| Oregon Case Report: 05OR005 |
March 23, 2006 |
Summary
On March 17, 2005, a 61-year-old woodworker operating a glue-press machine
at a wood-products firm was killed while attempting to replace a glue
tray while the machine was running. The glue tray had been removed to
correct a glue-dripping problem. The press operator instructed another
worker to finish processing a product that was already in the press, while
he and a new coworker attempted to reattach the glue tray. The press operator
put his head between the frame and the closed top lid of the press in
order to see where to latch the glue tray. While he was in this position,
the top plate suddenly lifted at the end of a programmed automatic cycle,
and crushed the operator’s head against the frame. Coworkers witnessed
the event and immediately extricated the operator from the machine. The
victim was transported to the hospital, where he was pronounced dead.
|
The glue press operates on an automatic
cycle, with a conveyor running beneath a glue roller and into the
press. |
Recommendations
- Completely shut down and lockout machinery before conducting maintenance.
- Employers should develop, implement, and enforce a comprehensive hazardous
energy program.
- Ensure that all machinery moving parts and pinch points are fully
guarded.
- Employers should conduct regular hazard surveys and follow through
with corrective action.
- Employers should investigate on-the-job injuries and review work procedures
in order to correct hazards and prevent similar incidents.
- Employers should implement a preventive maintenance program for machinery,
with designated, trained personnel authorized to perform maintenance
tasks.
Introduction
On March 17, 2005, a 61-year-old woodworker operating a radio-frequency
glue-press machine was killed while attempting to replace a glue tray
while the machine was running. OR-FACE received notification of the incident
on July 20, 2005. An employer interview and onsite visit were requested
but not granted. This report is based on reports from emergency responders,
the medical examiner, and Oregon OSHA.
The employer is an Oregon wood-products firm with about 300 employees,
specializing in the operation of sawmills, planer mills, and wood remanufacturing.
The fatality occurred at the wood-products remanufacturing location, where
custom wood products are produced to a customer’s specifications.
Dimensional wood is sawed and sanded, then run through a glue machine
before being recut and resanded, palletized and shrink-wrapped for shipping.
The manufacturing plant has 46 employees, working two 8-10 hour shifts,
5 days a week.
According to the OR-OSHA investigation, the employer had a written safety
and hazardous-energy control program, but it was not implemented. Only
the shift supervisors, the day-shift press operator, and the plant manager
were trained in lockout procedures. Comprehensive training on safety procedures
was not provided to all machine operators and supervisors. Lockout was
not performed by employees while equipment was worked on, maintained,
adjusted, unjammed, or during cleanup activities.
Although the facility had a safety committee, members of the committee
were not trained, nor active in hazard identification. No periodic safety
inspections were conducted, and no procedures existed for the investigation
of on-the-job injuries. Three weeks prior to the March 17 fatality, a
glue-press worker was seriously injured when caught in the unguarded glue
rolls while cleaning up without locking out the machine. No lockout training,
installation of machine guards, or other corrective action was undertaken
following that incident.
On each shift, the glue-press machine is run by one operator and two
helpers. The operator in this incident had 1 year of experience as the
night-shift glue-press operator. The operator had not received lockout
or equipment maintenance training. The new coworker helping him had been
on the job only 15 minutes when the incident occurred.
Investigation
The 1960’s model radio-frequency glue-press machine, purchased
used by the employer, has conveyor on-load and off-load tables. The machine’s
chain and sprocket conveyor system pushes pre-cut wood to be glued into
the press. A gluing roller with a detachable glue pan is connected to
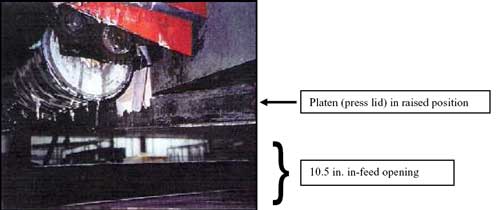
the upper frame assembly by pins, and latched. The in-feed opening to
the electric heat press is 10.5 in. high. A hydraulically powered lid,
called a platen, automatically depresses and rises during a programmed
cycle. The gap between the depressed platen and the upper frame of the
machine is 8.5 in.
At the time of the incident, the glue-press conveyor chain and sprocket
system, press opening, glue feed rolls, and loading-table mechanisms were
unguarded. A makeshift repair to correct a glue-dripping problem had been
made by the operator 2 weeks earlier, using a piece of duct tape to hold
a piece of wood veneer to direct dripping glue from the roller into the
glue tray. The glue tray in front of the press in-feed had been removed
to correct the glue-dripping problem.
The press conveyor had multiple start buttons. The control panel containing
an emergency stop button was located at one side of the press. A second
emergency stop was located at the end of the off-load table. The electrical
panel providing power to the machine was 50 ft away.
|
| A close-up view of the
glue press in-feed opening shows the platen above, and the glue
roller in front with a piece of duct tape attached. |
The glue-press operator was working with two coworkers. He instructed
one coworker to finish processing a product that was already in the press,
while he and the new coworker attempted to reattach the glue tray. The
platen cycle was set to automatically depress and rise every 80 seconds.
Attempting to reattach the glue tray while the glue press was running,
the operator had difficulty finding the latch, and put his head into the
8.5 in. gap between the frame and the depressed platen to see it. While
he was in this position, the platen suddenly opened and crushed the operator’s
head against the frame above. He fell to one side, dropping his end of
the heavy glue tray.
The new coworker assisting with the glue tray was unable to see the press
operator from her position on the other side of the machine. She was unable
to hold the tray alone, and dropped it and called to the operator. Getting
no response, she called coworkers for help. A responding supervisor went
to the other side of the glue press to shut it off at the main power disconnect
50 ft away, and began pushing relief valves to release the hydraulic pressurized
lid. The victim was extricated from the machine by coworkers. Emergency
responders transported the victim to the hospital, where he was pronounced
dead.
Cause of Death
Traumatic brain injury
Recommendations/Discussion
Recommendation #1: Completely shut down and lockout machinery before
conducting maintenance.
Machine maintenance should never be conducted while a machine is running,
except in limited cases where operation is a necessary part of a routine
maintenance procedure and the worker is not exposed to hazardous energy.
Recommendation #2. Employers should develop, implement, and enforce a
comprehensive hazardous energy program.
A comprehensive hazardous energy program includes written safe operating
procedures for shutting down, de-energizing, and locking out machinery,
particularly during maintenance activities (29 CFR 1910.147). A tagout
program provides an additional level of safety by preventing the equipment
from being re-energized by a coworker. Some companies have a tagout system
with a photo of the employee to help identify whose tagout is on the equipment.
All machine operators, maintenance personnel, and supervisors should be
well trained in lockout/tagout procedures, and employers need to consistently
reinforce these procedures.
Recommendation #3. Ensure that all machinery moving parts, shear, and
pinch points are fully guarded.
Employers need to assess all machinery, especially older machinery, and
install guards to prevent access to all moving, shear, and pinch points.
In this incident, the glue press was an older machine, manufactured without
guards, but a retrofit guard is available through the press manufacturer.
In cases where specific retrofit guards are not available, private suppliers
can provide a wide variety of guards to bring older machinery into compliance
with safety standards.
Recommendation #4. Employers should conduct regular hazard surveys and
follow through with corrective action.
A firm’s safety committee should perform a hazard survey of the
workplace and a job safety analysis to identify hazards and unsafe work
practices. In this case, the company had a written lockout program, but
the procedures were not implemented at this site and periodic inspections
were not performed. A hazard survey is best performed regularly. Corrective
actions should be set with a schedule for completion. A job safety analysis
provides additional information by tracking each step in a work process,
identifying safe work procedures and necessary personal protection equipment.
Employee safety training and retraining should incorporate the results
of the job safety analysis. Employers need to maintain written records
related to hazardous-energy program training, in order to promote adequate
and accurate training, and promote compliance by both supervisors and
front-line workers. Employee retraining must be conducted whenever there
is reason to believe an employee has inadequate knowledge of or deviates
from the use of safe procedures.
Recommendation #5. Employers should investigate on-the-job injuries and
review work procedures in order to correct hazards and prevent similar
incidents.
This incident emphasizes the importance of using a safety committee to
investigate and respond to on-the-job injuries. The employer had experienced
a similar, though less severe incident on the glue press 3 weeks prior
to the fatality. Investigation of injury incidents is crucial to the maintenance
of an effective safety and training program. Data collected regarding
these incidents can provide employers with the necessary information to
implement corrective action related to engineering controls, employee
work habits, and revised safe-work procedures. An investigation of the
nonfatal incident may have identified a hazard and led to corrective action.
Recommendation #6. Employers should implement a preventive maintenance
program for machinery, with designated, trained personnel authorized to
perform maintenance tasks.
Employers need to ensure that only authorized, competent, and trained
personnel perform maintenance on machinery. In this case, there was no
designated maintenance person for the machinery. The glue-press operator
was not a trained mechanic, and by report had not been instructed in safe
operating procedures for maintenance activities.
References
- Center for Research on Occupational and Environmental Toxicology.
(n.d.). Lockout/Tagout. Online resource: http://www.croetweb.com/links.cfm?subtopicID=250
- Center for Research on Occupational and Environmental Toxicology.
(n.d.). Machine guarding. Online resource: http://www.croetweb.com/links.cfm?subtopicID=251
- National Institute for Occupational Safety and Health. (1999). Preventing
worker deaths from uncontrolled release of electrical, mechanical, and
other types of hazardous energy. Available online: http://www.cdc.gov/niosh/99-110.html
- Occupational Safety and Health Administration. (2005). Control
of hazardous energy (lockout/tagout). Online resource: http://www.osha.gov/SLTC/controlhazardousenergy/index.html
- Oregon OSHA. (2006). Machine safeguarding at the point of operation
[Pub 440-2980]. Available online: http://www.cbs.state.or.us/external/osha/pdf/pubs/2980.pdf
- Oregon OSHA. (2005). Safety committees for the real world.
Available online: http://www.cbs.state.or.us/external/osha/pdf/pubs/2341.pdf
Oregon FACE Program
CROET at OHSU performs OR-FACE investigations through a cooperative agreement
with the National Institute for Occupational Safety and Health (NIOSH),
Division of Safety Research. The goal of these evaluations is to prevent
fatal work injuries in the future by studying the work environment, the
worker, the task, the tools, the fatal energy exchange, and the role of
management in controlling how these factors interact.

To contact Oregon
State FACE program personnel regarding State-based FACE reports, please
use information listed on the Contact Sheet on the NIOSH FACE web site.
Please contact In-house
FACE program personnel regarding In-house FACE reports and to gain
assistance when State-FACE program personnel cannot be reached.
Oregon FACE reports are for information, research, or occupational injury
control only. Safety and health practices may have changed since the investigation
was conducted and the report was completed. Persons needing regulatory
compliance information should consult the appropriate regulatory agency.
|