
Emergency Medical Technician Receives Serious Burns from an Oxygen Regulator Flash Fire-South Carolina
SUMMARY
On August 27, 1998, a female Emergency Medical Technician (EMT) was severely burned while performing a routine truck (ambulance) changeover. The changeover required the EMT (victim) to check all equipment, supplies, oxygen cylinders, and make any changes needed. The EMT had just started her evening shift and began to complete the changeover. She removed the Oxy-Caddy (bag which housed the oxygen resuscitator) from its storage compartment. She opened the top of the Oxy-Caddy to gain access to the regulator, placed it in a vertical position, and made three attempts to open the post valve to charge the regulator. Experiencing difficulties (valve was tightly closed), she placed her foot on the step of the patient compartment door and placed the cylinder against her leg and on the step to gain extra leverage to open the post valve. On the fourth attempt the regulator charged and immediately flashed, emitting a white ball of fire from the regulator. The victim pushed the regulator and cylinder inside the patient compartment as her clothes caught fire from the waist down. She then ran into the station’s bay where she was met by the Corporal of the Emergency Medical Service (EMS) station who came out of the office when he heard a loud pop and the victim screaming. The EMTs inside the office immediately initiated patient care by dousing the victim with water as the Corporal called the fire department and an ambulance. The Corporal then exited the office to retrieve supplies from the truck only to witness the truck was fully engulfed in flames. Approximately 4 minutes later the fire department and ambulance arrived on scene. The truck fire was extinguished by the fire department as the victim was loaded into the ambulance and transported to a local hospital with burns to approximately 25 percent of her upper and lower extremities.
NIOSH investigators concluded that, to reduce the risk of similar incidents, fire departments should:
consider the use of oxygen regulators constructed of materials having an oxygen compatibility equivalent to brass
ensure that the cylinder is placed in an upright position, the cylinder post valve is pointed in a safe direction (away from the operator), and opened then closed before the regulator is attached to the cylinder
ensure that when opening a cylinder post valve with the regulator attached, it should be opened slowly and positioned away from the operator
ensure that fire fighters are trained and aware of safe handling procedures pertaining to oxygen systems
ensure that any components added to the regulator, such as gauge guards, are installed so that they do not block the regulator vent holes
ensure that oxygen systems (cylinders and regulators) are stored in a cool area free of dirt, oils, and grease
ensure that oxygen refilling stations and maintenance areas where oxygen equipment is serviced, are in a locked, air-conditioned room that is clean and free of dirt, oils, and grease
Additionally, to reduce the risk of similar incidents, manufacturers should:
ensure that they provide a warning pertaining not to occlude the vent ports on the regulator.

Incident Scene
INTRODUCTION
On August 27, 1998, a 24-year-old female EMT was severely burned while performing a routine truck changeover. The victim removed the Oxy-Caddy from its storage compartment and began to check the oxygen cylinder’s pressure. As the victim opened the post valve to charge the regulator, it immediately flashed, causing serious burns to the victim’s upper and lower extremities.
On September 9, 1998, a Safety and Occupational Health Specialist and a physician from NIOSH investigated this incident. Meetings were conducted with the victim, EMTs present at the incident, the director of the EMS, and staff involved with the EMS equipment and operations. The truck and oxygen resuscitator were photographed and individual reports from the station’s investigation were obtained. The ambulance involved in the incident was inspected during the site visit.
The EMS operation involved in this incident serves a population of 350,000 in a geographical area of 789 square miles. The EMS operation has approximately 150 employees: 120 full-time and 24 part-time employees. They use 12 trucks (ambulances) and 3 rescue stations in response to approximately 35,000 calls a year. All EMTs are State certified and are provided the following training: orientation, system operation, bloodborne pathogens, hazmat response, and hazmat equipment. Additionally, as a part of the State certification, each EMT is required to set up an oxygen resuscitator. Refresher training is provided each month which includes 4 hours of medical service training and 8 hours of specialized rescue training. The victim had 1 ½ years’ experience as an EMT.
INVESTIGATION
On August 27, 1998, at 1840 hours, an Emergency Medical Service truck (ambulance) had just returned to the station to complete a shift changeover. The shift change requires all EMTs starting the new shift to complete a truck changeover. The changeover requires the EMTs to check all equipment, supplies, oxygen cylinders, and make any changes needed. The victim had just arrived to start her evening shift (assigned to this station as a fill-in) when the truck had returned from a call. The victim began to complete the truck changeover as the other EMTs went inside the office of the EMS station. The victim removed the Oxy-Caddy from the airway storage compartment, located in the patient compartment, and removed the cylinder from its horizontal position (see Photo 1). Placing it in a vertical position on the step of the patient compartment door (see Photo 2), the victim attempted to open the post valve to charge the regulator. The victim made three unsuccessful attempts to open the post valve. She stated that the valve had been tightly closed, so she placed her foot on the step of the patient compartment door and placed the cylinder under her leg and on the step to provide additional leverage. She then made a fourth attempt to open the post valve and succeeded. The victim stated that she heard a loud popping sound and then the regulator flashed, emitting a white ball of fire. The victim’s polyester clothing caught fire from the waist down. She pushed the cylinder into the patient compartment and ran into the station bay. A Corporal in the station heard the loud pop and the victim screaming. He opened the door to the station’s office to find the victim running toward him on fire from the waist down. The Corporal helped the victim through the door where she dropped to the ground. The Corporal and EMTs inside the office immediately initiated patient care by dousing the victim with water. The Corporal then called the fire department and an ambulance. One of the EMTs cut off the victim’s clothes and requested someone go to the truck and get supplies to treat the victim. The Corporal exited the office to retrieve supplies from the truck (approximately 10 feet from the bay) only to find it fully engulfed in flames.
They continued pouring water on the victim’s burns as they waited for the ambulance to arrive. Approximately 4 minutes after the call, the fire department and ambulance arrived on scene. The fire department extinguished the flames in the truck as the ambulance EMTs provided assistance to the victim. One of the EMTs called the local hospital to receive orders for morphine to treat the victim. The order was received and an IV line was started. She was also placed on an oxygen re-breather @ 15 liters per minute. The Corporal then gave the victim additional morphine as the EMTs wrapped her in burn blankets and loaded her onto the stretcher. She was then transported to the local hospital with burns to approximately 25 percent of her upper and lower extremities. The truck involved in the incident was declared a total loss and the estimated value was $175,000 (see Photo 2).
NOTE: The EMTs who had just finished their shift stated that the cylinder involved in the incident was changed the night before the incident occurred; however, it was not used during that shift. The EMTs also stated that they had charged the regulator before the start of their shift to check the cylinder’s pressure and it appeared to be working properly.
CYLINDER / REGULATOR INFORMATION
The cylinder involved in the incident was an "E"-size aluminum-bodied cylinder. The cylinder was last checked at 1,800 pounds per square inch (psi) at the beginning of the previous shift and was not used after the check. The cylinders were refilled and inspected by a local contractor. The cylinder involved in the incident was ruptured in two areas and showed some deformation near the neck (see Photo 3). It was standard procedure by the EMS to remove the cylinders from service whenever the pressure dropped below 500 psi. The cylinder involved in this incident was stamped with a 1997 inspection date and had previously proved to be in good working condition. All secondary cylinders were stored in a separate, clean, locked room at the EMS station. The cylinders were stored in a vertical position with dust covers over the post valve opening.
The type of regulator involved in this incident has been involved in several other incidents in the past.14 The manufacturer of the regulator had issued a recall notice prior to this incident stating the stainless steel screen located under the inlet nozzle (see Photo 4) should be replaced with a sintered-bronze inlet filter. The manufacturer would send the sintered-bronze inlet filter upon request. However, the EMS operation could not recall or show any record of having received this recall notice. The regulator involved was a full-bodied aluminum regulator with aluminum exposed to high-pressure oxygen. Additionally, laboratory testing has shown that the sintered-bronze filter was not completely effective in preventing fire flashes.15
The regulator involved in the incident had a gauge guard placed on it to protect the pressure gauge from damage. The gauge guard (see Photo 5) was positioned on the regulator in a manner that blocked the relief vent holes (see Photo 6). Laboratory testing has shown that in past regulator fires the vent holes were usually the first exit of fire. In this incident the gauge guard blocked the vent holes, not letting the fire vent properly, causing the fire to burn back into the cylinder (blowback) and the cylinder to rupture (see Photo 3) which increased the severity of this incident.
During the fire, the regulator broke off the cylinder and was found in several pieces (see Photo 7). The regulator and cylinder were sent by the EMS involved in this incident to an independent forensic testing laboratory to be evaluated. The results of that evaluation are summarized in the next section.
TEST RESULTS
The test results presented here are based on the investigation completed by Barry Newton (Wendell Hull & Associates, Inc.) and the inspection of the fire-damaged equipment. The following conclusions are from the report prepared by Mr. Newton.2
1) The origin of fire could not be isolated with certainty due to extreme consumption of the regulator’s component parts. However, the melt-flow patterns and propagation paths were consistent with an origin either at the cylinder’s valve seat or in the high-pressure section of the regulator. Due to the presence of the gauge protector, the propagation patterns and blowback condition (burning in a backwards direction into the cylinder) would have been expected for initial ignition at either location. Due to the extreme flammability of aluminum under the service conditions, the combustion event would be strongly dominated by aluminum ignition in the regulator in the very early stages of the fire. Experience indicates that cylinder valve seat ignition due to frictional interaction with the metallic nozzle or particle impact ignition against the regulator’s stainless steel screen are the most likely ignition mechanisms. Experience also indicates that multiple ignition mechanisms are active in normal oxygen systems and that several of these have been associated with regulator fires with promoted ignition of the aluminum body. The design of the regulator in this incident is not sufficient to shield the ignition of the aluminum body for the foreseeable service conditions. In the investigator’s opinion the regulator design, in its application and exposure of aluminum to normally active ignition mechanisms, is hazardous and represents a highly defective design condition.
2) The fire patterns were consistent with early stage kindling and propagation from the inlet filter downstream and then against the normal flow (i.e., "blowback") due to the inability of the regulator to vent through the normal vent ports. Propagation against the normal flow, which experience indicates is rare, was felt to be due to the containment produced by the gauge guard encapsulating the external body of the regulator. This guard essentially blocked the vent ports for the regulator and therefore prevented the venting of the fire in the early stages of the event. The momentary containment of the event within the regulator is consistent with development of very high combustion over pressures, which would be expected to result in propagation and pressure buildup in a direction toward the oxygen cylinder. The blowback and unidirectional flow patterns indicated by the evidence are consistent with this condition. In the investigator’s opinion, the gauge protector rendered this fire more severe and should not be utilized if occlusions of the vent ports are produced. Further, the regulator manufacturer should have maintained the warning pertaining to occluding the vent ports as was provided on other regulators in the past.
3) Propagation from the regulator to the cylinder follows a reasonable progression considering the containment developed with the gauge guard and the blowback condition. Propagation from the cylinder to the regulator does not follow a reasonable progression due to the lack of normally active ignition mechanisms within the cylinder. Ignition within the cylinder valve leading to ignition of the regulator is also possible as long as the blowback condition is present. In the investigator’s opinion, had the gauge protector not been present, the fire would have progressed in a manner similar to the previous regulator fires investigated and probably would not have promoted the oxygen pressure cylinder.
4) This regulator fire is unique when compared to the previous regulator fires due to extreme severity probably resulting from the presence of the gauge protector. It is, however, indicative of the extreme conditions that are plausible with aluminum combustion under high-pressure oxygen conditions. In the investigator’s opinion, exposure of aluminum without sufficient shielding from the normally active ignition mechanisms is unreasonable in a design of this nature. Furthermore, due to the extreme flammability of aluminum, in the investigator’s opinion, this fire represents a new category of oxygen regulator fires that has not been observed previously.
INJURY RESULTS
The victim received first-, second-, and third-degree burns to over 25 percent of her upper and lower extremities.
RECOMMENDATIONS AND DISCUSSION
Recommendation #1: Fire departments should consider the use of oxygen regulators constructed of materials having an oxygen compatibility equivalent to brass.2-7, 14
Discussion: Aluminum alloys are attractive candidate materials for pressure vessels because of their high strength-to-weight ratios. High pressure oxygen system components for portable or flight use must be lightweight, so it may appear to be desirable to build their housings from such lightweight metals as aluminum. However, the use of aluminum alloys in lines, valves, and other components should be avoided whenever possible because they easily ignite in high-pressure oxygen, burn rapidly, and have very high heats of combustion. Aluminum is ignited exceptionally easily by friction because the wear destroys its protective oxide layer; it should not be used in systems where frictional heating is possible.6
Aluminum is easily ignited by particle impact, and aluminum particulate is a far more effective ignition source than many other metal particulate tested to date (titanium particulate has not been tested). High-pressure oxygen systems fabricated from aluminum must be designed with extreme care to eliminate particulate. Testing has shown that aluminum is substantially more flammable in oxygen than brass or other high copper or high nickel alloys.7
Sources indicate that commonly used aluminum alloys can easily burn in the presence of high-pressure pure oxygen once an ignition is present. Thus, aluminum will burn in pure oxygen at a pressure of 35 psi (this is about twice the normal atmospheric pressure) whereas some brass alloys require over 5000 psi of pure oxygen to burn. Aluminum will also produce approximately 10 times the amount of heat of copper alloys when burning.
One concern of using aluminum in the downstream flow path is the possibility of particle impact and the aluminum not being able to contain the ignition. Particles can be introduced into oxygen resuscitators in many different ways. Experts suggest the presence of a particle or particles in the cylinders is not as problematic as the design of the oxygen flow path and the materials used.
The cylinder has a post valve that closes off the oxygen opening and allows the regulator to be attached. When the post valve is screwed into the aluminum cylinder, there is a possibility that the two metals rubbing together could create metal particles that would remain enclosed in the cylinder body. Galling is a condition involving smearing and transfer of material from one surface to the other and particles could be introduced by metal-to-metal rubbing seals which occurs when the post valve is opened and closed. The frictional heat of the galling could lead to ignition of the valve; or the particles generated by the galling could cause malfunction or ignition of another component downstream. Therefore, the design of the regulator’s downstream flow path should be forgiving of the particles if ignition should occur. Experts suggest the downstream flow path should be lined with brass, bronze, or a similar material which would resist particle ignition, and that using such a material would shield the particle ignition and provide the opportunity to burn out.
Recommendation #2: Fire departments should ensure that the cylinder is placed in an upright position, the cylinder post valve is pointed in a safe direction, and opened then closed before the regulator is attached to the cylinder.8
Discussion: After removing the valve protection cap, the cylinder post valve should be opened slowly for an instant to clear the opening of particles of dust or dirt, being careful to point the valve opening away from personnel and in a safe direction.
Cylinders are generally stored on the fire trucks in a horizontal position, which could allow particles to rest near the neck of the cylinder. Whenever possible, cylinders should be placed in an upright position not only when in storage, but also when in use. If cylinders are stored in an upright manner, any particulate in the cylinder would generally settle in the bottom of the cylinder and not as easily entrain in the oxygen flow discharge.
In this incident, the cylinder was lying in a horizontal position when the victim opened the airway bag. When she placed the cylinder in a vertical position and opened the post valve, the cylinder flashed. Particle impact is a possible ignition source in this incident; however, the majority of the regulator was consumed in the fire and a definite source of ignition could not be determined.
Recommendation #3: Fire departments should ensure that when opening a cylinder post valve with the regulator attached, it should be opened slowly and positioned away from the operator.5, 8, 9
Discussion: The Compressed Gas Association Manual, CGA G-4, Section 4.4.10,8 recommends the following: Never to permit oxygen to enter the regulator suddenly. Always open the cylinder valve slowly. Stand to one side and not in front of or behind the regulator when opening the cylinder valve. Never use wrenches or tools except those provided or approved by the oxygen regulator manufacturer. Avoid the use of a wrench on valves equipped with hand wheels. Never hammer a valve handwheel in attempting to open or to close the valve. If a valve cannot be opened by hand, notify the supplier.
The fast opening of the valve could subject passageways or components to adiabatic compression (rapid compression with an associated rise in gas temperature, potentially to a material’s ignition point), which could result in hot spots and possible ignition of nonmetallic or particulate contaminates. Fast opening of the valve also provides the possibility of particles being forced into the downstream flow path. Once the particles are introduced into the downstream flow, it is also possible that the particles can collide with the filter located underneath the inlet screw or an additional target (see Photo 4). The filter will then act as the target which results in the ignition of the metal particle.
The regulator should be positioned away from the operator when the cylinder valve is opened and to let the regulator pressurize before looking at the gauge. The cylinder should be positioned upright and placed between the operator and the regulator (regulator barrel pointed away from the operator). This way an operator can open the cylinder valve from at arm’s length away from the operator. Operators typically look at the gauge when the cylinder valve is opened. It is recommended that operators not try to read the gauge until the regulator has fully pressurized and they have waited until the pressurization transients settle out.
In this incident it is unclear if the victim opened the valve slowly. The victim stated that the valve was tightly closed and she had to use excessive force to open it, which could possibly cause the sudden inrush of oxygen. Once ignition took place, the aluminum inside the regulator ignited, released outward, and also burnt backwards into the cylinder (due to the gauge guard blocking the vent holes), causing serious injury to the victim. Laboratory tests have concluded that aluminum alloys will readily sustain combustion at pressures as low as 35 pounds per square inch ambient (psia) and produce approximately 10 times the heat of copper alloys when burning.
Recommendation #4: Fire departments should ensure that fire fighters are trained and aware of safe handling procedures pertaining to oxygen systems.8, 10
Discussion: Fire departments should provide fire fighters with adequate techniques for safe handling of oxygen resuscitators. The training should include areas such as handling oxygen resuscitators, operating procedures, maintenance, cleaning, visual inspections, and hazards that can occur. The operation of oxygen resuscitators is not a complicated task; therefore, training is sometimes overlooked. The operators should not only be able to operate oxygen resuscitators, but also know how to care for them and be aware of hazards involved with their use. Fire fighters are sometimes put in complicated situations where they have to administer oxygen to patients in the vicinity of grease, oil, gas, or other dangerous substances. Fire fighters should be trained to know what to do in these situations and understand the proper maintenance procedures as well as when to report that a system needs repair.
Additionally, operators should be instructed to first open the cylinder valve slowly, letting the regulator pressurize, and then fully open the cylinder valve. What often happens is that the operator opens the valve just slightly, sees the gauge register pressure, and then doesn’t fully open the cylinder valve. Fully opening the cylinder valve has two positive effects: (1) When the valve is not fully opened it can cause deformation of the cylinder seat valve, and this has been suspected to be an ignition source; 2) Opening the cylinder valve against the stem gasket (i.e., fully opening and back seating the valve) helps keep oxygen from leaking past the stem gasket during use.7
Operators should also use care when installing the inlet gasket. Installation of this gasket is a good way of contaminating the regulator/cylinder valve if the operators hands or components are not clean. Care should also be used to tighten the regulator onto the cylinder valve rigidly to prevent leakage of oxygen past the seal during use.7
To further assist in the understanding of these areas, fire departments can refer to, and follow, the Compressed Gas Association’s CGA G-48 manual and additionally ASTM’s documents regarding training.10
Recommendation #5: Fire departments should ensure that any components added to the regulator, such as gauge guards, are installed so that they do not block the regulator vent holes.7
Discussion: Gauge guards can be installed on regulators to protect the gauge from being damaged. However, if any additional components (such as a gauge guard) are installed on the regulator, they should be supplied by the manufacturer and installed so as not to block the regulator vent holes. Covering of the vent holes could restrict the vents from functioning properly and possibly cause a blowback condition if a fire would occur.
NOTE: The following two recommendations do not apply to this investigation. However, these recommendations are included to remind users of the proper storage for oxygen cylinders.
Recommendation #6: Fire departments should ensure that oxygen systems (cylinders and regulators) are stored in a cool area free of dirt, oils, and grease.4, 8-13
Discussion: Fire departments should ensure that oxygen cylinders are stored in a specific location. Oxygen cylinders should be kept free of flammable material, especially oil, grease, or any other readily combustible substance. Oxygen cylinders should also not be placed where oil can drip on the cylinder, its valve, or other attachments. It is possible that these substances could be introduced into the cylinder if they are present. If a cylinder comes in contact with a flammable substance or has been around a flammable substance where a possible contaminant could be introduced into the cylinder, the cylinder should be removed from service and the supplier contacted.
Cylinders should remain in a cool area while not in use. Cylinders should not be stored above 125EF (51.7EC) or used above 120EF (48.9EC). Cylinders should never be allowed to reach temperatures exceeding 125EF (51.7EC) , because of the rise in pressure in the cylinder with increasing temperature. Therefore, cylinders should never be placed near furnaces, radiators, or any other source of heat.
Cylinders should also be stored with plastic caps over the post valve openings to reduce the possibility of contaminate buildup around the valves’ openings. The plastic caps should be placed on the cylinder’s post valves as soon as the cylinders are refilled. The cylinders should also be stored in a secured vertical position.
Recommendation #7: Fire departments should ensure that oxygen refilling stations and maintenance areas where oxygen equipment is serviced, are in a locked air-conditioned room that is clean, and free of dirt, oils, and grease.1, 8, 9
Discussion: Some fire departments refill their own cylinders, while other fire departments contract out the process. Departments that refill their cylinders should have an area for the refilling system that can be locked when not in use. This will reduce the risk of tools used for the process being removed, contaminated, and reintroduced to this environment. This area should be kept clean and free of oils, grease or any other combustible substance. During the refilling process, the post valve opening is generally left uncovered until the tank is refilled, leaving the valve available to collect contaminants. Keeping the area separate, locked, and clean should reduce the possibility of contaminants entering the area.
The refilling process should be completed by an individual who has been properly trained. The individual should have clean hands free of any contaminants, and if using gloves, should use a clean pair that are used only for this process. All tools and materials used in this process should be routinely cleaned and used only for this process. The area of the refilling station should be air-conditioned to maintain adequate temperatures.
Maintenance areas should be kept clean, especially when gauges are being replaced. After the gauge is removed the gauge port should be inspected for signs of contamination, and the gauge should be inspected for contamination (oil coming from gauge port) etc.
Recommendation #8: Manufacturer’s should ensure that they provide a warning pertaining not to occlude the vent ports on the regulator.2
Discussion: Manufacturer’s should provide a warning not to occlude the vent ports on oxygen regulators. If a fire would occur in a regulator, the vent ports would be a relief opening for the fire to properly vent. Blocking the ports could increase the combustion intensity and overpressure causing the fire to propagate towards the cylinder. In this incident, the vent ports were blocked by a gauge guard which protected the pressure gauge. When the fire occurred, the gauge guard blocked the fire vent path, causing a blowback condition. The fire then began burning into the cylinder, causing the cylinder to rupture. The fire became more intense and consumed most of the interior of the ambulance (truck) involved. The Emergency Medical Service stated that they received no warning which pertained to occluding the vent ports on the oxygen regulators.
Oxygen resuscitators are medical devices which come under the jurisdiction of the Food and Drug Administration (FDA). NIOSH has been working with the FDA on the potential hazards with aluminum-bodied regulators which have been identified through the NIOSH investigations. In February 1999, the FDA issued a Public Health Advisory jointly with NIOSH entitled Explosions and Fires in Aluminum Oxygen Regulators. A copy of this advisory is available on the FDA homepage at www.fda.gov/cdrh/safety.html.
REFERENCES
1. Title 49, Code of Federal Regulations (CFR) Part 173.34 (e), Qualification, maintenance, and use of cylinders. U.S. Department of Transportation (DOT).
2. Newton, BE. Report to State of South Carolina County Emergency Medical Service concerning oxygen resuscitator fire. Wendell Hull & Associates, Inc., Las Cruces, NM, March 10, 1999.
3. Canadian Standards Association [1987]. Pressure regulators, gauges, and flow-metering devices for medical gases. Ontario, Canada, CAN CSA-Z305.3-M87.
4. ASTM [1997]. Standards related to flammability and sensitivity of materials in oxygen-enriched atmospheres. West Conshohocken, PA, ASTM PCN 03-704097-31.
5. National Aeronautics and Space Administration [1983]. Design guide for high pressure oxygen systems, Washington, DC, Publication 1113.
6. National Aeronautics and Space Administration [1996]. Safety standard for oxygen and oxygen systems. Washington, DC, Publication NSS 1740.15.
7. Newton, BE., Personal communication review of NIOSH FACE report 98-F23, January 13,1999.
8. Compressed Gas Association [1996]. 4.0 High pressure oxygen cylinders. Oxygen CGA G-4. 9th ed. Compressed Gas Association, Inc., 1725 Jefferson Davis Highway, Arlington, VA 22202.
9. National Fire Protection Association [1994]. NFPA 53: Guide on fire hazards in oxygen- enriched atmospheres. Quincy, MA.
10. Werley BL, ed. [1991]. ASTM Committee G4.05 fire hazards in oxygen systems: ASTM standards technology training course book. 2nd ed. Philadelphia, PA.
11. Compressed Gas Association, Inc. CGA P-1, Safe handling of compressed gases in containers. Compressed Gas Association, Inc., 1725 Jefferson Davis Highway, Arlington,VA 22202.
12. National Fire Protection Association [1990]. NFPA 50: Standard for bulk oxygen systems at consumer sites. National Fire Protection Association, Batterymarch Park, Quincy, MA.
13. National Fire Protection Association [1993]. NFPA 99:Standard for health care facilities. National Fire Protection Association, Batterymarch Park, Quincy, MA.
14. FDA, NIOSH [1999]. FDA and NIOSH public health advisory: explosions and fires in aluminum oxygen regulators. Washington, DC: U.S. Department of Health and Human Services, Food and Drug Administration.
15. NIOSH [1999]. Injury in the line of duty: Oxygen regulator flash severely burns one fire fighter - Florida. Morgantown, WV: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, Division of Safety Research, DHHS (NIOSH) Publication 98F-23.
INVESTIGATOR INFORMATION
Frank C. Washenitz II, Safety and Occupational Health Specialist, Surveillance and Field Investigations, Division of Safety Research and Tom Hodous, M.D., Office of the Director, Division of Safety Research.
EXPERT INPUT AND TECHNICAL REVIEW
Barry E. Newton, BSME, PE, Wendell Hull & Associates, Inc.

Photo 1: This photo depicts the Oxy-Caddy which is used to house the oxygen resuscitator when not in use. (Not actual Oxy-Caddy involved)
Photo 2: This photo depicts the ambulance (truck) involved in the incident.
Photo by: Wendell Hull and Associates, Inc.
Photo 3: These photos depict various views of the external wall of the fire-damaged oxygen cylinder. The cylinder was bulged from heat and internal pressure near the neck and had split, as shown, in an axial direction.
Photo by: Wendell Hull and Associates, Inc.
Photo 4: This photo is an internal section view of a similar regulator involved in this incident. This view depicts the position of the stainless steel screen.
Photo by: Wendell Hull and Associates, Inc.
Photo 5: This photo depicts a similar regulator with a gauge guard blocking the vent ports.
Photo by: Wendell Hull and Associates, Inc.
Photo 6: This photo depicts the vent ports located in the low pressure section of the regulator. In previous regulator fires, the fire usually exited the regulator through the vent ports.
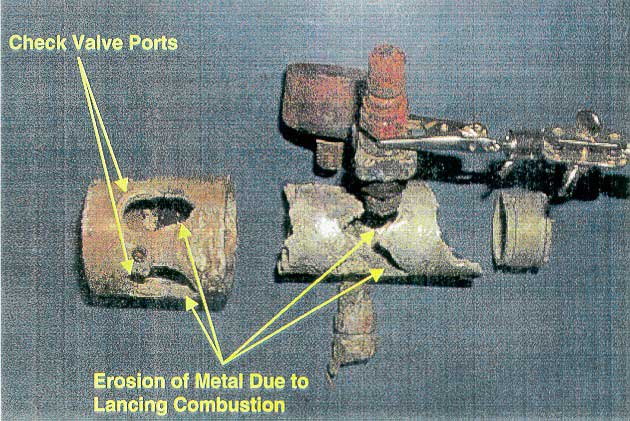
Photo by: Wendell Hull and Associates, Inc.
Photo 7: This photo depicts the remains of the regulator involved in the incident. The regulator was completely detached from the cylinder and discovered in several pieces as a result of the flash.

Return to Fire Fighter Homepage
![]()
This page was last updated on 11/21/05