
Table of Contents
Streptococcus pneumoniae (S. pneumoniae or "pneumococcus") is a bacterium commonly found in the nasopharynx (back of the nose) of healthy people. More than 90 serotypes of S. pneumoniae have been identified. Serotypes of pneumococcus are identified on the basis of differences in the polysaccharide (sugar) capsule of the organism. The presence of pneumococcus in the nasopharynx is referred to as "carriage". Most people have been carriers of S. pneumoniae at some point in their lives. Pneumococcal carriage is more common in young children, is usually transient and generally causes no illness. S. pneumoniae is an exclusively human pathogen and is spread from person-to-person by respiratory droplets, meaning that transmission generally occurs during coughing or sneezing to others within 6 feet of the carrier. Thus, carriers of S. pneumoniae, while generally healthy, are an important source of infection and disease for others.
Occasionally, S. pneumoniae will spread from the nasopharynx of a colonized person into other parts of the body and cause diseases, including otitis media (ear infections), sinusitis (sinus infections) and pneumonia (lung infections). In addition, S. pneumoniae can sometimes get into places in the body that are normally sterile (free of bacteria) including the blood, causing bacteremia, or the lining of the brain and spinal cord, causing meningitis. When pneumococci get into these sterile places in the body, it is called "invasive" pneumococcal disease. A relatively small number of serotypes of S. pneumoniae account for most invasive disease. Invasive pneumococcal infections can result in serious complications or death.
Worldwide, S. pneumoniae is the most common cause of bacterial meningitis, community-acquired pneumonia, bacteremia and otitis media. Certain populations in the United States, including Alaska Natives, have very high rates of pneumococcal disease [1].
Further information about S. pneumoniae can be found at CDC
Division of Bacterial and Mycotic Diseases - Streptococcus pneumoniae
Disease
What is antibiotic-resistant Streptococcus pneumoniae?
In the 1940s, penicillin antibiotics became available and were used effectively to treat pneumococcal infections. During the 1960s, however, the first pneumococcal bacteria that were not susceptible ("resistant") to penicillin were discovered in humans [2]. Since then, penicillin resistant pneumococcal bacteria have been reported all over the world. By the late 1970s, pneumococci that were resistant to other types of antibiotics in addition to penicillins were reported [3]. These "multidrug resistant" pneumococci have now been reported all over the world [4].
Further information about antibiotic-resistant S. pneumoniae can be found at CDC Get Smart - General Information about Antibiotic Resistance
Further information on the mechanisms of acquired resistance among pneumococcal organisms can be found by searching CDC database.
What is the concern about antibiotic-resistant Streptococcus pneumoniae?
Antibiotic-resistant pneumococcal infections are difficult and expensive to treat. Treatment failures for disease caused by antibiotic-resistant Streptococcus pneumoniae have been reported. Antibiotic-resistant S. pneumoniae infections may require higher doses of antibiotic, longer duration of treatment and hospitalization, the use of more expensive medications, or use of medications with greater side-effect potential. The spread of these resistant bacteria increased dramatically during the 1990s. Understanding the evolution of resistant pneumococci and their spread among people is critical to developing effective prevention strategies and is an extremely important public health priority.
Streptococcus pneumoniae in Alaska
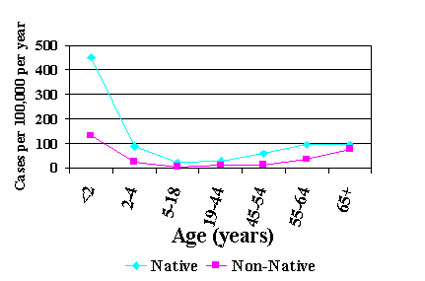
In Alaska, S. pneumoniae is one of the leading causes of bacteremia, pneumonia, meningitis, otitis and sinusitis. Alaska Natives, particularly those less than 2 and greater than 65 years of age have among the highest rates of invasive pneumococcal disease of any population worldwide [5] [Fig. 1]. Risks associated with invasive pneumococcal disease among Alaska Natives < 2 years of age include prior pneumonia or hospitalization, group child care center, a tobacco smoker or chewer in the household, lack of breast feeding, and certain underlying medical conditions [5,6]. Among Alaska Native adults 20-64 the major risk factor is alcoholism and among those aged 65 years and older, risk factors include underlying medical conditions including chronic lung disease, anemia and heart disease [5].
As in other parts of the world, drug-resistant pneumococci have been detected in Alaska. The first pneumococcal bacteria that were resistant to penicillin were detected in Alaska in the 1980s [7]. Since then, pneumococci that have decreased susceptibility to penicillin have become widespread throughout the state [8]. In other parts of the world, an association between antibiotic use and carriage or infection with resistant pneumococci organisms has been identified. The role of antibiotic use and other risks factors in emerging resistant pneumococcal carriage and disease among Alaska Natives is currently under investigation.
High rates of invasive pneumococcal infections and widespread resistant organisms
are a great concern to Alaskans and Alaskan health care providers. Several
studies are ongoing in Alaska to characterize invasive pneumococcal disease,
including monitoring trends in antibiotic-resistant organisms, and designing
and evaluating prevention strategies.
Figure 1. Rates of invasive pneumococcal disease in Alaska by age, 1986 - 2000.
Pneumococcal polysaccharide vaccines have been available in the United States since 1977. Currently, a 23-valent vaccine (the 23 serotypes most likely to cause invasive disease) is available for use in persons greater than 2 years of age. In Alaska, this vaccine is routinely administered to persons 55 years of age or older to prevent invasive pneumococcal disease. Polysaccharide vaccines are also used in younger persons who are at high risk for serious outcomes from pneumococcal disease including persons with sickle cell disease, HIV infection and certain medical conditions. Vaccination is currently our best strategy to prevent invasive pneumococcal disease in these populations.
Although polysaccharide pneumococcal vaccines have been available for many years, they are not effective in young children. In 2000, a 7-valent protein-polysaccharide pneumococcal vaccine (Prevnar®), which is effective in young children, was licensed by the Food and Drug Administration. In January 2001, the State of Alaska made this vaccine available for children < 5 years of age. Two years after the introduction of vaccine, rates of invasive pneumococcal disease among Alaska Native children caused by serotypes in Prevnar® declined by 90% [9]. This suggests that vaccination of young children might be the key to decreasing rates of disease in this population.
Along with vaccination, characterizing antibiotic use patterns and the relationship between antibiotic use and carriage or disease with resistant pneumococci among Alaskans is an ongoing prevention activity. Several epidemiologic studies have demonstrated an association between frequent or prolonged use of antibiotics and drug-resistant pneumococcal carriage [4]. Addressing the appropriate use of antibiotics in Alaskan communities may be critical to preventing or decreasing the rate at which pneumococci become resistant.
Finally, on-going surveillance for invasive pneumococcal disease helps to evaluate vaccine effectiveness and monitor bacterial changes. Studies to assess for pneumococcal carriage help to determine transmission patterns of drug-resistant bacteria, possible emergence of new serotypes, and assess the effectiveness of vaccines in preventing carriage and disease.
Recommendations for the use of pneumococcal vaccines in Alaska can be found at State of Alaska Health and Social Services - Alaska Immunization Program.
Information and materials regarding judicious use of antimicrobial agents
are available at: CDC
Get Smart - General Information about Antibiotic Resistance.
1. CDC. Prevention of pneumococcal disease: Recommendations
of the Advisory Committee on Immunization Practices (ACIP). MMWR 1997; 46
(no.RR-08).
2. Hansman D, Devitt L, Miles H, Riley I. . Pneumococci
relatively insensitive to penicillin from Australia and New Guinea. Med J
Aust 2 1974: 353-356.
3. Jacobs MR, Koornhof HJ, Robins-Browne RM, Stevenson
CM, Vermack ZA, et al. Emergence of multiply resistant pneumococci. N Engl
J Med 299 1978: 735-740.
4. Hennessy TW, Petersen KM, Bruden D, et al. Changes in
antibiotic prescribing practices and carriage of penicillin-resistant Streptococcus
pneumoniae: a controlled intervention trial in rural Alaska. Clin Infect
Dis 2002;34:1543-1550.
5. Davidson M, Parkinson AJ, Bulkow LR et al. The epidemiology
of invasive pneumococcal disease in Alaska, 1986-1990 -ethnic differences
and opportunities for prevention. J Infect Dis. 1994; 170:368-76.
6. Gessner BD, Ussery XT, Parkinson AJ, et al. Risk factors
for
invasive disease caused by Streptococcus pneumoniae among Alaska native
children younger than two years of age. Pediatr Infect Dis J, 1995;14:123-8.
7. Parkinson AJ, Davidson M, Fitzgerald MA, et al. Serotype
distribution and antimicrobial resistance patterns of invasive isolates of
S. pneumoniae: Alaska 1986-90. J Infect Dis 1994;170:461-4.
8. Rudolph, KM, Parkinson AJ, Reasonover AL, Bulkow LR,
Parks DJ Butler JC. Serotype distribution and antimicrobial resistance
patterns of invasive isolates of S. pneumoniae: Alaska 1991-8. J Infect
Dis 2000; 490-6.
9. Singleton R, Butler JC, Hennessy T, et al. Pneumococcal
disease in Alaska Native children 2 years after statewide routine vaccination
with 7-valent pneumococcal vaccine. Poster 37th National Immunization Conference
March 17-20, 2003, Chicago.