|
|
|
|||||||||||||||||
|
|||||||||||||||||
|
Dispatch Pathologic Studies of Fatal Cases in Outbreak of Hand, Foot, and Mouth Disease, TaiwanWun-Ju Shieh,* Shih-Ming Jung,† Chuen Hsueh,† Tseng-Tong Kuo,† Anthony Mounts,* Umesh
Parashar,* Chen Fu Yang,* Jeannette Guarner,*
Thomas G. Ksiazek,* Jacqueline Dawson,* Cynthia Goldsmith,* Gwong-Jen J. Chang,* Steve M.
Oberste,* Mark A. Pallansch,* Larry J. Anderson,*
Sherif R. Zaki,* and the Epidemic Working Group (1)
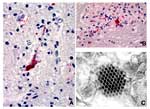
During April through July 1998, an outbreak of hand, foot, and mouth disease occurred in Taiwan; enterovirus 71 (EV71) was identified as the main etiologic agent. The outbreak was associated with an unusually high death rate in young children. At least 55 fatal cases were initially reported (1,2) in healthy children, who developed refractory shock after an acute prodromal illness; many of them manifested neurologic disorders during illness and died within 24 hours of hospitalization (3). In many fatal cases, EV71 was indicated as the etiologic agent by serologic, virologic, and polymerase chain reaction tests conducted on specimens from nonsterile sites, such as throat swabs or stool specimens. While these results may indicate a precedent EV71 infection in the fatal cases, they do not directly implicate EV71 as the causative agent of neurologic disorders and eventual death. In contrast, histopathologic examination in conjunction with special pathology techniques, such as immunohistochemistry (IHC), in situ hybridization, and electron microscopy, can provide unequivocal evidence linking a particular agent to death. We report results of pathologic examination of two fatal cases during this outbreak. The Study
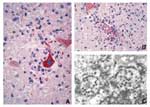
The clinical and histopathologic features of the first case were initially reported by Chang et al. (4); the second case was in a patient admitted to the same hospital with a similar clinical course. Histopathologic features were similar in both cases and showed severe and extensive encephalomyelitis. An IHC technique using a monoclonal mouse anti-EV71 antibody and an in situ hybridization test using a digoxigenin-labeled enterovirus probe were performed on formalin-fixed, paraffin-embedded central nervous system (CNS) tissues and major organs of both cases. In the first case, positive staining of enteroviral antigens and nucleic acids was observed in neurons, neuronal processes, and inflammatory foci at various CNS sites, including the cerebral cortex, brain stem, and all levels of spinal cord (Figure 1A, B). No immunostaining or hybridization was present in lung, heart, liver, spleen, or kidney. Electron microscopy evaluation of spinal cord tissues showed a highly vacuolated neuron containing scattered picornavirus-like particles and viral inclusions (Figure 1C). The second case was negative for EV71 by IHC, in situ hybridization, polymerase chain reaction, and viral isolation. An IHC test using an anti-Japanese encephalitis antibody showed intense immunostaining of flaviviral antigens in neurons, neuronal processes, and inflammatory foci at various CNS sites (Figure 2A, B). No immunostaining of flavivirus was present in other major organs. Further study was conducted by injecting neurologic tissue of the patient into suckling mice. CNS material from an inoculated mouse was passed onto Vero-E6 cells and produced cytopathic effect. Electron microscopy examination of mouse brain and infected cell culture revealed flavivirus particles (Figure 2C), and polymerase chain reaction with sequencing confirmed the isolate as Japanese encephalitis virus. ConclusionsIn addition to classic hand, foot, and mouth disease, EV71 can cause severe CNS infections with a high death rate (5). Two previous EV71 outbreaks were associated with neurologic disorders and increased deaths; the first one occurred in Bulgaria in 1975 (5) and the second in Malaysia in 1997 (1,6). The neurologic disorders and clinical courses of acute viral CNS infections can be very similar regardless of causative agents, and definitive diagnoses are sometimes very difficult to establish without further pathologic studies. A definitive laboratory and pathologic diagnosis is crucial for implementing effective measures to control an outbreak (7); the Nipah virus encephalitis outbreak in Malaysia (8,9) and the West Nile encephalitis outbreak in New York City (10,11) lend additional support to this statement. Our report illustrates how two different etiologic agents can cause similar diseases during an outbreak and emphasizes the need for postmortem examination. Dr. Shieh is a staff pathologist, Division of Viral and Rickettsial Diseases, Centers for Disease Control and Prevention. His research interests include infectious disease pathology, pathology and pathogenesis of viral encephalitides, molecular epidemiology, and infectious disease outbreak investigations. Address for correspondence: Wun-Ju Shieh, Centers for Disease Control and Prevention, 1600 Clifton Road, Mail Stop G32, Atlanta, GA 30333, USA: fax: 404-639-3043; e-mail: wshieh@cdc.gov. References
1. Epidemic Working Group at Centers for Disease Control and Prevention: Jim Alexander, Betty Brown,
David Shay, Patricia Greer, Charles Humphrey, Tim Morken; Tara Ferebee-Harris. |
||||||||||||||||||||||||||||||||
Home | Top of Page | Current Issue | Expedited | Upcoming Issue | Past Issue | EID Search | Contact Us CDC Home | Search | Health Topics A-Z This page last reviewed February 20, 2001 Emerging Infectious Diseases Journal |