV group - 255 randomised, 1 excluded due to cong. heart disease, 4 exclusions due to parental request (data used for early outcomes). | HFOV [SensorMedics 3100A, 10-15 HZ, IT 0.33, initial MAP 2 cm H20 > than CV.
CV - synchronized intermittent mandatory ventilation with VIP Bird or Draeger Babylog 800 or Bear Cub with volume monitor or Bear Cub 750vs; VT 4 - 7 ml/kg, IT 0.25 - 0.40 sec, rates <60/min. PaCO2 target 45 - 60 mm Hg.
Randomised at mean age of 2.7 hrs in each group. | Death by 36 weeks PMA, chronic lung disease at 36 weeks PMA (oxygen therapy or other assisted ventilation), IVH, PVL, pneumothorax, ROP grade 2 or more, NEC, duration of IPPV. | Surfactant and prophylactic indomethacin used in all; prenatal corticosteroids given in 74% of HFOV cases and 71% of CV cases | A |
| Craft 2003 | Concealment of randomisation - yes.
Blinding of treatment - no
Completeness of followup - yes
Blinding of outcome assessment - no for CLD, unknown for IVH | 46 preterm infants 23 - 34 weeks & <1000gms birth wt.
Two centres | HFO - Infant Star 10-12 HZ, high volume strategy.
CV - Infant Star, 'open lung strategy (PEEP 4-6, PIP 16-24, SIMV. PaCo2 target 50 - 60 mm Hg.
Age at randomisation not reported. | CLD at 36 weeks PMA - oxygen required to maintain SaO2 >92%, death, IVH grades 3 or 4, Airleak, Retinopathy of prematurity,
failure leading to cross-over of ventilation type | Jan. 1999 - may 2000. trial stopped because of lack of effect.
Full course of antenatal corticosteroids given to 50% in each group | A |
| Durand 2001 | Randomised but concealment of randomization - unknown
Blinding of intervention - no.
completeness of followup - 2 infants withdraw from HFOV arm at parent request.
Blinding of outcome assessment - no | 48 preterm infants with birth weights 501 - 1200 gms, < 4 hrs of age, had one dose of surfactant, on mechanical ventilation, MAP =or> 6 cms H2O, ongoing ventilation for >24 hrs anticipated.
7 nurseries involved | HFOV - Sensormedics 3100A, 15 HZ, I/T 0.33, high volume strategy.
CV - SIMV using Drager Babylog, Bearcub, VIP Bird - lung protective strategy - Rate <60, PEEP 4-6, Ti 0.25-0.35, CO2 target 40 55 or higher. | Death by 36 weeks, CLD at 36 weeks in survivors, IVH grades 3 or 4, PVL, mean no. of doses of surfactant. | Pilot study for Courtney 2003 - subjects not include in later study. | B |
| Gerstmann 1996 | Concealment of randomisation - yes (sealed opaque envelopes) in 2 tiered balanced blocks; blinding of treatment - no; complete follow up - yes; blinding of outcome assessment - no. | Multicentre (3); <35 weeks gestation and respiratory distress with abnormal chest Xray consistent with poor inflation and use of IPPV and < 12 hrs of age; 125 ( approx. 63 % of eligible) subjects enrolled; stratified by birth weight more or less than 1 kg and by age more or less than 4 hrs; | HFOV (Sensormedics 3100, insp/exp 0.33, 10 - 15 Hz, airway pressure > CV). HVS used (higher MAP, wean FiO2 first)
CV (IT 0.35 - 0.55 sec, rates <60/min, PEEP 3 - 7 cms H2O, PIP up to 30 cms H2O if <1 kg and up to 35 cms H2O if > 1 kg); crossed over to other treatment if met set failure criteria. Mean age at randomisation 2.9 vs 2 hrs. | Chronic lung disease (CLD) = oxygen therapy at 30 days & abnormal chest Xray; oxygen at discharge (mean age 37 weeks PMA); mortality at 30 days; failure of assigned treatment (PaO2 <50 or PaCO2 >60 mmHg for > 2 hrs, or excessive pressures of IPPV); pulmonary air leak; all IVH; grade 3 or 4 IVH; PVL; mechanical ventilation at 28 days; NEC; use of vasopressors; PDA (treated); ROP; BAER; hospital cost | Bovine surfactant used in about 70%; prenatal steroid use 29.7% in HFOV and 18% in CV; original design had 3 arms, including a HFOV without surfactant arm; interim analysis after 50 subjects | A |
| HIFI 1989 | Concealment of randomisation - yes; blinding of treatment - no; complete follow up - yes for primary outcome (CLD, 98.3%), lower for late outcomes (see below); blinding of outcome assessment - yes | Multicentre (10); RDS & birth weight 750 - 2000 gms (those at 1250 - 2000 gms only eligible if severe RDS) & < 24 hrs of age & IPPV for < 12hrs; stratified by centre and in 250 gms weight groups in those at 500 - 1500 gms; 823 eligible, 673 randomised, 12 withdrawals (died or consent withdrawn before treated); exclusions - meconium aspiration, neuromuscular conditions, hydrops, congenital heart disease, congenital abnormalities, multiple births of 3 or more. | HFOV [Hummingbird, 15 HZ, MAP same or below CV] vs CV [20 - 40 /min, IT 0.3 - 1.0 sec, PIP 20 - 25 cms H2O, PEEP 2 - 5 cms H2O]. Mean age at randomisation 5.8 vs 6.1 hrs in HFOV and CV groups. | Chronic lung disease (CLD) = oxygen therapy at 28 days & abnormal chest Xray; mortality at 28 days; pulmonary air leak (+ / - pneumothorax); all IVH; grade 3 & 4 IVH; PVL; mechanical ventilation at 28 days; failure of assigned treatment (PaO2 < 45 mmHg or PaCO2 > 65 mm Hg; NEC; use of vasopressors; pulmonary function at 9 months (432, 82% of survivors); neurodevelopmental outcome at 16 - 24 months (386, 74% of survivors). | Surfactant not used; rate of prenatal corticosteroid usage not reported. | A |
| Johnson 2002 | Concealment of randomisation - unclear; blinding of treatment - no; complete follow up - yes; blinding of outcome assessment - no for primary outcomes, yes for head ultrasounds. | Multicentre (25); 870 infants 23 to 28 weeks inclusive. Randomised immediately before the birth. 33 infants in each group subsequently did not meet eligibility criteria and were not continued in the trial. Eligibility criteria included - intubated from birth for respiratory support, < 1 hr of age.
Exclusions - congenital abnormality or needing transfer out.
Of 804 eligible infants 7 withdrawn (?groups) leaving 400 in HFOV group and 397 in CV group. | HFOV [SLE 2000 HFO - 187 infants, Drager Babylog 8000 - 165 infants, SensorMedics 3100A - 38 infants]; 10 HZ, MAP 6-8 cms H20; I:E 1:1 or 1:2, FiO2 weaned before MAP (high volume strategy)
CV [SLE 2000 - 193 infants, Drager Babylog 8000 - 192 infants, other ventilators - 12 infants]; IT 0.4 sec, initial rate 60/min, target PaCO2 34-53 mm Hg, Au: most on synchronised ventilation. | Death by 36 weeks PMA, chronic lung disease at 36 weeks PMA (oxygen therapy or other assisted ventilation), failure of assigned treatment, IVH, PVL, pulmonary airleak (not defined), ROP grade 2 or more, NEC, length of hospital stay. | Surfactant given to 97% of HFOV group and 99% of CV group.
Prenatal corticosteroids given in 91% of HFOV cases and 92% of CV cases. | B |
| Moriette 2001 | Concealment of randomisation - yes (central randomization); blinding of treatment - no; complete follow up - yes (7% loss); blinding of outcome assessment - yes for head ultrasound and chest xrays, no for other outcomes. | Multicentre (10); 292 infants 24 - 29 weeks with clinical and radiological RDS and PaO2/Fio2 < 200 mm Hg randomized, 273 analysed (139 HFOV and 134 CV).
Exclusions: congenital abnormalities, PPROM >24 hrs, hydrops, grade 3/ 4 IVH or pulmonary air leak before entry.
Age < 6hrs (median 142 mins in HFOV and 145 mins in CV). | HFOV with piston oscillator (OHFI, Dufour, France), 1:1 I:E ratio, 15 hz, high volume strategy (higher mean airway pressure, sighs); vs CV with Drager babylog 8000, TI < 0.45 sec, PEEP 4-5 cms H2O, SIMV, 77%.
Use of alternative mode in 1st 10 days if MAP > 14 cms H2O in HFOV gp or after surfactant FiO2 > 0.5 &/or PIP >25 in CV gp | Death (neonatal and before discharge);
Use of > 1 dose of surfactant;
Pulmonary airleak (PIE and pneumothorax);
ROP (? grade)
CLD (oxygen at 28 days and oxygen at 36 weeks;
Duration of IPPV, O2 therapy, hospitalisation
Grade 3/4 IVH (7-10 day U/S);
PVL (28 day U/S);
| All received 1 dose of surfactant; maternal antenatal corticosteroids in 52% HFOV and 55% CV 21 | A |
| Ogawa 1993 | Concealment of randomisation - yes (opaque sealed envelops); blinding of treatment - no; complete follow up - yes; blinding of outcome assessment - yes | Multicentre (9); Presumed RDS; 750 - 2000 gms; <1 hr of age for inborn and <6 hrs for outborn (mean 2 +/- 1.6 vs 1.7 +/- 1.5 hrs); stratified by birth weight 750 - 1249 vs 1250 - 2000 gms; 118 admissions, 16 met exclusion criteria (as for HIFI 1989); 46 allocated to each treatment. | HFOV (Hummingbird, 15 Hz). HVS used (higher MAP, sighs).
CV (pressure limited time cycled, method not stated). PaCO2 target 35-50 mm Hg.
Mean age at randomization HFOV 2 vs CV 1.7 hrs. | Primary outcome all IVH and grade 3 or 4 IVH; Chronic lung disease (CLD) = oxygen therapy at 28 days & abnormal chest Xray; mortality at 28 days; failure of assigned treatment (as for HIFI 1989); pulmonary air leak; PVL; mechanical ventilation at 28 days; duration of mechanical ventilation; neurodevelopmental outcome at 12 months (all survivors). | Bovine surfactant given for RDS as rescue | A |
| Plavka 1999 | Concealment of randomisation - yes (sealed envelopes); blinding of treatment - no; completeness of followup - 2 excluded (1 CNS abnormality in HFOV gp. and 1 congenital heart disease in CV); blinding of outcome assessment - not stated for most outcomes, chest xrays reviewed by blinded observers. | Single centre; 43 preterm infants <31 weeks and 500 - 1499 gms birth weight. Exclusions - small for gestational age, major congenital abnormality, neuromuscular condition or ventilated for CNS disorder or circulatory reason. | HFOV (Sensormedics 3100A) at 15 HZ, high volume strategy (high MAP and FiO2 weaned before pressure) vs CV (Bearcub 2100 or Infant Star) time cycled, pressure limited, + or - patient triggered, rate 30 - 60, IT 0.3 - 0.5, PEEP 3-5. | Mortality at 30 days and at 36 weeks PMA, any airleak, pneumothorax, CLD 30 days and 36 weeks PMA, any IVH and severe grade 3 or 4 IVH, periventricular leucomalacia, retinopathy > gd 2 | Selective intubation at birth, chest xray and surfactant treatment < 3 hrs, randomised < 3hrs
Author provided additional data on rates of IVH and pulmonary air leaks in excluded early deaths | A |
| Rettwitz-Volk 1998 | Concealment of randomisation - yes (central computer); blinding of treatment - no; complete follow up - yes; blinding of outcome assessment - no | Multicentre (3); preterm infants birth weight 750 - 1500 gms (stratified > or < 1000gms) and < 2 hrs old and RDS with FiO2 > 0.6; exclusions - Congenital abnormalities, hydrops. 46 in HFOV gp and 50 in CV gp. | HFOV Stephan SHF 3000 piston oscillator, 15-20 Hz, not HVS.
CV using time cycled pressure limited ventilators, IT 0.25 - 0.45, I:E = 1:2, PEEP 3-4.
Mean age at randomisation 70 vs 40 mins. | Mortality before discharge, CLD (O2 at 37 weeks PMA), failure of assigned treatment (PaO2 <45 mmHg or PaCO2 > 60 mm Hg), pulmonary ALS +/- pneumothorax, IVH, PVL | Bovine surfactant used as rescue in all; antenatal corticosteroids in 71%, 92% inborn; all patients still on oxygen therapy at 7 days of age received a 21 day course of Dexamethasone (HFOV 43% vs CV 60%). Cross over from CV to HFOV also allowed if PIE developed. | A |
| Schreiber 2003 | Randomised but concealment unclear.
Blinding of treatment - no.
Completeness of follow up - yes for primary analysis, 82% for developmental follow up.
Blinding of outcome assessment - yes for chest xray, head ultrasound, ROP, neurodevelopment.
| 207 preterm infants <34 weeks gestation and birthweight <200gms, <72 hrs of age, with RDS and IPPV to be given.
| Trial randomised infants to Nitric oxide vs placebo and to HFOV vs CV.
HFOV 102 infants - Sensormedics 3100A, 10-15 hz.
CV - 105 infants, Ventilator type ?, rate 40/min, PEEP 4-6cms H2O. PaCO2 target 35 - 55 mm Hg. | Death, CLD at 28 days and 36 week PMA, pulmonary air leak, severe IVH grds 3 or 4, PVL, ROP | Antenatal steroid rate 55%, all recieve surfactant | B |
| Thome 1998 | Concealment at randomisation - yes (consecutively numbered, sealed opaque envelopes); blinding of treatment - no; complete follow up - yes (98.3%); blinding of outcome assessment - yes for chest xrays, no for head ultrasound. | Multicentre (6); preterm < 30 weeks gestational age (stratified 24-25, 26-27, 28-29 wks) and intubated for IPPV < 6 hrs; exclusions - outborn or cong. abnormality. 140 in HFOV gp and 144 in CV gp. | HFOV with Infant Star ventilator (software version 83) at 10 Hz. HVS used (higher MAP, wean FiO2 first, sighs).
CV with various time cycled pressure limited ventilators, initial rates 60 - 80/min, aimed at lower PIP and PEEP 3 cms H2O or more.
Age at randomisation < 1 hr in all but 2 infants. | Failure (ALS < 10 days, oxygenation index > 35 , 40 or 45 in the 3 gestation strata, CLD at 36 weeks or death before discharge), CLD = oxygen or vent. support at 36 weeks, ALS = PIE or gross air leaks; IVH; PVL; ROP | Bovine or porcine surfactant given to 68% of HFOV and 71% of CV; prenatal corticosteroids in 86% of HFOV and 81% of CV. Postnatal corticosteroids given to 39% of HFOV vs 41% of CV. | A |
| Van Reempts 2003 | Concealment at randomisation - yes (sealed folded papers); blinding of treatment - no; complete follow up - yes; blinding of outcome assessment - yes for grading of chronic lung disease, intracranial hemorrhage, periventricular leukomalacia and retinopathy of prematurity. | 300 infants (147 HFOV and 153 controls) born at <32 weeks gestation, less than 6 hours of age, FiO2 >0.40 or MAPXFiO2 >3.8, clinical and radiological diagnosis of RDS.
Exclusions - major congenital abnormality, active infection. | HFOV using a high volume strategy (higher mean airway pressure than CV, wean O2 before pressure) using Sensormedics 3100A (122 infants) or Infant Star (25 infants) - MAP 8 cms H2O if <29 weeks & 10 cms H2O if 29-31 weeks. Rate 10 hz.
CV - Drager Babylog (73 infants), Infant Star (80 infants) - PIP=20 cmsH2O (aim low), PEEP 4 cms H2O start, IT <.35 start, rate 80/min, PaCO2 target 35 - 70 mmHg. I:E=1:1.1 | Chronic lung disease (CLD - on O2 or assisted ventilation) at 36 weeks, death before discharge, failure of assigned treatment, CLD at 28 days, pulmonary interstitial air, pneumothorax, intraventricular haemorrhage, periventricular leukomalacia, retinopathy of prematurity, days of IPPV/CPAP/O2, developmental outcome in early childhood for infants <30 weeks or with an abnormal head ultrasound. | All infants given surfactant; prenatal corticosteroids given to 63% in HFOV group and 66% of CV group
Author provided additional information on grades of ROP, prenatal steroids and neonatal mortality. | A |
| Vento 2005 | Concealment of randomization - yes.
Blinding of intervention - no.
Completeness of follow up - two infants (one from each group) excluded after randomisation due to diagnosis of congenital pneumonia.
Blinding of outcome assessment - unknown | 42 infants with birthweights 501 - 1500gms and gestational age 24 - 29 weeks.
All required intubation at birth and required ongoing ventilation.
Exclusions - congenital abnormalities, congenital pneumonia. | HFOV - via flow interrupter (Drager Babylog 8000+), high volume strategy, 10HZ.
CV - Draeger Babylog, SIMV, PEEP 4-6 cm, TI 0.30 - 0.40, Max. rate 60/min, PIP weaned first,.
In both CO2 target 45 - 55 mmHg.
Interventions commenced after randomization at 30mins of age. | death before discharge, CLD (O2 therapy at 36 weeks PMA), pneumothorax, PIE, IVH grades 3 or 4, PVL, ROP >stage 2. | Antenatal corticosteroids - any 100% HFOV & 95% CV, completed course 55% HFOV & 60% CV. | A |
IT = inspiratory time; PIP = positive inspiratory pressure; PEEP = positive end-expiratory pressure; MAP = mean airway pressure; CLD = chronic lung disease; ALS = air-leak syndrome; IVH = intraventicular haemorrahge; PVL = periventricular leukomalacia; PMA = post-mentrual ageCharacteristics of excluded studies
| Study | Reason for exclusion |
| Cambonie 2003 | |
| Froese 1987 | After randomization of infants (unknown gestation range), 5 of 11 in the HFOV group and an unknown number from the CV group were excluded from the comparisons between treatments. |
| HiFO 1993 | Rescue treatment with primary aim of preventing pulmonary air leak. |
| Lombert 1996 | 22% excluded after randomization, mixed population of preterm and term infants. |
| Pardou 1993 | Results reported for only 13 (54%) of the 24 subjects randomised to high frequency flow interrupter or CV. |
| Ramanathan 1995 | Mandatory crossover of treatments at 96 hrs. |
Characteristics of ongoing studies
| Study | Trial name or title | Participants | Interventions | Outcomes | Starting date | Contact information | Notes |
| Texas Infant Star | Texas infant Star | Eligible infants include < 1250 gms birth weight or < 29 weeks gestation. | Randomization to 3 modes of ventilation: conventional, high frequency oscillation, and combination (HFOV + 2 - 5 bpm CV). | | Study commenced in late 1996 - has been completed but not yet published. | Contact: Dr Anthony L Talbert, Texas Tech University School of Medicine, Odessa, Texas, USA. Phone +1 915 335 5270. | |
References to studies
References to included studies
Clark 1992 {published and unpublished data}Clark RH, Gerstmann DL, Null DM, deLemos RA. Prospective randomized comparison of high-frequency oscillatory and conventional ventilation in respiratory distress syndrome. Pediatrics 1992;89:5-12.
Courtney 2002 {published data only}
* Courtney SE, Durand DJ, Asselin JM, Hudak ML, Aschner JL, Shoemaker CT. High-frequency oscillatory ventilation versus conventional mechanical ventilation for very-low-birth-weight Infants. New England Journal of Medicine 2002;347:643-652.
Durand DJ, Asselin JM, Hudak ML, Aschner JL, McArtor RD, Cleary JP, VanMeurs KP, Stewart DL, Shoemaker CT, Wiswell TE, Courtney SE. Early high frequency oscillatory ventilation versus synchronized intermittent mandatory ventilation in very low birth weight infants: a pilot study of two ventilation protocols. Journal of Perinatology 2001;21:221-229.
Craft 2003 {published data only}
Craft SP, Bhandari V, Finer NN. The sy-fi study: a randomized prospective trial of synchronized intermittent mandatory ventilation versus a high-frequency flow interrupter in infants less than 1000 g. Journal of Perinatology 2003;23:14-19.
Durand 2001 {published data only}
Durand DJ, Asselin JM, Hudak ML, Aschner JL, McArtor RD, Cleary JP et al. Early high-frequency oscillatory ventilation versus synchronized mandatory ventilation in very low birth weight infants: a pilot study of two ventilation protocols. Journal of Perinatology 2001;21:221-229.
Gerstmann 1996 {published and unpublished data}
Gerstmann DR, Minton SD, Stoddard RA, Meredith KS, Bertrand JM. Results of the Provo multicenter surfactant high frequency oscillatory ventilation controlled trial. Pediatric Research 1995;37:333A.
* Gerstmann DR, Minton SD, Stoddard RA, Meredith KS, Monarco F, Bertrand JM, Battisti O, Langhendries JP, Francois A, Clark RH. The Provo multicenter early high-frequency oscillatory ventilation trial: Improved pulmonary and clinical outcome in respiratory distress syndrome. Pediatrics 1996;98:1044-1057.
Gerstmann DR, Minton SD, Stoddard RA, Meredith KS. The use of early high-frequency oscillatory ventilation in respiratory distress syndrome. Clinical Research 1994;42:109A.
Gerstmann DR, Minton SD, Stoddard RA. Results of the provo multicenter surfactant high frequency oxcillatory ventilation controlled trial. Pediatric Research 1995;37:333A.
Gerstmann DR, Wood K, Miller A, Steffen M, Ogden B, Stoddard RA, Minton SD. Childhood outcome after early high-frequency oscillatory ventilation for neonatal respiratory distress syndrome. Pediatrics 2001;108:617-623.
HIFI 1989 {published data only}
Abbasi S, Bhutani VK, Spitzer AR, Fox WW. Pulmonary mechanics in preterm neonates with respiratory failure treated with high-frequency compared with conventional mechanical ventilation. Pediatrics 1991;87:487-493.
Gerhardt T, Reifenberg L, Goldberg RN, Bancalari E. Pulmonary function in preterm infants whose lungs were ventilated conventionally or by high-frequency oscillation. Journal of Pediatrics 1989;115:121-126.
* The HIFI study group. High frequency oscillatory ventilation compared with conventional mechanical ventilation in the treatment of respiratory failure in preterm infants. New England Journal of Medicine 1989;320:88-93.
The HIFI study group. High frequency oscillatory ventilation compared with conventional mechanical ventilation in the treatment of respiratory failure in preterm infants: assessment of pulmonary function at 9 months of corrected age. Journal of Pediatrics 1990a;116:933-41.
The HIFI study group. High frequency oscillatory ventilation compared with conventional mechanical ventilation in the treatment of respiratory failure in preterm infants: neurodevelopmental status at 16 to 24 months of postterm age. Journal of Pediatrics 1990b;117:939-46.
Johnson 2002 {published data only}
Johnson AH, Peacock JL, Greenough A, Marlow N, Limb ES, Marston L, Calvert SA. High-frequency oscillatory ventilation for the prevention of chronic lung disease of prematurity. New England Journal of Medicine 2002;347:633-42.
Osborn DA, Evans N. Randomized trial of high-frequency oscillatory ventilation versus conventional ventilation: effects on systemic blood flow in very preterm infants. Journal of Pediatrics 2003;143:192-8.
Thomas MR, Rafferty GF, Limb ES, Peacock JL, Clavert SA, Marlow N, Milner AD, Greenough A. Pulmonary function at follow-up of very preterm infants from the United Kingdom oscillation study. American Journal of Respiratory and Critical Care Medicine 2004;169:868-72.
Moriette 2001 {published data only}
Moriette G, Walti H, Salanave B, Chagnot D, Magny J-F, Cambonie G, Pauchard JY, Cantagrel S, Lacaze T, Storme L, Blanc T, Liet J-M, Lebouedec S, Paris-Llado J, Breart G. Prospective randomized multicenter comparison of high-frequency oscillatory ventilation (HFOV) and conventional ventilation (CV) in preterm infants < 30 weeks gestational age (GA) with RDS. Pediatric Research 1999;45:212A.
* Moriette G, Paris-Llado J, Walti H, Escande B, Magny J-F, Cambonie G, Thiriez G, Cantagrel S, Lacaze-Masmonteil T, Storme L, Blanc T, Liet J-M, Andre C, Salanave B, Breart G. Prospective randomized multicenter comparison of high-frequency oscillatory ventilation and conventional ventilation in preterm infants of less than 30 weeks with respiratory distress syndrome. Pediatrics 2001;107:363-372.
Ogawa 1993 {published data only}
* Ogawa Y, Miyasaka K, Kawano T, Imura S, Inukai K, Okuyama K, Oguchi K, Togari H, Nishida H, Mishina J. A multicentre randomised trial of high frequency oscillatory ventilation as compared with conventional mechanical ventilation in preterm infants with respiratory failure. Early Human Development 1993;32:1-10.
Plavka 1999 {published data only}
Plavka R, Kopecky P, Sebron V, Svihovec P, Zlatohlavkova B, Janus V. A prospective randomized comparison of conventional mechanical ventilation and early high frequency oscillatory ventilation in extremely premature newborns with repiratory distress syndrome. Intensive Care Medicine 1999;25:68-75.
Rettwitz-Volk 1998 {published and unpublished data}
Rettwitz-Volk W, Veldman A, Roth B, Vierzig A, Kachel W, Varnholt V, Schlosser R, von Loewenich V. A prospective, randomized, multicentre trial of high-frequency oscillatory ventilation compared with conventional ventilation in preterm infants with respiratory distress syndrome receiving surfactant treatment. Journal of Pediatrics 1998;132:249-254.
Schreiber 2003 {published and unpublished data}
Mestan KK, Marks JD, Hecox K, Huo D, Schreiber MD. Neurodevelopmental outcomes of premature infants treated with inhaled nitric oxide. New England Journal of Medicine 2005;353:23-32.
* Schreiber MD, Gin-Mestan K, Marks JD, Hou D, Lee L, Srisuparp P. Inhaled nitric oxide in premature infants with respiratory distress. New England Journal of Medicine 2003;349:2099-107.
Schreiber MD, Gin-Mestan K, Srisuparp P, Marks J. Inhaled nitric oxide decreases BPD, death and IVH/PVL in premature infants with respiratory distress syndrome. Pediatric Research 2003;53:31.
Thome 1998 {published and unpublished data}
Thome U, Kossel H, Lipowsky G, Porz F, Furste H, Genzel-Boroviczeny O, Troger J, Oppermann H-C, Hogel J, Pohlandt F und das Team der HFOV-Studie. Hochfrequenzoszillationsbeatmung (HFOV) im Vergleich mit hochfrequenter intermittierender positiver Druckbeatmung (IPPV) als Ersttherapie bei Fruhgeborenen (FG) mit Atemnotsyndrom. Eine propektive randomisierte multizentrische Studie. In: Proc. German-Austrian Society for Neonatology and Pediatric Critical Care, Munster. October 1997.
Thome U, Kossel H, Lipowsky G, Porz F, Furste H, Genzel-Boroviczeny O, Troger J, Oppermann H-C, Hogel J, Pohlandt F and the HFOV Study Group. High frequency oscillatory ventilation (HFOV) compared with high rate intermittent positive pressure ventilation (IPPV) as first line therapy for premature infants with respiratory insufficiency. A prospective randomized multicenter trial. Pediatric Research 1998;43:300A.
* Thome U, Kossel H, Lipowsky G, Porz F, Furste HO, Genzel-Boroviczeny O, Troger J, Oppermann HC, Hogel J, Pohlandt F. Randomized comparison of high-frequency ventilation with high-rate intermittent positive pressure ventilation in preterm infants with respiratory failure. Journal of Pediatrics 1999;135:39-46.
Van Reempts 2003 {published data only}
* Van Reempts P, Borstlap C, Laroche S, Van der Auwer J-C. Early use of high frequency ventilation in the premature neonate. Eurpean Journal of Pediatrics 2003;162:219-226.
Van Reempts P, Borstlap K, Laroche S. Randomised controlled trial comparing high frequency ventilation versus conventional ventilation in preterm infants. Pediatric Research 2000;47:379A.
Vento 2005 {published data only}
* Vento G, Matassa PG, Ameglio F, Capoluongo E, Zecca E, Tortorolo L, Martelli M, Romagnoli C. HFOV in premature neonates: effects on pulmonary mechanics and epithelial lining fluid cytokines. A randomized controlled trial. Intensive Care Medicine 2005;31:463 - 70.
Vento G, Matassa PG, Ameglio F, Capoluongo E, Zecca E, Martelli M, Tortorolo L, Romagnoli C. HFOV improves lung mechanics and late pulmonary outcome in extremely low gestational age infants (<30 wks) with resoiratory distress syndrome. Pediatric Research 2002;51:393A.
References to excluded studies
Cambonie 2003 {published data only}Cambonie G. Guillaumont S. Luc F. Vergnes C. Milesi C. Voisin M. Haemodynamic features during high-frequency oscillatory ventilation in preterms. Acta Paediatrica 2003;92:1068-1073.
Froese 1987 {published data only}
Froese AB, Butler PO, Fletcher WA, Byford LJ. High-frequency oscillatory ventilation in premature infants with respiratory failure: a preliminary report. Anesthesia and Analgesia 1987;66:814-24.
HiFO 1993 {published data only}
HiFO study group. Randomised study of high-frequency oscillatory ventilation in infants with severe respiratory distress syndrome. Journal of Pediatrics 1993;122:609-19.
Lombert 1996 {published data only}
Lombert J, Claris O, Debauche C, Putet G, Rigo J, Verellen G, Salle B. High frequency oscillation (HFO) versus conventional mechanical ventilation (CMV) for respiratory distress syndrome (RDS). Proceedings of the European Society for Pediatric Research 1996:Abstract 110.
Pardou 1993 {published data only}
Pardou A, Vermeylen D, Muller MF, Detemmerman D. High-frequency ventilation and conventional mechanical ventilation in newborn babies with respiratory distress syndrome: a prospective, randomized trial. Critical Care Medicine 1993;19:406-10.
Ramanathan 1995 {published data only}
Ramanathan R, Ruiz I, Tantivit P, Cayabyab R, deLemos R. High frequency oscillatory ventilation compared to conventional mechanical ventilation in preterm infants with respiratory distress syndrome. Pediatric Research 1995;37:347A.
References to studies awaiting assessment
Dani 2006 {published data only}Dani C, Bertini G, Pezzati M, Filippi L, Pratesi S, Caviglioli C, Rubaltelli F. Effects of pressure support ventilation plus volume guarantee vs. high-frequency ventilation on lung inflammation in preterm infants. Pediatric Pulmonology 2006;41:242-249.
References to ongoing studies
Texas Infant Star {unpublished data only}Eligible infants include < 1250 gms birth weight or < 29 weeks gestation. Randomization to 3 modes of ventilation: conventional, high frequency oscillation, and combination (HFOV + 2 - 5 bpm CV). Study commenced in late 1996. Contact: Dr Anthony L Talbert, Texas Tech University School of Medicine, Odessa, Texas, USA Phone +1 915 335 5270.
* indicates the primary reference for the study
Other references
Additional references
Bancalari 1992Bancalari E, Sinclair JC. Mechanical ventilation. In: Sinclair JC, Bracken MB, editor(s). Effective Care of the Newborn Infant. Oxford: Oxford University Press, 1992:200-220.
Bhuta 2003
Bhuta T, Henderson-Smart DJ. Elective high frequency jet ventilation versus conventional ventilation in preterm infants mechanically ventilated for RDS (Cochrane Review). In: Cochrane Database of Systematic Reviews, Issue 1, 2003. John Wiley & Sons, Ltd.
Bhuta 2005
Bhuta T, Henderson-Smart DJ. Rescue high frequency oscillatory ventilation vs conventional ventilation in preterm infants with acute pulmonary dysfunction (Cochrane Review). In: Cochrane Database of Systematic Reviews, Issue 1, 2005. John Wiley & Sons, Ltd.
Bollen 2003
Bollen CW, Uiterwaal CS, van Vught AJ. Cumulative meta-analysis of high-frequency versus conventional ventilation in premature neonates. American Journal of Respiratory Critical Care Medicine 2003;168:1150-5.
Clark 2000
Clark RH, Slutsky AS, Gerstmann DR. Lung protective strategies of ventilation in the neonate: what are they? Pediatrics 2000;105:112-4.
de Lemos 1987
de Lemos RA, Coalson JS, Gerstmann DR et al. Ventilatory management of infant baboons with hyaline membrane disease; the use of high frequency ventilation. Pediatric Research 1987;21:594-602.
Ehrenkrantz 1992
Ehrenkranz RA, Mercurio MR. Bronchopulmonary dysplasia. In: Sinclair JC, Bracken MB, editor(s). Effective Care of theNewborn Infant. Oxford: Oxford University Press, 1992:399-424.
Froese 1991
Froese AB, Bryan AC. Reflections on the HIFI trial. Pediatrics 1991;87:565-567.
Greenough 2003
Greenough A, Milner AD, Dimitriou G. Synchronised mechanical ventilation in neonates (Cochrane Review). In: Cochrane Database of Systematic Reviews, Issue 3, 2004. John Wiley & Sons, Ltd.
Halliday 2003
Halliday H, Ehrenkranz R. Moderately early (7-14 days) postnatal corticosteroids for preventing chronic lung disease in preterm infants (Cochrane Review). In: Cochrane Database of Systematic Reviews, Issue 1, 2003. John wiley & Sons, Ltd.
Jobe 2000
Jobe AH, Ikegami M. Lung development and function in preterm infants in the surfactant treatment era. Annual Review Physiology 2000;62:825-46.
Jouvet 1997
Jouvet P, Hubert P, Isabey D, Oinquier D, Dahan E, Cloup M, Harf A. Assessment of high-frequency neonatal ventilator performances. Intensive Care Medicine 1997;23:208-213.
Kinsella 1991
Kinsella JP, Gerstmann DR, Clark RH, Null DM Jr, Morrow WR, Taylor AF, deLemos RA. High frequency oscillatory ventilation versus intermittent mandatory ventilation: early hemodynamic effects in the premature baboon with hyaline membrane disease. Pediatric Research 1991;29:160-166.
Laubscher 1996
Laubscher B, van Melle G, Fawer C-L, Sekarski N, Calame A. Haemodynamic changes during high frequency oscillation for respiratory distress syndrome. Archives of Diseases in Childhood 1996;74:F172-F176.
McCulloch 1988
McCulloch PR, Forkert PG, Froese AB. Lung volume maintenance prevents lung injury during high-frequency oscillatory ventilation in surfactant-deficient rabbits. American Review of Respiratory Disease 1988;137:1185-92.
Meredith 1989
Meredith KS, deLemos RA, Coalson JJ, King RJ, Gerstmann DR, Kumar R, et al. Role of lung injury in the pathogenesis of hyaline membrane disease in premature baboons. Journal of Applied Pysiology 1989;66:2150-8.
Northway 1992
Northway WH. An introduction to bronchopulmonary dysplasia. Clinics in Perinatology 1992;19:489-495.
Petrucci 2006
Petrucci N, Iacovelli W. Ventilation with lower tidal volumes versus traditional tidal volumes in adults for acute lung injury and acute respiratory distress syndrome. In: Cochrane Database of Systematic Reviews, Issue 3, 2006. Chichester, UK: John Wiley & Sons Ltd.
Pillow 1999
Pillow, Neil et al.. Effect of I/E ratio on mean alveolar pressure during high-frequency oscillatory ventilation. Journal of Applied Physiology 1999;87:407-414.
Roberts 2006
Roberts D, Dalziel S. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. In: Cochrane Database of Systematic Reviews, Issue 3, 2006. John Wiley & Sons, Ltd.
Thome 2005
Thome UH, Carlo WA, Pohlandt F. Ventilation strategies and outcome in randomized trials of high frequency ventilation. Archives of Disease in Childhood Fetal and Neonatal Edition 2005;90:F466-73.
Truog 1984
Truog WE, Standaert TA, Murphy JH, Woodrum DE, Hodson WA. Effect of prolonged high frequency oscillatory ventilation in premature primates with experimental hyaline membrane disease. American Review of Respiratory Disease 1984;130:76-80.
Woodgate 2006
Woodgate PG, Davies WW. Permissive hypercapnia for the prevention of morbidity and mortality in mechanically ventilated newborn infants. In: Cochrane Database of Systematic Reviews, Issue 3, 2006. John wiley & Sons Ltd.
Other published versions of this review
Henderson-Smart 1999Henderson-Smart DJ, Bhuta T, Cools F, Offringa M. Elective high frequency oscillatory ventilation vs conventional ventilation for acute pulmonary dysfunction in preterm infants (Cochrane Review). In: Cochrane Database of Systematic Reviews, Issue 2, 1999. Oxford: Update Software.
Henderson-Smart 2001
Henderson-Smart DJ, Bhuta T, Cools F, Offringa M. Elective high frequency oscillatory ventilation versus conventional ventilation for acute pulmonary dysfunction in preterm infants (Cochrane Review). In: Cochrane Database of Systematic Reviews, Issue 4, 2001. Oxford: Update Software.
Henderson-Smart 2003
Henderson-Smart DJ, Bhuta T, Cools F, Offringa M. Elective high frequency oscillatory ventilation versus conventional ventilation for acute pulmonary dysfunction in preterm infants (Cochrane Review). In: Cochrane Database of Systematic Reviews, Issue 4, 2003. Oxford: Update Software.
Comparisons and data
| Comparison or outcome |
Studies |
Participants |
Statistical method |
Effect size |
| 01 HFOV vs CV (all trials) |
| 01 Death by 28-30 days |
9 |
2060 |
RR (fixed), 95% CI |
1.09 [0.88, 1.35] |
| 02 Mechanical ventilation at 28 - 30 days in survivors |
3 |
767 |
RR (fixed), 95% CI |
1.08 [0.86, 1.35] |
| 03 Oxygen at 28-30 days in survivors |
6 |
1043 |
RR (fixed), 95% CI |
0.98 [0.88, 1.10] |
| 04 CLD at 28-30 days (O2 + xray) in survivors |
4 |
820 |
RR (fixed), 95% CI |
0.86 [0.74, 1.01] |
| 05 Death or CLD at 28-30 days |
5 |
1160 |
RR (fixed), 95% CI |
0.94 [0.85, 1.04] |
| 06 Death by 36-37 weeks or discharge |
13 |
2820 |
RR (fixed), 95% CI |
0.98 [0.83, 1.14] |
| 07 CLD at 36-37 weeks PMA or discharge in survivors |
13 |
2310 |
RR (fixed), 95% CI |
0.89 [0.81, 0.99] |
| 08 Death or CLD at 36-37 weeks PMA or discharge |
13 |
2820 |
RR (fixed), 95% CI |
0.93 [0.86, 1.00] |
| 09 Any pulmonary air leak |
11 |
2726 |
RR (fixed), 95% CI |
1.19 [1.05, 1.34] |
| 10 Gross pulmonary air leak |
9 |
1804 |
RR (fixed), 95% CI |
1.32 [1.00, 1.72] |
| 11 Intraventricular hemorrhage - all grades |
10 |
2971 |
RR (fixed), 95% CI |
1.05 [0.96, 1.15] |
| 12 Intraventricular hemorrhage - grd 3 or 4 |
15 |
3585 |
RR (fixed), 95% CI |
1.11 [0.95, 1.30] |
| 13 Periventricular leukomalacia |
13 |
3474 |
RR (fixed), 95% CI |
1.10 [0.85, 1.43] |
| 14 Retinopathy of prematurity (grd 2 or more) in survivors |
10 |
2367 |
RR (fixed), 95% CI |
0.85 [0.74, 0.99] |
| 02 HFOV vs CV subgrouped by volume strategy
on HFOV |
| 01 Death by 36-37 weeks or discharge |
13 |
2820 |
RR (fixed), 95% CI |
0.98 [0.83, 1.14] |
| 02 CLD at 36-37 weeks PMA or discharge in survivors |
13 |
2310 |
RR (fixed), 95% CI |
0.89 [0.81, 0.99] |
| 03 Death or CLD at 36-37 weeks PMA or discharge |
13 |
2820 |
RR (fixed), 95% CI |
0.93 [0.86, 1.00] |
| 04 Gross pulmonary air leak |
9 |
1804 |
RR (fixed), 95% CI |
1.32 [1.00, 1.72] |
| 05 Intraventricular hemorrhage - grd 3 or 4 |
15 |
3585 |
RR (fixed), 95% CI |
1.11 [0.95, 1.30] |
| 06 Periventricular leukomalacia |
13 |
3474 |
RR (fixed), 95% CI |
1.10 [0.85, 1.43] |
| 03 HFOV vs CV subgouped by use of surfactant |
| 01 Death by 36-37 weeks or discharge |
13 |
2820 |
RR (fixed), 95% CI |
0.98 [0.83, 1.14] |
| 02 CLD at 36-37 weeks PMA or discharge in survivors |
13 |
2310 |
RR (fixed), 95% CI |
0.89 [0.81, 0.99] |
| 03 Death or CLD at 36-37 weeks PMA or discharge |
13 |
2820 |
RR (fixed), 95% CI |
0.93 [0.86, 1.00] |
| 04 Gross pulmonary air leak |
9 |
1804 |
RR (fixed), 95% CI |
1.32 [1.00, 1.72] |
| 05 Intraventricular hemorrhage - grd 3 or 4 |
15 |
3585 |
RR (fixed), 95% CI |
1.11 [0.95, 1.30] |
| 06 Periventricular leukomalacia |
13 |
3474 |
RR (fixed), 95% CI |
1.10 [0.85, 1.43] |
| 04 HFOV vs CV subgrouped by type of HFO ventilator |
| 01 Death by 36-37 weeks or discharge |
13 |
2820 |
RR (fixed), 95% CI |
0.98 [0.83, 1.14] |
| 02 CLD at 36-37 weeks PMA or discharge in survivors |
13 |
2310 |
RR (fixed), 95% CI |
0.89 [0.81, 0.99] |
| 03 Death or CLD at 36-37 weeks PMA or discharge |
13 |
2820 |
RR (fixed), 95% CI |
0.93 [0.86, 1.00] |
| 04 Gross pulmonary air leak |
9 |
1804 |
RR (fixed), 95% CI |
1.32 [1.00, 1.72] |
| 05 Intraventricular hemorrhage - grd 3 or 4 |
15 |
3585 |
RR (fixed), 95% CI |
1.11 [0.95, 1.30] |
| 06 Periventricular leukomalacia |
14 |
3476 |
RR (fixed), 95% CI |
1.10 [0.85, 1.43] |
| 05 HFOV vs CV subgrouped by lung protective
(LPS) CV strategy |
| 01 Death by 36-37 weeks or discharge |
13 |
2820 |
RR (fixed), 95% CI |
0.98 [0.83, 1.14] |
| 02 CLD at 36-37 weeks PMA or discharge in survivors |
13 |
2310 |
RR (fixed), 95% CI |
0.89 [0.81, 0.99] |
| 03 Death or CLD at 36-37 weeks PMA or discharge |
13 |
2822 |
RR (fixed), 95% CI |
0.93 [0.86, 1.00] |
| 04 Gross pulmonary air leak |
9 |
1804 |
RR (fixed), 95% CI |
1.32 [1.00, 1.72] |
| 05 Intraventricular hemorrhage - grd 3 or 4 |
15 |
3585 |
RR (fixed), 95% CI |
1.11 [0.95, 1.30] |
| 06 Periventricular leukomalacia |
13 |
3474 |
RR (fixed), 99% CI |
1.10 [0.78, 1.55] |
| 06 HFOV vs CV subgrouped by age at randomisation |
| 01 Death by 36-37 weeks or discharge |
11 |
2474 |
RR (fixed), 95% CI |
0.95 [0.80, 1.12] |
| 02 CLD at 36-37 weeks PMA or discharge in survivors |
11 |
2015 |
RR (fixed), 95% CI |
0.86 [0.78, 0.96] |
| 03 Death or CLD at 36-37 weeks PMA or discharge |
11 |
2474 |
RR (fixed), 95% CI |
0.90 [0.83, 0.97] |
| 04 Gross pulmonary air leak |
8 |
1504 |
RR (fixed), 95% CI |
1.29 [0.97, 1.70] |
| 05 Intraventricular hemorrhage - grd 3 or 4 |
13 |
3239 |
RR (fixed), 95% CI |
1.11 [0.95, 1.31] |
| 06 Periventricular leukomalacia |
13 |
3176 |
RR (fixed), 95% CI |
1.08 [0.82, 1.41] |
| 07 HFOV vs CV subgrouped by I:E ratio on HFOV |
| 01 Death by 36-37 weeks or discharge |
13 |
2820 |
RR (fixed), 95% CI |
0.98 [0.83, 1.14] |
| 02 CLD at 36-37 weeks PMA or discharge in survivors |
13 |
2310 |
RR (fixed), 99% CI |
0.89 [0.78, 1.02] |
| 03 Death or CLD at 36-37 weeks PMA or discharge |
13 |
2820 |
RR (fixed), 95% CI |
0.93 [0.86, 1.00] |
| 04 Gross pulmonary air leak |
9 |
1804 |
RR (fixed), 95% CI |
1.32 [1.00, 1.72] |
| 05 Intraventricular hemorrhage - grd 3 or 4 |
14 |
3544 |
RR (fixed), 95% CI |
1.11 [0.95, 1.30] |
| 06 Periventricular leukomalacia |
13 |
3474 |
RR (fixed), 95% CI |
1.10 [0.85, 1.43] |
01 HFOV vs CV (all trials)
01.01 Death by 28-30 days
01.02 Mechanical ventilation at 28 - 30 days in
survivors
01.03 Oxygen at 28-30 days in survivors
01.04 CLD at 28-30 days (O2 + xray) in survivors
01.05 Death or CLD at 28-30 days
01.06 Death by 36-37 weeks or discharge
01.07 CLD at 36-37 weeks PMA or discharge in survivors
01.08 Death or CLD at 36-37 weeks PMA or discharge
01.09 Any pulmonary air leak
01.10 Gross pulmonary air leak
01.11 Intraventricular hemorrhage - all grades
01.12 Intraventricular hemorrhage - grd 3 or 4
01.13 Periventricular leukomalacia
01.14 Retinopathy of prematurity (grd 2 or more)
in survivors
02 HFOV vs CV subgrouped by volume strategy on HFOV
02.01 Death by 36-37 weeks or discharge
02.01.01 High volume strategy
02.01.02 No high volume strategy
02.02 CLD at 36-37 weeks PMA or discharge in survivors
02.02.01 High volume strategy
02.02.02 No high volume strategy of HFOV
02.03 Death or CLD at 36-37 weeks PMA or discharge
02.03.01 High volume strategy on HFOV
02.03.02 No high volume strategy on HFOV
02.04 Gross pulmonary air leak
02.04.01 High volume strategy HFOV
02.04.02 No high volume strategy on HFOV
02.05 Intraventricular hemorrhage - grd 3 or 4
02.05.01 High volume strategy on HFOV
02.05.02 No high volume strategy on HFOV
02.06 Periventricular leukomalacia
02.06.01 High volume strategy on HFOV
02.06.02 No high volume strategy on HFOV
03 HFOV vs CV subgouped by use of surfactant
03.01 Death by 36-37 weeks or discharge
03.01.01 Routine surfactant
03.01.02 No routine surfactant
03.02 CLD at 36-37 weeks PMA or discharge in survivors
03.02.01 Routine surfactant
03.02.02 No routine surfactant
03.03 Death or CLD at 36-37 weeks PMA or discharge
03.03.01 Routine surfactant
03.03.02 No routine surfactant
03.04 Gross pulmonary air leak
03.04.01 Routine surfactant
03.04.02 No routine surfactant
03.05 Intraventricular hemorrhage - grd 3 or 4
03.05.01 Routine surfactant
03.05.02 No routine surfactant
03.06 Periventricular leukomalacia
03.06.01 Rouitine surfactant
03.06.02 No routine surfactant
04 HFOV vs CV subgrouped by type of HFO ventilator
04.01 Death by 36-37 weeks or discharge
04.01.01 Flow interrupter
04.01.02 HF oscillator
04.01.03 Both HF oscillation and flow interruptors
04.02 CLD at 36-37 weeks PMA or discharge in survivors
04.02.01 Flow interrupter
04.02.02 HF oscillator
04.02.03 Both HF oscillators and flow interrupters
04.03 Death or CLD at 36-37 weeks PMA or discharge
04.03.01 HF flow interrupter
04.03.02 HF oscillation
04.03.03 Both HF oscillators and HF flow interrupters
04.04 Gross pulmonary air leak
04.04.01 HF flow interrupter
04.04.02 HF oscillation
04.04.03 Both HF oscillators and HF flow interrupters
04.05 Intraventricular hemorrhage - grd 3 or 4
04.05.01 HF flow interrupter
04.05.02 HF oscillator
04.05.03 Both HF oscillators and HF flow interrupters
04.06 Periventricular leukomalacia
04.06.01 HF flow interrupter
04.06.02 HF oscillator
04.06.03 Both HF oscillators and HF flow interrupters
05 HFOV vs CV subgrouped by lung protective (LPS) CV strategy
05.01 Death by 36-37 weeks or discharge
05.01.01 Definitive LPS on CV
05.01.02 Probable LPS on CV
05.01.03 Probably no LPS on CV
05.01.04 Definitively no LPS on CV
05.02 CLD at 36-37 weeks PMA or discharge in survivors
05.02.01 Definitive LPS on CV
05.02.02 Probable LPS on CV
05.02.03 Probably no LPS on CV
05.02.04 Definitively no LPS on CV
05.03 Death or CLD at 36-37 weeks PMA or discharge
05.03.01 Definitive LPS on CV
05.03.02 Probable LPS on CV
05.03.03 Probably no LPS on CV
05.03.04 Definitively no LPS on CV
05.04 Gross pulmonary air leak
05.04.01 Definitive LPS on CV
05.04.02 Probable LPS on CV
05.04.03 Probably no LPS on CV
05.04.04 Definitively no LPS on CV
05.05 Intraventricular hemorrhage - grd 3 or 4
05.05.01 Definitive LPS on CV
05.05.02 Probable LPS on CV
05.05.03 Probably no LPS on CV
05.05.04 Definitively no PLS on CV
05.06 Periventricular leukomalacia
05.06.01 Definitive LPS on cv
05.06.02 Probable LPS on CV
05.06.03 Probably no LPS on CV
05.06.04 Definitively no LPS on CV
06 HFOV vs CV subgrouped by age at randomisation
06.01 Death by 36-37 weeks or discharge
06.01.01 Less than 2 hours
06.01.02 2 to 6 hours
06.01.03 Greater than 6 hours
06.02 CLD at 36-37 weeks PMA or discharge in survivors
06.02.01 Less than 2 hours
06.02.02 2 to 6 hours
06.02.03 Greater than 6 hours
06.03 Death or CLD at 36-37 weeks PMA or discharge
06.03.01 Less than 2 hours
06.03.02 2-6 hours
06.03.03 Greater than 6 hours
06.04 Gross pulmonary air leak
06.04.01 Less than 2 hours
06.04.02 2 - 6 hours
06.04.03 Greater than 6 hours
06.05 Intraventricular hemorrhage - grd 3 or 4
06.05.01 less than 2 hours
06.05.02 2 - 6 hours
06.05.03 Greater than 6 hours
06.06 Periventricular leukomalacia
06.06.01 Less than 2 hours
06.06.02 2 - 6 hours
06.06.03 Greater than 6 hours
07 HFOV vs CV subgrouped by I:E ratio on HFOV
07.01 Death by 36-37 weeks or discharge
07.01.01 1:1
07.01.02 1:2
07.01.03 Range of I:Es or unknown
07.02 CLD at 36-37 weeks PMA or discharge in survivors
07.02.01 1:1
07.02.02 1:2
07.02.03 Range of I:Es or unknown
07.03 Death or CLD at 36-37 weeks PMA or discharge
07.03.01 1:1
07.03.02 1:2
07.03.03 Range of I:Es or unknown
07.04 Gross pulmonary air leak
07.04.01 1:1
07.04.02 1:2
07.04.03 Range of I:Es or unknown
07.05 Intraventricular hemorrhage - grd 3 or 4
07.05.01 1:1
07.05.02 1:2
07.05.03 Range of I:Es or unknown
07.06 Periventricular leukomalacia
07.06.01 1:1
07.06.02 1:2
07.06.03 Range of I:Es or unknown
Contact details for co-reviewers
Dr Tushar Bhuta, MBBS FRACP MD DCh MMed(Clin Epi)
Staff Specialist
Department of Neonatal Medicine
Royal North Shore Hospital
Pacific Highway
St Leonards
Sydney
New South Wales AUSTRALIA
2065
Telephone 1: +61 2 9926 5586
Telephone 2: 0412 980 130
Facsimile: +61 2 9926 6651
E-mail: tbhuta@med.usyd.edu.au
Secondary address (home):
45 Station Street
Pymble
Sydney
New South Wales AUSTRALIA
2073
Telephone: +61 2 9449 5010
Facsimile: +61 2 9402 5876Dr Filip Cools
Neonatologist
Pediatrics
Academic Hospital, Free University of Brussels
Laarbeekaan 101
Brussels
BELGIUM
1090
Telephone 1: +32 2 4776065
Facsimile: +32 2 4776095
E-mail: Filip.Cools@az.vub.ac.be
DR Martin Offringa
Neonatologist
Pediatrics, H3-144
Academic Medical Center
P.O. Box 22700
Amsterdam
NETHERLANDS
1100 DE
Telephone 1: +31 20 566 9111
E-mail: m.offringa@amc.uva.nl
| This review is published as a Cochrane review in The Cochrane Library,
Issue 3, 2007 (see http:www.thecochranelibrary.com for information).
Cochrane reviews are regularly updated as new evidence emerges and in response
to feedback. The Cochrane Library should be consulted for the most recent
version of the review. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
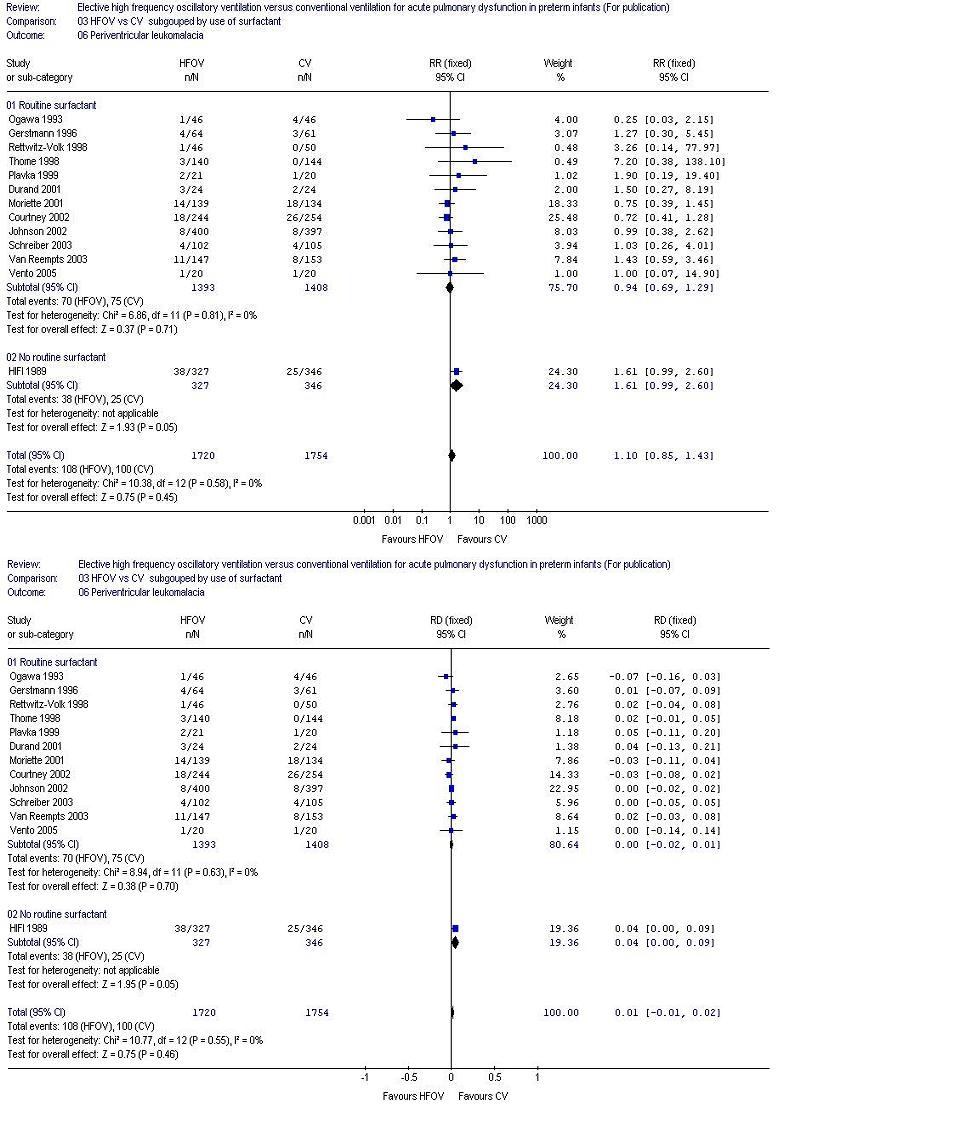{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
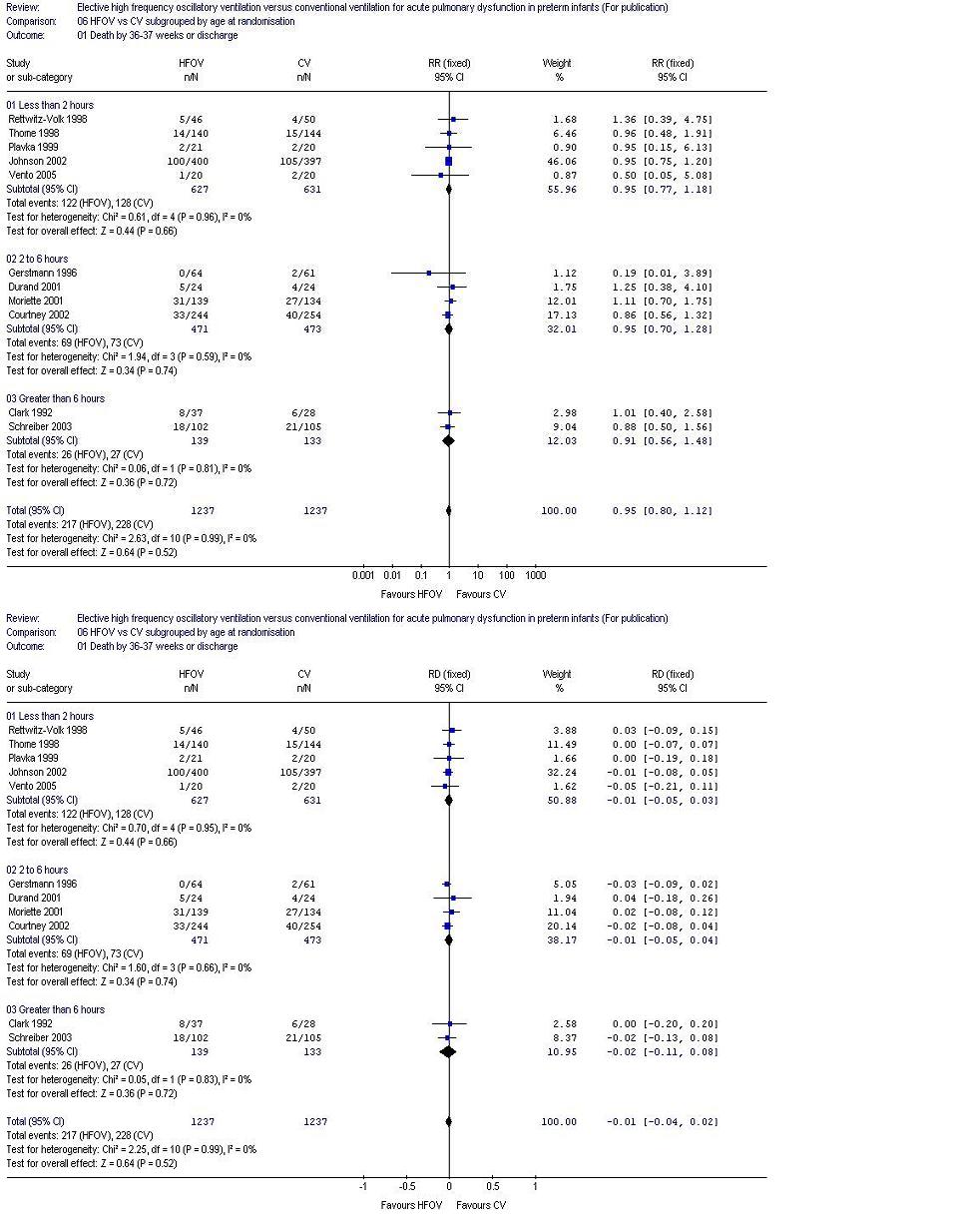{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}