Everything we do at NCI begins and ends with people—those with cancer, those at risk for the disease, and those who care for them. That singular focus lies at the heart of all our work in basic, translational, and clinical science to better treat cancer; our outreach into communities across the United States; and our efforts to build cancer prevention strategies and programs. People with cancer are not just "patients" to us. They are human beings with family, friends, dreams, and lives that are all impacted by their diagnoses. Cancer patients are the cornerstone of cancer research, and we are forever indebted to those men and women who give so generously of themselves to make life better for others.

Cancer, as a disease, is incredibly complex, both in its biology and in its social impact. We now know that cancer is not a single disease or even a small group of related diseases. Rather, we are finding that when viewed at the level of genes and proteins, cancer is a collection of many different diseases. It is this greater understanding of cancer at the molecular level that NCI believes will enable us to change the meaning of a cancer diagnosis in the future. The National Cancer Act of 1971 established the National Cancer Program and authorized NCI to coordinate its efforts. Encompassing academia, industry, the private sector, international partners, and other government agencies, NCI directs a massive multifaceted effort against cancer that continually strives to match the enormity of the disease itself.
NCI is dedicated to the understanding, diagnosis, treatment, and prevention of cancer for all people. To these ends, NCI creates connections: basic science to clinical therapies; researchers to patients and doctors; NCI internal ("intramural") work and external ("extramural") efforts; public and private cancer-related institutions and research; and the U.S. effort to the wider global fight against cancer.
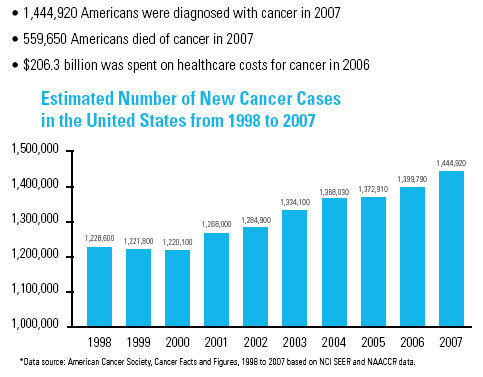
We have made progress, but much work remains. The rate of cancer mortality continues to drop; however, cancer still remains a leading cause of death, second only to heart disease. The number of new cancer diagnoses continues to rise, with more than 1.4 million people hearing the dreaded words "you have cancer" this year in the United States alone. And we know this burden is disproportionately shouldered by the poor, the elderly, and minority populations.
Our progress is thanks to the work of thousands of cancer researchers, both at the lab bench and in the clinic, and numerous patients who seek not only treatment for themselves but also to provide hope for others. As we now understand that cancer is a disease that results from changes in our genes, we are striving to comprehend the precise changes that occur before we are born or as we interact with our environment, and how to prevent or overcome them. We have pried open some of the secrets of how cancer begins, how it takes advantage of our normal biological makeup, and how it initiates its lethal spread, and we are pursuing potential new avenues to learn to stop it in its tracks.
Each step forward we take opens up promising new opportunities to make further progress, which must be seized. NCI cannot do this alone. Thus, it is essential that NCI increase its capacity to enable and support the many critical connections that will bring about real changes in cancer prevention, diagnosis, and treatment, all the while ensuring that the latest scientific advances become available to all patients, not just those who have access to the NIH Clinical Center or other leading national cancer centers.
Making these connections is not an easy task, and it is made even more difficult in light of the budgetary realities we face. Nearly 80 percent of our annual funding goes to support external scientists and researchers at academic institutions and centers across the country, including many who conduct the clinical trials necessary to translate basic scientific findings into cancer treatments. Much of the remainder supports our internal research operation, which facilitates collaborative opportunities between world class scientists, both at NCI and elsewhere, provides freedom to pursue new insights and opportunities (particularly for underserved populations), and trains and develops the next generation of cancer researchers.
The below-inflation budgets of the last two years have impacted both our internal and external capabilities. Indeed, implications of our budgetary constraints have carried beyond the basic research laboratories, impacting the clinical research options available to patients. For example, the NCI's Clinical Trial Cooperative Groups, which promote and support clinical trials of new cancer treatments, explore methods of cancer prevention and early detection, and study quality-of-life issues and rehabilitation during and after treatment, saw their funding cut by 10.9 percent between fiscal year 2002 and 2006. Although some of their lost funding was restored in FY 2007, fewer trials have been started, and fewer patients have been enrolled in available trials. This slows our ability to improve the standard of care for cancer patients through new drugs, devices, or interventions.