
Single-Family Dwelling Fire Claims the Life of a Volunteer Fire Fighter - Indiana
SUMMARY
On January 9, 1999, a male volunteer fire fighter (the victim) died of smoke inhalation while performing an interior attack on a fire at a single-family dwelling. A city police officer, who was first on-scene, entered the structure to try to extinguish the blaze with a portable fire extinguisher, and assisted the exit of family members from the structure. A volunteer engine company composed of a driver/operator and a fire fighter (the victim), were the first arriving company to the fire. When the engine company arrived, the driver/operator reported heavy smoke and fire showing from the northwest corner of the house. The Chief arrived within minutes of the first engine. The Chief then assisted the driver/operator in connecting the supply line to a fire hydrant approximately 150 feet away. At the same time, the victim and the police officer dragged the 1 3/4-inch hose from the engine to the front porch of the structure. The victim, wearing full turnout gear, donned an self-contained breathing apparatus (SCBA) and entered the structure to extinguish the fire. The Chief, returning from hooking up to the hydrant, noticed that the victim was not present and went around the exterior of the house to locate him. The Chief went to the hoseline that was inside the front door of the structure and pulled on it to get the victim’s attention. He did not feel any resistance on the line. The Chief then called "Man Down." At that same time, the Assistant Chief and three other fire fighters arrived in their privately owned vehicles (POVs). The Chief ordered a rescue attempt and the Assistant Chief, one fire fighter, and the driver/operator donned their SCBAs and entered the structure to search for the victim. They could only enter about 2 feet due to heavy smoke and extreme heat. Within minutes of the Assistant Chief entering the building, the water pressure dropped. Because of construction in the area, the water company previously reduced the flow of water on the main water line. The crew was forced to retreat because their SCBA low-air alarms began to sound. After the Assistant Chief and fire fighter’s changed their air bottles, the porch and part of the roof collapsed. The Chief then ordered an exterior attack with three charged lines. Approximately 2 hours after arrival, the fire was knocked down, and the attempts to locate the victim continued. The victim was found approximately 10 feet inside the structure. NIOSH investigators concluded that, to minimize similar incidents, fire departments should:
establish and implement an incident management system with written standard operating procedures for all fire fighters and ensure all fire fighters are trained on the system
ensure that command conducts an initial size-up of the incident before initiating fire fighting efforts and continually evaluates the risk versus gain during operation at an incident
ensure at least four fire fighters are on the scene before initiating interior fire fighting operations at a working structure fire
ensure that fire fighters wear and use PASS devices when involved in fire fighting, rescue, and other hazardous duties
ensure that fire fighters who enter hazardous areas, e.g., burning or suspected unsafe structures, be equipped with two-way communications with incident command
ensure automatic aid is established when known water pressure problems exist

House where fatality occurred.
INTRODUCTION
On January 9, 1999, a male 22-year-old volunteer fire fighter died of smoke inhalation while fighting a single-family dwelling fire. At approximately 0152 hours, the owner of a single-family dwelling called Central Dispatch to report a fire. The fire department was notified by Central Dispatch at 0154 hours. The first unit arrived at 0204 hours with one fire fighter and the victim. Within minutes, the victim entered the structure through the front door to attack the fire. Approximately 5 minutes later, the Chief realized the victim had entered the building alone and tried unsuccessfully to get his attention by pulling on the hoseline. He then ordered the Assistant Chief, one fire fighter and the driver/operator to begin rescue attempts. The heat intensified, and the porch and part of the roof collapsed. Rescue attempts were halted. The fire department then attempted to extinguish the fire with an exterior attack utilizing three charged hoselines. At approximately 0400 hours the fire was knocked down, and the victim’s body was located and removed.
On January 11, 1999, the U.S. Fire Administration notified NIOSH of the incident. On January 27, 1999, two NIOSH Safety and Occupational Health Specialists investigated this incident. Interviews were conducted with the Chief, the Assistant Chief and the fire fighters who responded to the incident. A site visit was conducted and pictures of the structure were taken. A copy of the death certificate, training records and layout of the structure were obtained.
The fire department involved in the incident serves a population of 1,200 in a geographic area of 52 square miles and is comprised of 16 fire fighters. The State requires each fire fighter to complete Fire Fighter Second Class training (equivalent to NFPA Level I) and the department requires 24 hours of annual refresher training. The victim had successfully completed Fire Fighter First Class training (equivalent to NFPA Level II). The victim had 13 months of fire fighting experience.
Although two volunteer fire companies were involved in this fire, only the one directly involved up to the time of the fatal incident are discussed in this report.
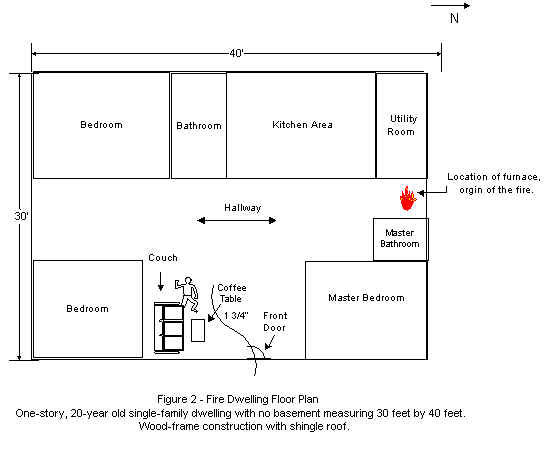
The site of the incident was a 20-year-old, one-story, ranch-style home with no basement, of approximately 1,100 square feet (see Figure 1). It was constructed of wood with a pitched, shingled roof.
INVESTIGATION RESULTS
On January 9, 1999, at 0152 hours, the resident of a single-family dwelling called Central Dispatch (Sheriff’s Office) to report a fire. The fire had been burning approximately 10 minutes prior to the call. The fire department was notified at 0154 hours. At 0204 hours, Engine 12-2 arrived with two fire fighters, including the victim. Engine 12-3, Tanker 12-4A, Tanker 12-4B and Rescue 12-5 arrived between 0210 and 0225 hours, each with one fire fighter. The Chief, Assistant Chief and two additional fire fighters arrived by POVs. Altogether, five pieces of apparatus and 10 personnel arrived at the fire scene between 0204 and 0225 hours.
A city police officer, who was the first on-scene, went inside the structure and tried to extinguish the fire with a portable fire extinguisher. When he applied the extinguisher agent, the flames rolled over him and the fire began to intensify. He then helped the family members escape from the home through the front door, leaving the door open. Engine 12-2 was the first to arrive on-scene at 0204 hours, with one fire fighter (the victim) and the driver/operator. The driver/operator of Engine 12-2 noticed the police officer and the family exiting through the front door when they arrived. The Chief, arriving in his POV at approximately 0206 hours, assumed command and reported heavy smoke and flames coming from the northwest corner of the house. The Chief assisted the driver/operator of Engine 12-2 in connecting the 5-inch supply line to the hydrant. During the same time, the victim and the police officer pulled a 1 3/4-inch crosslay hose from the engine and laid it at the front door of the structure. The victim, in full turnout gear, donned his SCBA and advanced the hoseline inside the structure through the front door. At approximately 0209 hours, the Chief, returning from hooking up the supply hose, noticed the victim was not present and the hoseline was inside the structure. He traveled around the exterior of the structure yelling into the windows for the victim to exit. Since he received no response, the Chief then tried to get the victim’s attention by pulling on the hoseline. The Chief did not feel any resistance on the line and immediately called "Man Down" to the personnel on-scene. At the same time, the Assistant Chief and two fire fighters arrived on-scene by POV. The Chief ordered the Assistant Chief and two fire fighters to don their SCBAs and perform a search to try and locate the victim. At approximately 0215 hours, the Chief called for back-up from a neighboring volunteer fire department. The Assistant Chief and two fire fighters retrieved an additional 150-foot, 1 3/4-inch crosslay from Engine 12-2 and attempted to enter the structure. The Assistant Chief (nozzle man) entered the structure approximately 2 feet but could not proceed any further due to extreme heat and thick smoke. He applied water overhead to cool the ceiling area; however, the water pressure dropped due to problems with the hydrant. (The water company had previously reduced the flow of water on the main water line due to construction in the area.) Additionally, SCBA low-air alarms began to sound, forcing the crew to retreat. After changing air bottles, the Assistant Chief and two fire fighters applied water to the exterior of the front porch. Within 1 minute, the porch and part of the roof collapsed. The Chief then ordered an exterior attack. At the same time, the back-up crew, consisting of six fire fighters, arrived in POVs. They retrieved an additional 150-foot, 1 3/4-inch crosslay from Engine 12-2 and began applying water to the fire. Additionally, another fire fighter hooked up a 2 ½-inch hoseline to Tanker 12-2. All water supply was transferred by the tankers due to the hydrant’s reduced flow of water. Tanker 12-3 was used to shuttle water between the fire scene and the nearest adequate hydrant, approximately 1/4 mile away. Fire extinguishment continued until approximately 0400 hours. When the conditions improved enough to allow entry into the structure, the victim was found approximately 10 feet inside the front door. The victim was found with his SCBA mask off and the mask partially melted. His turnout gear was destroyed and his helmet was missing. His legs were partially under a couch and a coffee table which were located in the living room (see Figure 2). Additionally, the Chief stated that the conditions for a flashover existed, i.e., simultaneous ignition of all combustibles in the room and high heat level from the floor to the ceiling. A post-incident investigation revealed the point of origin of the fire was in the furnace area.
CAUSE OF DEATH
According to the death certificate, the cause of death was asphyxiation due to smoke inhalation and carbon monoxide.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Fire departments should implement an incident command system (ICS) with written standard operating procedures for all fire fighters and ensure all fire fighters are trained on the system. 1-3
Discussion: The ICS should establish roles and responsibilities for all personnel involved, should ensure personnel accountability and safety, and should provide a well-coordinated approach to all emergency activities. All fire department personnel should be thoroughly trained on this system, and they should receive periodic refresher training. All training should be documented. While this department practices the two-in/two-out system, this was the first structure fire the victim had fought, and he entered the structure alone without the Chief’s knowledge. Under the ICS, the victim would have awaited additional personnel to man the attack hose and orders from the Chief prior to entry.
Recommendation #2: Fire departments should ensure that command conducts an initial size-up of the incident before initiating fire fighting efforts and continually evaluates the risk versus gain during operation at an incident. 4-6
Discussion: One of the most important size-up duties of the first-in officers is locating the fire and determining its severity. This information lays the foundation for the entire operation. First, it determines the number of fire fighters and the amount of apparatus and equipment needed to control the blaze. Second, it assists in determining the most effective point of fire attack and the most effective method of venting heat and smoke. The size-up should also include risk versus gain during incident operations. Due to lack of manpower when the Chief and first engine arrived, no initial size-up was conducted.
Recommendation #3: Fire departments should ensure at least four fire fighters are on the scene before initiating interior fire fighting operations at a working structure fire. 4, 7
Discussion: During interior structural fire fighting (an Immediately Dangerous to Life or Health [IDLH] atmosphere) operations, a SCBA is required, and at least two fire fighters must enter and maintain visual or voice contact with each other at all times. In addition, two fire fighters must be on standby while interior operations are going on. The two exterior fire fighters should form a rescue team that is stationed outside the hazardous area. The rescue team should be trained and equipped to begin a rescue immediately if needed. A dedicated rapid intervention team may be required if more than two fire fighters are in the hazardous area. Again, the victim entered the structure alone. By the time the Chief became aware of this and tried to alert the victim, conditions had deteriorated to the point that the hastily assembled rescue team could not gain entry to rescue the victim.
Recommendation #4: Fire departments should ensure that fire fighters wear and use Personal Alert Safety System (PASS) devices when involved in fire fighting, rescue, and other hazardous duties. 2, 4
Discussion: The PASS is a small electronic device worn by the fire fighter which will emit a distinctive audible alarm if the fire fighter becomes motionless for 30 seconds, or it can be activated manually if needed. This device is designed to assist rescuers in locating the fire fighter. All fire fighters who enter hazardous areas should be provided with and use a PASS device. Although the fire department provided two PASS devices on each apparatus, the victim was not wearing a PASS device.
Recommendation #5: Fire departments should ensure that fire fighters who enter hazardous areas, e.g., burning or suspected unsafe structures, be equipped with two-way communications with incident command. 2, 6
Discussion: Although face-to-face is the best form of communication, radio communication should be used when face-to-face communication is not possible. Radios are essential for efficient fireground operations and keep units in communication with one another. They provide progress and are necessary to request assistance. When the victim entered the building, he was not equipped with a two-way radio. If the victim had been equipped with a portable radio, the Chief may had been able to determine sooner that the fire fighter had experienced a problem and needed immediate assistance.
Recommendation #6: Fire departments should ensure automatic aid is established when known water pressure problems exist. 8
When water supply problems are known, the fire department should plan for availability of additional water sources and establish automatic aid (i.e., a plan developed between two or more fire departments for immediate joint response on first alarms). Preplanned availability will provide additional equipment to be dispatched on the first alarm. Although the Chief was notified days prior to this fire about the water pressure being turned down due to area construction, no other means of water was available at the first alarm of this fire.
REFERENCES
1. 29 Code of Federal Regulations 1910.120(q)(3), Hazardous Waste Operations and Emergency
Response.
2. International Fire Service Training Association [1998]. Essentials of fire fighting, 3rd ed. Stillwater, OK: Oklahoma State University, Fire Protection Publications.
3. National Fire Protection Association. NFPA 1561: Standard on fire department incident management system. 1995 ed. Quincy, MA: National Fire Protection Association.
4. National Fire Protection Association. NFPA 1500: Standard on fire department occupational safety and health program 1997 ed. Quincy, MA: National Fire Protection Association.
5. Kipp JD, Loflin ME [1996]. Emergency incident risk management: A safety and health perspective. New York, NY: Van Nostrand Reinhold Publishing.
6. Brunacini A. [1985] Fire Command, Quincy, MA: National Fire Protection Association
7. 29 Code of Federal Regulations 1910.134(g)(4) Respiratory Protection.
8. National Fire Protection Association. NFPA 1231: Standard on water supplies for suburban and rural fire fighting. 1993 ed. Quincy, MA: National Fire Protection Association.
INVESTIGATOR INFORMATION
Kimberly Cortez, Safety and Occupational Health Specialist, NIOSH, Surveillance and Field Investigations Branch, Division of Safety Research and Tommy N. Baldwin, Safety and Occupational Health Specialist, Hazard Evaluations and Technical Assistance Branch, Division of Surveillance, Hazard Evaluations, and Field Studies.
Figure 1. House where fatality occurred.

Return to Fire Fighter Homepage
![]()
This page was last updated on 11/21/05