|
| About Fogarty |
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
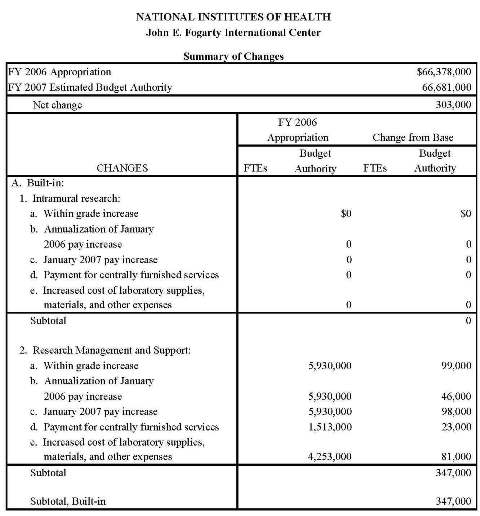
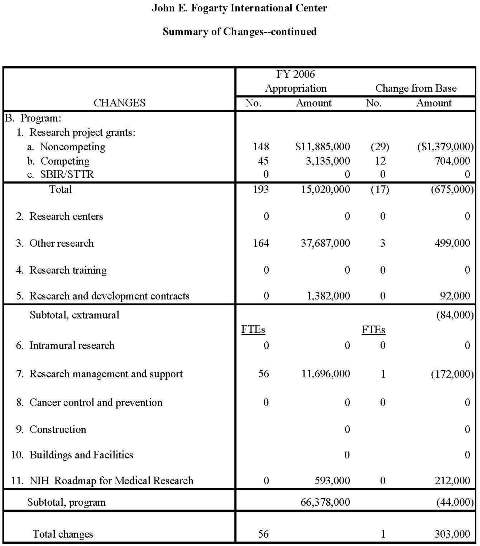
FIC FY2007 Congressional JustificationTable of Contents- Budget authority by activity - Significant items in House, Senate and Conference Appropriations Committee Reports - Detail of Full-time Equivalent Employment (FTE) 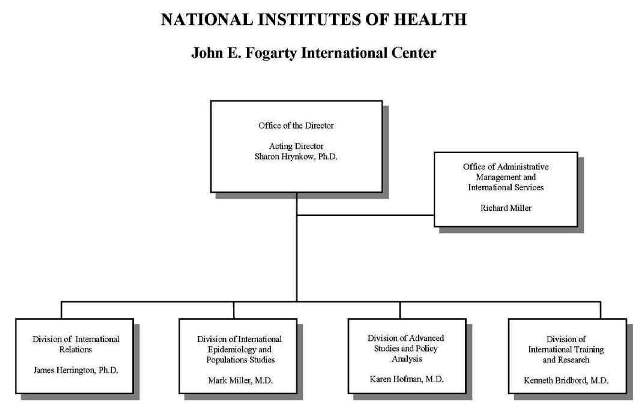 FY 2007 Proposed Appropriation Language:For carrying out the activities at the John E. Fogarty International Center [$67,048,000] $66,681,000. Amounts Available for Obligation *
* Excludes the following amounts for reimbursable activities carried out by this account: FY 2005 - $2,344,976; JustificationAuthorizing Legislation: Sections 301 and 307 and Title IV of the Public Health Service Act, as amended.
This document provides justification for the Fiscal Year (FY) 2007 activities of the John E. Fogarty International Center of $66,681,000, including HIV/AIDS activities. A more detailed description of NIH-wide Fiscal Year 2007 HIV/AIDS activities can be found in the NIH section entitled, "Office of AIDS Research (OAR)." Detailed information on the NIH Roadmap for Medical Research may be found in the Overview section. INTRODUCTION"Time and time again, it has been demonstrated that the goal of better health has the capacity to demolish geographic and political boundaries and to enter the hearts and minds of men, women, and children in the four corners of the earth. It is an issue which serves as a forceful reminder of the oneness, the essential brotherhood of man." Congressman John E. Fogarty, Congressional Record, 1959. When it comes to disease, we are truly one world. Congressman Fogarty, the visionary namesake of the National Institutes of Health (NIH) John E. Fogarty International Center for Advanced study in the Health Sciences, recognized this reality more than 40 years ago. His words and those of his Congressional colleagues implored us to work for "a healthy America, in a healthier world." Today, the Fogarty International Center works to meet this goal in two ways: by supporting the whole of the NIH mission via international partnerships, and through the development of global health research and training programs all aimed at improving the health of citizens in the United States and around the globe. In an increasingly interconnected global community, what befalls one country befalls all. The H5N1 bird flu is a stark reminder to the global community of the devastation and suffering that pandemic flu can cause. In 1918, pandemic influenza led to the deaths of an estimated 20-50 million worldwide, 0.5 - 1 million in the U.S. alone.[1] As we consider the potential of bird flu to wreak havoc on the human population, the importance of efforts to strengthen the ability of laboratory personnel in key countries to detect new strains and to respond as quickly as possible becomes clear. Building capacity in partner countries is also invaluable as we work to combat the scourge of HIV/AIDS and other infectious diseases. In addition, as chronic diseases including cardiovascular disease and cancer continue to rise in every nation on earth, our global scientific collaborations become even more critical to tackling these diseases. One of FIC's main functions is to build cadres of scientists in low- and middle-income countries who can collaborate in solving vital health problems. FIC capacity building programs provide epidemiological and laboratory training to scientists on the frontlines to detect infectious diseases and to develop drugs and treatments to prevent contagion, essential components of the global effort to mitigate the spread of influenza. These programs also develop local expertise in epidemiology that has contributed to significant lowering of AIDS incidence in key countries such as Haiti, Uganda, and Thailand, and that paves the way for successful prevention and treatment programs in mental health, cancer, and for conditions caused by environmental pollution, among others. In a world where one can move from any city on the globe to any other in 24 hours time, where communities in one part of the globe are strikingly similar genetically to communities thousands of miles away, the development of the international scientific framework is an endeavor that leads to protection of health of people everywhere. The second major function of the Fogarty International Center is to support the whole of the NIH mission through international partnerships. In doing so, we take into account the words of the famous French scientist, Louis Pasteur, who said, "Science knows no country because it is the light that illuminates the world." Fogarty's work to foster ties and to build bridges with NIH equivalent organizations and with international scientists has yielded significant benefit. Longstanding collaborations with the Japan Society for the Promotion of Science and the Human Frontier Science Programme have supported the development of young scientists across the globe. Newer programs such as the Civilian Research and Development Foundation have created partnerships between U.S. scientists and former weapons scientists from Russia and other former Soviet Union states. Nascent efforts to create a global network of agencies working to advance the health of indigenous peoples - expected to include the U.S., Australia, Canada, and New Zealand - through research and to support the International Polar Year which commences 2007 promise to leverage resources among national to make a difference in these neglected groups. These efforts to build a scientific community among nations are examples of FIC's initiatives in "health diplomacy." Indeed, they are "health diplomacy" in action. Back to topSCIENCE ADVANCES AND NEW INITIATIVESResearch and training programs to tackle global health challengesHIV/AIDS. Fogarty continues to place a high priority on combining HIV/AIDS - the deadliest pandemic of modern times. An estimated 4.9 million people worldwide became newly infected with HIV in 2004 - the highest number of new cases reported in any single year since the beginning of the pandemic.[2] Women and girls now make up almost 57% of all people infected with HIV in sub-Saharan Africa, where a striking 76% of young people (aged 15-24 years) living with HIV are female.[3] As the United States works to combat the AIDS problem domestically, one thing is clear - we will not solve our own crisis until the AIDs situation is solved globally. Trained scientists in countries hard-hit by AIDS are crucial allies in our fight. In its 18 year history, Fogarty's AIDS International Research and Training Program (AITRP) has helped to train nearly 2,000 health scientists, including Ph.D. and Masters level researchers from developing countries working on AIDS. More than 50,000 have received short-course training in their home countries through this program. These scientists represent a substantial increase in the global capacity to fight AIDS and a wealth of allies in our international struggle. Science Advance. A small number of studies have found higher rates of HIV transmission from mother to girl infants than boy infants, but these studies have not been able to determine whether the female babies were at increased risk of transmission during pregnancy, during labor and delivery, or during breastfeeding. Researchers at Johns Hopkins University and the University of Malawi examined the rates of HIV transmission among girl and boy infants at birth and at 6-8 weeks post delivery. Infants were enrolled in two studies that evaluated two different infant drug regimens to prevent HIV transmission. At birth, the infant girls were twice as likely as the boys to be HIV infected, indicating that the risk of infection during pregnancy was much higher for girls. At 6-8 weeks of age, among those infants not infected at birth, the increased risk for girls remained, though at a lower level, indicating that the risk of transmission through breastfeeding might also be higher for girls. Scientists are now considering whether infant girls are more susceptible to HIV infection or whether boy infants are more likely to die from the infection. These findings have implications for development of the most effective prevention strategies. Story of "Public Health Success"
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| MECHANISM: Research Grants | FY2005 Actual (No.) | FY2005 Actual (Amount) | FY2006 Appropriation (No.) | FY2006 Appropriation (Amount) | FY2007 Estimate (No.) | FY2007 Estimate (Amount) |
|---|---|---|---|---|---|---|
| Research Projects: | ||||||
| Non-competing | 154 |
$11.419,000 |
148 |
$11,464,000 |
119 |
$10,086,000 |
| Administrative supplements | (12) |
528,000 |
(9) |
421,000 |
(9) |
420,000 |
| Competing: | ||||||
| Renewal | 3 |
680,000 |
0 |
0 |
0 |
0 |
| New | 54 |
3,350,000 |
45 |
3,135,000
|
57 |
3,839,000 |
| Supplements | 0 |
0 |
0 |
0 |
0 |
0 |
| Subtotal, competing | 57 |
4,030,000 |
45 |
3,135,000 |
57 |
3,839,000 |
| Subtotal, RPGs | 211 |
15,977,000 |
193 |
15,020,000 |
176 |
14,345,000 |
| SBIR/STTR | 0 |
0 |
0 |
0 |
0 |
0 |
| Subtotal, RPGs | 211 |
15,977,000 |
193 |
15,020,000 |
176 |
14,345,000 |
| Research Centers: | ||||||
| Specialized/ comprehensive |
0 |
0 |
0 |
0 |
0 |
0 |
| Clinical research | 0 |
0 |
0 |
0 |
0 |
0 |
| Biotechnology | 0 |
0 |
0 |
0 |
0 |
0 |
| Comparative medicine | 0 |
0 |
0 |
0 |
0 |
0 |
| Research Ctrs. in Minority Institutions | 0 |
0 |
0 |
0 |
0 |
0 |
| Subtotal, Centers | 0 |
125 |
0 |
0 |
0 |
0 |
| Other Research: | ||||||
| Research careers | 16 |
1,717,000 |
15 |
1,643,000 |
17 |
1,823,000 |
| Cancer education | 0 |
0 |
0 |
0 |
0 |
0 |
| Cooperative clinical research | 0 |
0 |
0 |
0 |
0 |
0 |
| Biomedical research support | 0 |
0 |
0 |
0 |
0 |
0 |
| Minority biomedical research support | 0 |
0 |
0 |
0 |
0 |
0 |
| Other | 147 |
35,921,000 |
149 |
36,044,000 |
150 |
36,363,000 |
| Subtotal, Other Research | 163 |
37,638,000 |
164 |
37,687,000 |
167 |
38,186,000 |
| Total Research Grants | 374 |
53,615,000 |
357 |
52,707,000 |
343 |
52,531,000 |
| Research Training: | FTTPs |
FTTPs |
FTTPs |
|||
| Individual awards | 0 |
0 |
0 |
0 |
0 |
0 |
| Institutional awards | 0 |
0 |
0 |
0 |
0 |
0 |
| Total, Training | 0 |
0 |
0 |
0 |
0 |
0 |
| Research & development contracts | 0 |
0 |
0 |
0 |
0 |
0 |
| (SBIR/STTR) | (0) |
(0) |
(0) |
(0) |
(0) |
(0) |
FTEs |
FTEs |
FTEs |
||||
| Intramural research | 0 | 0 |
0 |
0 |
0 |
0 |
| Research management and support | 51 |
11,294,000 |
56 |
11,696,000 |
57 |
11,871,000 |
| Cancer prevention & control | 0 |
0 |
0 |
0 |
0 |
0 |
| Construction | 0 |
0 |
0 |
|||
| Buildings & Facilities | 0 |
0 |
0 |
|||
| NIH Roadmap for Medical Research | 0 |
421,000 |
0 |
593,000 |
0 |
805,000 |
| Total, N | 51 |
66,632,000 |
56 |
66,378,000 |
57 |
66,681,000 |
| (Clinical Trials) | (0) |
(0) |
(0) |
|
| FY 2006 Appropriation |
FY 2007 Estimate |
Increase or Decrease | |
|---|---|---|---|
| Total compensable work years: | |||
| Full-time employment | 56 |
57 |
1 |
| Full-time equivalent of overtime & holiday hours | 1 |
1 |
0 |
| Average ES salary | $154,263 |
$158,120 |
$3,857 |
| Average GM/GS grade | 11.6 |
11.6 |
0.0 |
| Average GM/GS salary | $81,482 |
$83,112 |
$1,630 |
| Average salary, grade established by act of July 1, 1944 (42 U.S.C. 207) | $88,644 |
$90,971 |
$2,327 |
| Average salary of ungraded positions | 138,653 |
142,292 |
3,639 |
OBJECT CLASSES |
FY 2006 Appropriation |
FY 2007 Estimate |
Increase or Decrease |
| Personnel Compensation: | |||
| 11.1 Full-Time Permanent | $3,569,000 |
$3,717,000 |
$148,000 |
| 11.3 Other than Full-Time Permanent | 668,000 |
695,000 |
27,000 |
| 11.5 Other Personnel Compensation | 80,000 |
83,000 |
3,000 |
| 11.7 Military Personnel | 226,000 |
235,000 |
9,000 |
| 11.8 Special Personnel Services Payments | 53,000 |
55,000 |
2,000 |
Total, Personnel Compensation |
4,596,000 |
4,785,000 |
189,000 |
| 12.0 Personnel Benefits | 1,129,000 |
1,173,000 |
44,000 |
| 12.2 Military Personnel Benefits | 205,000 |
215,000 |
10,000 |
| 13.0 Benefits for Former Personnel | 0 |
0 |
0 |
Subtotal, Pay Costs |
5,930,000 |
6,173,000 |
243,000 |
| 21.0 Travel & Transportation of Persons | 335,000 |
335,000 |
0 |
| 22.0 Transportation of Things | 21,000 |
21,000 |
0 |
| 23.1 Rental Payments to GSA | 0 |
0 |
0 |
| 23.2 Rental Payments to Others | 0 |
0 |
0 |
| 23.3 Communications, Utilities & Miscellaneous Charges | 70,000 |
72,000 |
2,000 |
| 24.0 Printing & Reproduction | 66,000 |
66,000 |
0 |
| 25.1 Consulting Services | 610,000 |
610,000 |
0 |
| 25.2 Other Services | 740,000 |
740,000 |
0 |
| 25.3 Purchase of Goods & Services from Government Accounts | 5,302,000 |
5,241,000 |
(61,000) |
| 25.4 Operation & Maintenance of Facilities | 118,000 |
120,000 |
2,000 |
| 25.5 Research & Development Contracts | 1,382,000 |
1,474,000 |
92,000 |
| 25.6 Medical Care | 0 |
0 |
0 |
| 25.7 Operation & Maintenance of Equipment | 11,000 |
11,000 |
0 |
| 25.8 Subsistence & Support of Persons | 0 |
0 |
0 |
| 25.0 Subtotal, Other Contractual Services | 8,163,000 |
8,196,000 |
33,000 |
| 26.0 Supplies & Materials | 120,000 |
115,000 |
(5,000) |
| 31.0 Equipment | 116,000 |
110,000 |
(6,000) |
| 32.0 Land and Structures | 0 |
0 |
0 |
| 33.0 Investments & Loans | 0 |
0 |
0 |
| 41.0 Grants, Subsidies & Contributions | 50,964,000 |
50,788,000 |
(176,000) |
| 42.0 Insurance Claims & Indemnities | 0 |
0 |
0 |
| 43.0 Interest & Dividends | 0 |
0 |
0 |
| 44.4 Refunds | 0 |
0 |
0 |
Subtotal, Non-Pay Costs |
59,855,000 |
59,703,000 |
(152,000) |
NIH Roadmap for Medical Research |
593,000 |
805,000 |
212,000 |
Total Budget Authority by Object |
66,378,000 |
66,681,000 |
303,000 |
Includes FTEs which are reimbursed from the NIH Roadmap for Medical Research
OBJECT CLASSES |
FY 2006 Appropriation |
FY 2007 Estimate |
Increase or Decrease |
|---|---|---|---|
| Personnel Compensation: | |||
| Full-Time Permanent (11.1) | $3,569,000 |
$3,717,000 |
$148,000 |
| Other Than Full-Time Permanent (11.3) | 668,000 |
695,000 |
27,000 |
| Other Personnel Compensation (11.5) | 80,000 |
83,000 |
3,000 |
| Military Personnel (11.7) | 226,000 |
235,000 |
9,000 |
| Special Personnel Services Payments (11.8) | 53,000 |
55,000 |
2,000 |
| Total Personnel Compensation (11.9) | 4,596,000 |
4,785,000 |
189,000 |
| Civilian Personnel Benefits (12.1) | 1,129,000 |
1,173,000 |
44,000 |
| Military Personnel Benefits (12.2) | 205,000 |
215,000 |
10,000 |
| Benefits to Former Personnel (13.0) | 0 |
0 |
0 |
| Subtotal, Pay Costs | 5,930,000 |
6,173,000 |
243,000 |
| Travel (21.0) | 335,000 |
335,000 |
0 |
| Transportation of Things (22.0) | 21,000 |
21,000 |
0 |
| Rental Payments to Others (23.2) | 0 |
0 |
0 |
| Communications, Utilities and Miscellaneous Charges (23.3) | 70,000 |
72,000 |
2,000 |
| Printing and Reproduction (24.0) | 66,000 |
66,000 |
0 |
| Other Contractual Services: | |||
| Advisory and Assistance Services (25.1) | 610,000 |
610,000 |
0 |
| Other Services (25.2) | 740,000 |
740,000 |
0 |
| Purchases from Govt. Accounts (25.3) | 3,520,000 |
3,438,000 |
-41,000 |
| Operation & Maintenance of Facilities (25.4) | 162,000 |
165,000 |
(82,000) |
| Operation & Maintenance of Equipment (25.7) | 11,000 |
11,000 |
0 |
| Subsistence & Support of Persons (25.8) | 0 |
0 |
0 |
| Subtotal, Other Contractual Services | 4,999,000 |
4,919,000 |
(80,000) |
| Supplies and Materials (26.0) | 120,000 |
115,000 |
(5,000) |
| Subtotal, Non-Pay Costs | 5,611,000 |
5,528,000 |
(83,000) |
| Total, Administrative Costs | 11,541,000 |
11,701,000 |
160,000 |
Item
Tuberculosis Training - The Committee is please with the Fogarty International Center's efforts to supplement grants in the AIDS International Training and Research Program (AITRP) or International Training and Research Program in Emerging Infectious Diseases (ERID), which trains tuberculosis experts in the developing world. Given the magnitude of global tuberculosis, the Committee encourages FIC to consider developing a specific free-standing TB program (p. 99).
Action taken or to be taken
Given the impact of tuberculosis (TB) on the global health agenda, FIC has integrated TB research and training efforts across the spectrum of extramural programs, allowing leveraging of resources and multi-disciplinary approaches to tackle this urgent problem. TB continues to be an important focus of several FIC extramural programs, including: the Global Infectious Disease (GID) Research Training Program; the International Clinical, Operational, and Health Services Research and Training Award for AIDS and TB program (ICOHRTA AIDS/TB); the AIDS International Training and Research Program (AITRP); and the Stigma and Global Health Research program. In addition, TB research is also conducted within FIC's Tobacco Research program and the International Research Scientist Development Award (IRSDA) program for junior U.S. scientists. By building on infrastructure in place for a range of infectious diseases, the GID program allows TB researchers in low- and middle-income nations to leverage resources of a range of partners, including the National Institute of Allergy and Infectious Diseases (NIAID), the Centers for Disease Control and Prevention (CDC), and the Aeras Global TB Vaccine Foundation, supported by the Bill and Melinda Gates Foundation involving TB vaccine research in South Africa. By linking clinical, operational and health services research training on AIDS with that of TB, thet ICOHRTA AIDS/TB program allows FIC and its partner agencies, including the National Institute on Drug Abuse (NIDA), and also CDC and USAID, to bolster efforts in these linked epidemics in the developing world. Training and research on TB has been an important part of AITRP since its inception eighteen years ago.
In FY 2005 FIC added two new linked developing country/U.S. awards under its International Clinical Operational and Health Services Research Training Awards Program on AIDS and Tuberculosis (ICOHRTA AIDS/TB) involving Brazil and Zimbabwe, in addition to existing awards in China, Russia, Haiti, and Uganda which were funded in prior fiscal years. In FY 2006, FIC plans to convene a TB Network Meeting across all of its major TB-related programs in conjunction with a meeting of the National Tuberculosis Curriculum Consortium, supported by the National Heart Lung and Blood Institute.
Item
Chronic Obstructive Pulmonary Disease - The Committee notes that Chronic Obstructive Pulmonary Disease (COPD) is the fourth leading cause of death worldwide, and encourages the FIC expand its COPD research and training activities (p. 158).
Action taken or to be taken
The Fogarty International Center (FIC) continues to address chronic obstructive pulmonary disease (COPD) with the establishment in FY 2003 of the International Tobacco and Health Research and Capacity Building Program. The FIC and eight partners, including the National Cancer Institute and National Institute on Drug Abuse, made 14 awards to institutions working in 20 developing countries to support research and training on the impact of smoking-associated adverse health consequences. These awards will enhance the ability of scientists in low- and middle-income nations to understand risk factors for smoking uptake, particularly in youth, to develop effective prevention and mitigation programs, and to identify the most effective health service and communications policies to reduce the negative impacts of smoking on populations. Among the studies supported are those that focus on the use of the Internet for education related to smoking in rural Dominican Republic, economic analysis and smoking policies in China, smoking cessation in Syria, the use of water pipes in Egypt, and adolescent smoking prevention and cessation in South Africa. It should be noted that waterpipes are becoming more popular in the U.S. as well. The knowledge gained and interventions developed abroad through this program will benefit the United States since risk factors are similar in communities at home and abroad, and since effective interventions developed overseas may have particular effectiveness in U.S. groups. The FIC is pleased with progress under this program and publications are beginning to appear in the scientific literature based on support from this program. For example, in an article in the journal Lancet, authored by Jha and Peto, two FIC Principle Investigators, they were able to show a strong link between smoking and tuberculosis, indicating that TB was not only more common than expected in smokers, but also much more lethal. A recent publication in the American Journal of Public Health (June 2005, vol. 95, no. 6) indicates that this program is the most significant international tobacco research program in the world. FIC is planning to recompete this program in FY 2007 with an announcement for this recompetition planned to be issued in FY 2006.
In addition to the tobacco program, FIC is also addressing COPD under its International Training and Research in Environmental and Occupational Health (ITREOH) Program. The ITREOH is a collaborative program involving FIC and the National Institute of Environmental Health Sciences (NIEHS) within the NIH, and also the National Institute for Occupational Health and Safety (NIOSH) within the Centers for Disease Control and Prevention. Examples include efforts to reduce environmental and occupational health risks associated with mining and mineral processing in sub-Saharan Africa, in countries such as Zambia, Zimbabwe, and South Africa, as well as prevention of silicosis in Vietnam, and reduction of smoking and exposure to environmental tobacco smoke in China. For the first time, global programs are making in-roads with more coordinated efforts with the goal of educating people on the dangers of tobacco, thus reducing initial uptake as well as overall exposure, and thereby ultimately reducing illness and disease associated with tobacco use.
Item
Fragile X B: The Fogarty International Center addresses global health challenges through innovative and collaborative research and training programs and supports and advances the NIH mission through international partnerships. International collaboration among scientists is an essential element in Fragile X research. The Committee encourages the Fogarty International Center to consider Fragile X syndrome through all appropriate programs, such as the Fogarty International Research Collaboration Award and the FIC Brain Disorders in the Developing World Program (p. 99-100).
Action taken or to be taken
The Fogarty International Center was invited by Ms. Karen Fay, the Director of the Conquer Fragile X Foundation (CFXF:http://www.fragilex.org/cfxf/) to speak to their scientific advisory board and grantees during the annual Fragile X meeting, held at the Renaissance Hotel in Washington, DC, on June 26, 2004. This presentation entitled "Funding Opportunities for International Research in Fragile X Syndrome" highlighted a variety of FIC Programs in which Fragile X Syndrome could be addressed including Brain Disorders, Fogarty International Research Collaboration Award (FIRCA), Stigma, International Clinical, Operational, and Health Services Research and Training Award (ICOHRTA-I), Genetics, and International Research Scientist Development Award (IRSDA) programs. Participants were introduced to the FIC mission and website. Discussions were held on how the CFXF's international funding activities might synergize with NIH opportunities in this field. FIC staff had further follow-up discussions with a number of the Foundation's grantee regarding FIC funding opportunities.
FY 2006 Senate Appropriations Committee Report Language
Item
Fragile X B: The Committee encourages the Fogarty International Center to consider Fragile X syndrome through all appropriate programs, such as the Fogarty International Research Collaboration Award and the FIC Brain Disorders in the Developing World Program (p. 158, Senate).
Please refer above to the IC's response to the House for this Significant Item regarding Fragile X B.
Back to top| PHS Act/ Other Citation |
U.S. Code Citation |
2006 Amount Authorized |
FY 2006 Appropriation |
2007 Amount Authorized |
FY 2007 Budget Estimate |
|
|---|---|---|---|---|---|---|
Research & Investigation |
Section 301 |
42§241 |
Indefinite |
Indefinite |
||
International Cooperation |
Section 307 |
42§242I |
$66,378,000 |
$66,681,000 |
||
John E. Fogarty International Center |
Section 482 |
42§287b |
Indefinite |
Indefinite |
||
National Research Service Awards |
Section 487(d) |
42§288 |
0 |
0 |
||
Total, Budget Authority |
$66,378,000 |
$66,681,000 |
Fiscal Year |
Budget Estimate to Congress |
House Allowance |
Senate Allowance |
Appropriation 1/ |
|---|---|---|---|---|
| 1998 | 16,755,000 2/ | 27,620,000 | 28,468,000 | 28,289,000 |
| 1999 | 19,045,000 2/ 3/ | 30,367,000 | 35,426,000 | 35,426,000 |
| Rescission | 0 | 0 | 0 | (24,000) |
| 2000 | 23,498,000 2/ | 40,440,000 | 43,723,000 | 43,723,000 |
| Rescission | (229,000) | |||
| 2001 | 32,532,000 2/ | 50,299,000 | 61,260,000 | 50,514,000 |
| Rescission | (21,000) | |||
| 2002 | 56,449,000 | 56,021,000 | 57,874,000 | 56,940,000 |
| Rescission | (81,000) | |||
| 2003 | 63,088,000 4/ | 63,088,000 | 60,880,000 | 63,880,000 |
| Rescission | (415,000) | |||
| 2004 | 64,266,000 | 64,266,000 | 65,900,000 | 65,800,000 |
| Rescission | (418,000) | |||
| 2005 | 67,182,000 | 67,182,000 | 67,600,000 | 67,182,000 |
| Rescission | (550,000) | |||
| 2006 | 67,048,000 | 67,048,000 | 68,745,000 | 67,048,000 |
| Rescission | (670,000) | |||
| 2007 | 66,681,000 |
OFFICE/DIVISION |
FY 2005 Actual |
FY 2006 Appropriation |
FY 2007 Estimate |
|---|---|---|---|
| Office of the Director | 10 |
11 |
11 |
| Office of Administrative Management and International Services | 12 |
12 |
12 |
| Division of International Training and Research | 11 |
12 |
12 |
| Division of International Relations | 8 |
10 |
11 |
| Division of Advanced Studies and Policy Analysis | 5 |
5 |
5 |
| Division of International Epidemiology and Population Studies | 5 |
6 |
6 |
| Total | 51 |
56 |
57 |
Includes FTEs which are reimbursed from the NIH Roadmap for Medical Research.
FTEs supported by funds from Cooperative Research and Development Agreements. |
|||
FISCAL YEAR |
Average GM/GS Grade |
||
2003
2004
2005
2006
2007 |
11.1
11.0
11.6
11.6
11.6 |
||
GRADE |
FY 2005 Actual |
FY 2006 Appropriation |
FY 2007 Estimate |
|---|---|---|---|
| ES | 1 |
2 |
2 |
| Subtotal | 1 |
2 |
2 |
| Total - ES Salary | $150,696 |
$307,420 |
$313,568 |
| GM/GS-15 | 7 |
7 |
7 |
| GM/GS-14 | 10 |
11 |
11 |
| GM/GS-13 | 5 |
6 |
6 |
| GS-12 | 4 |
4 |
4 |
| GS-11 | 5 |
5 |
6 |
| GS-10 | 0 |
0 |
0 |
| GS-9 | 3 |
4 |
4 |
| GS-8 | 2 |
2 |
2 |
| GS-7 | 6 |
6 |
6 |
| GS-6 | 0 |
0 |
0 |
| GS-5 | 0 |
0 |
0 |
| GS-4 | 0 |
0 |
0 |
| GS-3 | 0 |
0 |
0 |
| GS-2 | 1 |
1 |
1 |
| GS-1 | 0 |
0 |
0 |
| Subtotal | 43 |
46 |
47 |
| Grades established by Act of July 1, 1944 (42 U.S.C. 207): | |||
| Assistant Surgeon General | 0 |
0 |
0 |
| Director Grade | 1 |
1 |
1 |
| Senior Grade | 1 |
1 |
1 |
| Full Grade | 0 |
0 |
0 |
| Senior Assistant Grade | 0 |
0 |
0 |
| Assistant Grade | 0 |
0 |
0 |
| Subtotal | 2 |
2 |
2 |
| Ungraded | 14 |
16 |
16 |
| Total permanent positions | 46 |
50 |
51 |
| Total positions, end of year | 60 |
66 |
67 |
| Total full-time equivalent (FTE) employment, end of year |
51 |
56 |
57 |
| Average ES salary | $150,696 |
$153,710 |
$156,784 |
| Average GM/GS grade | 11.6 |
11.6 |
11.6 |
| Average GM/GS salary | $79,884 |
$81,482 |
$83,112 |
FY 2007 |
|||
|---|---|---|---|
| Grade | Number | Annual Salary |
|
| Program Specialist | GS-9 |
1 |
$45,753 |
| Total Requested | 1 |
45,753 |
|
[1] Russell CJ & Webster, RG. The genesis of a pandemic influenza virus. Cell: Vol. 123 (3): 368-371, Nov. 4, 2005.
[2] UNAIDS AIDS Epidemic Update: December 2004, p. 2.
[4] Wilentz J (ed.), Fogarty at 35. NIH: May 2003.
[5] Global Fund to Fight AIDS, Tuberculosis and Malaria website at: http://www.theglobalfund.org/en/tuberculosis/
[6] Global Alliance for TB Drug Development website: http://www.tballiance.org
[7] Schwartzman K, Oxlade O, Barr RG, Grimard F, Acosta I, Baez J, Ferreira E, Melgen RE, Morose W, Salgado AC, Jacquet V, Maloney S, Laserson K, Pablos Mendez A, Menzies D: Domestic returns from investment in the control of tuberculosis in other countries. NEJM 353:1008-1020, 2005.
[8] Breman JG, Alillo MS, Mills A. Conquering the intolerable burden of malaria: What's new, what's needed: a summary. Am J. Trop Med Hyg, Aug 7, 1 (2 suppl): 1-15, 2004.
[9] Malaria Brochure, WHO Roll Back Malaria Department at www.who.int/malaria/docs/brochure_RBM.pdf.
[10] WHO Mental Health Fact Sheet at http://www.who.int/mental_health/en.
[11] WHO, Preventing Chronic Diseases: A Vital Investment (2005), pp. 2-6.
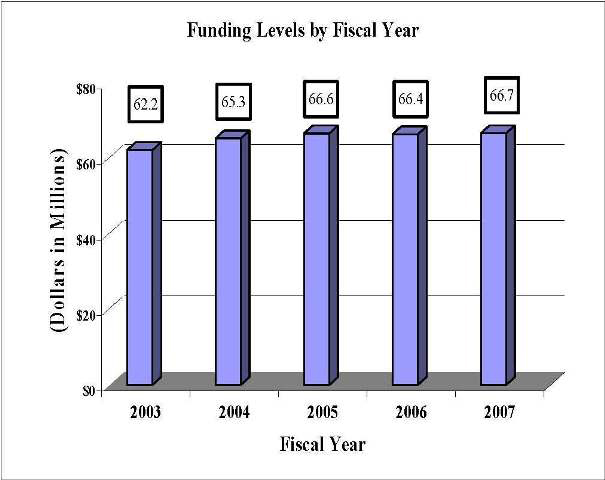
(Dollars in Millions)
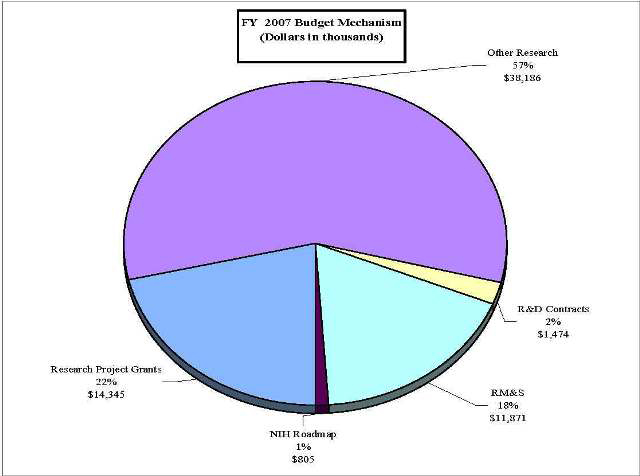
(Dollars in thousands)
| Programs | Funding | News | About | Questions? | Privacy Policy | Disclaimer | Accessibility | FOIA | Site Map |
| Fogarty International Center National Institutes of Health 31 Center Drive - MSC 2220 Bethesda, MD 20892-2220 USA |