|
 |
Filoviruses
 View PDF (128KB) View PDF (128KB)
| What
are filoviruses? |
 |
|
| Filoviruses
belong to a virus family called Filoviridae and can cause severe hemorrhagic
fever in humans and nonhuman primates. So far, only two members
of this virus family have been identified: Marburg virus and Ebola
virus. Four species of Ebola virus have been identified: Ivory Coast,
Sudan, Zaire, and Reston. Ebola-Reston is the only known filovirus
that does not cause severe disease in humans; however, it can be fatal
in monkeys.
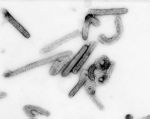
Structurally,
filovirus virions (complete viral particles) may appear in several
shapes, a biological feature called pleomorphism. These shapes include
long, sometimes branched filaments, as well as shorter filaments
shaped like a "6", a "U", or a circle. Viral
filaments may measure up to 14,000 nanometers in length, have a
uniform diameter of 80 nanometers, and are enveloped in a lipid
(fatty) membrane. Each virion contains one molecule of single-stranded,
negative-sense RNA. New viral particles are created by budding from
the surface of their hosts’ cells; however, filovirus replication
strategies are not completely understood.
|
|
|
|
 |
|
Negative
stain image of an isolate of Marburg virus, showing filamentous
particles as well as the characteristic "Shepherd's Crook".
Magnification approximately 100,000 times. Image courtesy
of Russell Regnery, Ph.D., DVRD, NCID, CDC. Go
to high-resolution version.
|
|
|
|
|
|
|
|
|
 |
|
|
| When
were the members of the filovirus family first recognized? |
|
|
The first filovirus
was recognized in 1967 when a number of laboratory workers in Germany
and Yugoslavia, who were handling tissues from green monkeys, developed
hemorrhagic fever. A total of 31 cases and seven deaths were associated
with these outbreaks. The virus was named after Marburg, Germany,
the site of one of the outbreaks.
After the initial
outbreaks, the virus disappeared. It did not reemerge until 1975,
when a traveler, most likely exposed in Zimbabwe, became ill in
Johannesburg, South Africa. The virus was transmitted there
to his traveling companion and a nurse. A few sporadic cases of
Marburg hemorrhagic fever have been identified since that time.
Ebola virus
was first identified in 1976 when two outbreaks of Ebola hemorrhagic
fever (Ebola HF) occurred in northern Zaire (now the Democratic
Republic of Congo) and southern Sudan. The outbreaks involved what
eventually proved to be two different species of Ebola virus; both
were named after the nations in which they were discovered. Both
viruses showed themselves to be highly lethal, as 90% of the Zairian
cases and 50% of the Sudanese cases resulted in death.
Since 1976,
Ebola virus appeared sporadically in Africa, with small to midsize
outbreaks confirmed between 1976 and 1979. Large epidemics of Ebola
HF occurred in Kikwit, Zaire in 1995 and in Gulu, Uganda in 2000.
Smaller outbreaks were identified in Gabon between 1994 and 1996.
For information on known Ebola HF cases and outbreaks, please refer
to the chronological list .
|
|
|
 |
|
In
the isolation area during the Kikwit, Zaire outbreak of Ebola HF.
|
|
|
|
|
|
| What
are the natural hosts of filoviruses? |
|
It appears that filoviruses
are zoonotic, that is, transmitted to humans from ongoing life cycles
in animals other than humans. Despite numerous attempts to locate the
natural reservoir or reservoirs of Ebola and Marburg viruses, their origins
remain undetermined. However, because the virus can be replicated in some
species of bats, some types of bats native to the areas where the virus
is found may prove to be the viruses’ carriers.
| How
are filoviruses spread? |
|
In an outbreak or
isolated case among humans, just how the virus is transmitted from the
natural reservoir to a human is unknown. Once a human is infected, however,
person-to-person transmission is the means by which further infections
occur. Specifically, transmission involves close personal contact between
an infected individual or their body fluids, and another person. During
recorded outbreaks of hemorrhagic fever caused by filovirus infection,
persons who cared for (fed, washed, medicated) or worked very closely
with infected individuals were especially at risk of becoming infected
themselves. Nosocomial (hospital) transmission through contact with infected
body fluids – via reuse of unsterilized syringes, needles, or other
medical equipment contaminated with these fluids – has also been
an important factor in the spread of disease. When close contact between
uninfected and infected persons is minimized, the number of new
filovirus infections in humans usually declines. Although in the laboratory
the viruses display some capability of infection through small-particle
aerosols, airborne spread among humans has not been clearly demonstrated.
During outbreaks,
isolation of patients and use of protective clothing and disinfection
procedures (together called viral hemorrhagic fever isolation precautions
or barrier nursing) has been sufficient to interrupt further transmission
of Marburg or Ebola viruses, and thus to control and end the outbreak.
Because there is no known effective treatment for the hemorrhagic fevers
caused by filoviruses, transmission prevention through application of
VHF isolation precautions is currently the centerpiece of filovirus control.
In conjunction with
the World Health Organization, CDC has developed practical, hospital-based
guidelines, titled Infection Control for Viral
Haemorrhagic Fevers In the African Health Care Setting. The
manual can help health-care facilities recognize cases and prevent further
hospital-based disease transmission using locally available materials
and few financial resources.
|
 |
|
|
| Related
Links |
|
|
|
|
|
| Glossary |
| Unsure
about some of the terms used on this page? Visit our glossary
of terms for help. |
|
|
|
|
|