| Remember: Children have 2-9 viral respiratory illnesses
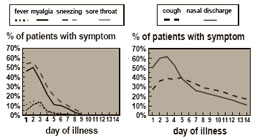
per year.2 In uncomplicated colds, cough and nasal
discharge may persist for 14 days or more –
long after other symptoms have resolved Duration of symptoms in 139 rhinovirus colds3 Controlled studies do not support antibiotic
treatment of mucopurulent rhinitis.4 Antibiotics do not effectively treat URI, or
prevent subsequent bacterial infections.5 Don’t overdiagnose sinusitis Though most viral URIs involve the
paranasal sinuses, only a small minority are
complicated by bacterial sinusitis. Avoid unnecessary treatment by using
strict criteria for diagnosis:5 Symptoms of rhinorrhea or persistent daytime
cough lasting more than 10 - 14 days
without improvement. or Severe symptoms of acute sinus infection:
- fever (> 39 C) with purulent nasal discharge
- facial pain or tenderness
Treating sinusitis:
- Target likely organisms with first-line drugs:Amoxicillin, Amoxicillin/Clavulanate6
- Use shortest effective course:Should see improvement in 2-3 days. Continue treatment for 7 days after symptoms improve or resolve (usually a 10 - 14 day course).7
- Consider imaging studies in recurrent or unclear cases:But remember that some sinus involvement is frequent early in the course of uncomplicated viral URI - so interpret studies with caution.
Share the CDC/AAP principles and pamphlets with parents to help them understand when antibiotic treatment risks outweigh the benefits.
- rhinorrhea, fever, and cough are symptoms of viral URI
- changes in mucous to yellow, thick, or green are the natural course of viral URI, NOT an indication for antibiotics.8
- treating viral URI will not shorten the course of illness or prevent bacterial infection.5
References
- Rosenstein N, Phillips WR, Gerber MA, Marcy SM, Schwartz B, Dowell SF. The common cold-principles of judicious use. Pediatrics 1998;101:181-184.
- Monto AS, Ullman BM. Acute respiratory illness in an American community. JAMA 1974;227:164-169.
- Gwaltney JM, Hendley JO, Simon G, Jordan WS. Rhinovirus infections in an industrial population. JAMA 1967;202:158-164.
- Todd JK, Todd N, Damato J, Todd WA. Bacteriology and treatment of purulent nasopharyngitis: a double blind, placebo-controlled evaluation. Pediatric Inf Dis J 1984;3:226-232.
- Gadomski AM. Potential interventions for preventing pneumonia among young children: lack of effect of antibiotic treatment for upper respiratory infections. Pediatric Infect Dis J 1993;12:115-120.
- Avorn J, Solomon D. Cultural and economic factors that (mis)shape antibiotic use: the nonpharmacologic basis of therapeutics. Ann of Intern Med 2000:133:128-135.
- O’Brien KL, Dowell SF, Schwartz B, et al. Acute sinusitis – prin-ciples of judicious use of antimicrobial agents. Pediatrics 1998;101:174-177.
- Wald ER. Purulent nasal discharge. Pediatric Infect Dis J 1991;10:329-333.
|