
Revised: October 19, 2007
Revised: October 19, 2007
On June 25, 2006, a 34-year-old male volunteer Deputy Fire Chief (the victim) died after falling through a failed section of floor on the first floor of a residential structure fire while attacking the fire from above. Attempts were made to reach the victim via a 14’ roof ladder, but due to debris in the basement, fire/smoke conditions, and the angle of the failed floor, all attempts to reach the victim via the ladder failed. Fire fighters entered the house, traversed the floor, and gained interior access to the basement to retrieve the victim. The victim was immediately found but was unresponsive. The crews had difficulty in moving him up the basement stairs, but after approximately 20 minutes they were able to remove, provide medical treatment, and transport him via ambulance to the hospital where he was pronounced dead.
 |
NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should:
On June 25, 2006, a 34-year-old male volunteer Deputy Fire Chief (the victim) died after falling through a failed section of floor in a one-story residential structure on fire. On June 26, 2006, the U.S. Fire Administration (USFA) notified the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR), of the fatality. On September 18–20, 2006, the DSR chief of fatality investigations and a DSR safety engineer performed an on-site investigation of the incident. Meetings and interviews were conducted with the acting Chief (Assistant Chief) and officers of the department; firefighters; representatives from the Office of the State Fire Marshal; and the local sheriff’s office. NIOSH investigators also reviewed diagrams of the incident, training records, photographs, witness statements, run sheets, dispatch tapes, the coroner’s report, the state Fire Marshal’s report, and the county sheriff’s report.
Fire Department
The combination fire department involved in this incident had seven front-line responding apparatus from one station and 30 uniformed volunteer fire fighters. The acting Chief (Assistant Chief) was the only paid fire fighter at the department. The department served a rural population of approximately 25,000 in an area of about 26 square miles. The fire department did not have written standard operating procedures (SOPs).
Victim's Training and Experience
According to fire department records, the victim was a fire fighter for six years, and attended 149 hours of fire fighter-related training in addition to EMS training - all received at the fire department. Training dates ranged from a period of December 2000 through May 2006.
Apparatus and Equipment
First Alarm
Deputy Chief (victim)—Personally Owned Vehicle (POV)
Engine 402 (E-402)—Captain (initial IC), FF #1
Fire fighter #2 (FF#2) —POV
Engine 406 (E-406)—Assistant Chief (IC), 1 FF
Tanker 404 (T-404)— 2 FFs
Rescue 405—1 FF
2 Medic units (county EMS services)
Second Alarm (after the victim had fallen through the floor hole)
4 mutual aid departments
Note: Total resources that responded to this incident consisted of 11 apparatus, 2 advanced life support (ALS) units, 1 basic life support (BLS) unit, and 44 fire fighters.
Structure
The one-story ranch-style residential structure was approximately 2,000 sq. ft. (main floor) in size, and it was built in 2004 of wood-frame construction. There was a partial unfinished basement of approximately 1,200 sq. ft. The exterior was finished with horizontal vinyl siding. The main level flooring system was comprised of pre-engineered I-joists that measured 26’ in length x 18” deep, with 3 ½” flanges. The joists were set 19 ½” on center. Two main beams supporting the system were 26’ long and consisted of 2” x 12” laminated beams. The floor decking in the area of the hole consisted of ¾” oriented strand board (OSB), covered by ¼” luan and vinyl tile. The structure was heated and cooled via natural gas and electricity. There was a glass-enclosed porch covering an in-ground pool that was attached to Side C of the home (Photo 1 and Figure 1).
 |
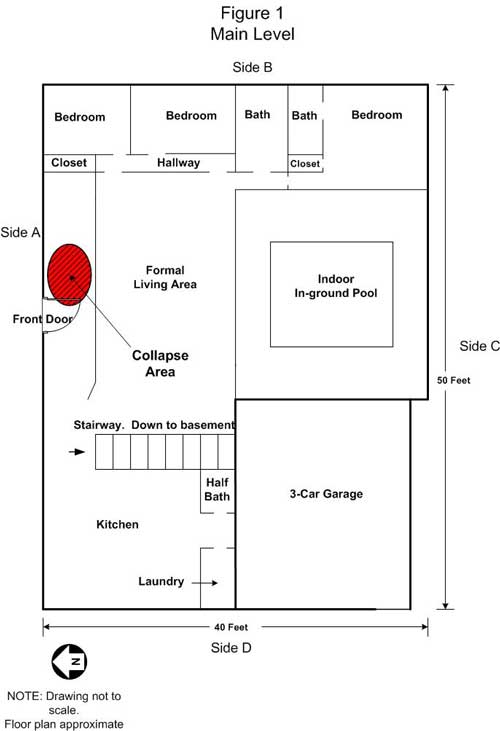 |
Figure 1. Main Level |
Weather
A severe thunderstorm had recently passed through the area, and light rain and winds persisted throughout this incident.
On June 25, 2006, at approximately 1429 hours, a neighbor called 911 to report a lightning strike and that there was light smoke coming from the residence. (Note: A severe thunderstorm had passed/was passing through the area at the time. The thunderstorm also incapacitated the 800 MHz radio system in the area, complicating the dispatch of the department and the subsequent communication between the fire department and the 911 center). The initial caller indicated that there was no one home at the time and that the residents were gone for the day. At 1430 hours, the fire department received tones for dispatch, but it received no audio. The Assistant Chief reported attempting to contact the 911 center via the 800 MHz system to no avail. He also reported attempting to contact the 911 center on low band, also to no avail. He then called the 911 center on his cell phone and informed the 911 dispatcher that the department had heard tones, but no audio. At 1432, the department was re-dispatched via low-band by the county 911 dispatch.
The victim was the first to arrive on-scene in his POV at approximately 1438 hours. Initial size-up indicated that there was nothing apparent, and the victim radioed to incoming units to slow, but continue their response. (Note: there was heavy rain in the area at this time). After completing his size-up, the victim discovered that the windows in the front of the house were darkened, and upon his opening the front door, heavy smoke rolled out.
The victim immediately radioed all incoming units to return to “signal 10” response (lights/sirens). Shortly thereafter, E-402 (Captain #1, FF#1) arrived on scene at approximately the same time as a county medic unit. (Note: the 911 center in this area did not have time-stamp capability at the time of the incident; therefore, exact times are unknown). Both units positioned on the A-side of the residence.
The volunteer Captain who arrived on E-402 (Captain #1) declared initial incident command (IC). The victim and IC conversed briefly and decided to make entry through the front door with a 1 3/4” pre-connected hand line charged by a compressed air foam system (CAFS) for search/rescue and to search for the seat of the fire. (Note: the pump operator (Captain # 1) noted that they were using 60gpm/60cfm class “A” foam at 125psi). The IC also served as pump operator. After going on air, the victim and FF#1 (the entry team) entered the structure through the front door (A-side) entrance at approximately 1442 hours, noting that a section of the floor just to the left of the front door had already given way. Once inside to the right approximately 6 feet, the team realized the floor under them was very hot and “spongy.” At the same time, the conditions inside the structure became untenable, with intensifying heat and “zero visibility” as a result of thick, black smoke. Within 30-45 seconds of making entry, the victim informed FF#1 that they were going to evacuate to get a light. As they exited the structure, they pulled the hose line out with them. The victim stayed at the front entrance with the nozzle and sent FF#1 to E-402 to retrieve a box light and to pull another pre-connect. (Note: at this point, team integrity was compromised leaving one fire fighter operating alone in close proximity to the fire.) After retrieving the light, the victim instructed FF#1 to stretch the additional line around to the B-side to hit the fire in the basement through a window (Note: the basement window led to a crawl space, so no water actually hit the basement, or the fire). Also, during this time, FF#2 set up a positive pressure ventilation (PPV) fan at the entrance on side A.The victim stayed at the front entrance (alone a second time) to reportedly attack the fire through the hole in the floor just to the left of the entrance (see Photo 2 and Figure 2).
 |
Photo 2: Depicts the failed floor from above. Note the front door in the upper left-hand corner. Photo courtesy of the fire department. |
 |
Figure 2. Basement Layout. |
Around this time, the Assistant Chief arrived on scene in E-406, along with one fire fighter, but did not assume IC. As the Assistant Chief made his way to A-side of the structure, he saw a hose going down through a hole in the floor just inside the main entrance (see Photo 3). He yelled down into the hole and heard a muffled reply. He could not hear what the victim was saying, so he turned down the positive pressure ventilation (PPV) fan and then very clearly heard the victim yell for help (Note: it was stated by the Assistant Chief that the clarity of the victim’s voice indicated that he had apparently taken his SCBA mask off to communicate). The Assistant Chief immediately called to E-402 for a 14’ roof ladder to be placed into the hole in the floor. At this time, FF#1 returned to A-side and started to slide down into the hole (prior to the ladder being placed) to try to retrieve the victim.
 |
Photo 3 illustrates the floor failure area, viewed from the basement. Photo courtesy of the fire department
|
The basement area to the left of FF#1 (A-B corner in basement) as well as the unfinished ceiling and unprotected floor joists were burning and FF#1 had to use a handline to put water on the fire before descending. As soon as FF#1 reached the lower level, his low-air alarm went off. FF#1 immediately climbed out of the basement and went to replace his air bottle. FF#2 and the Assistant Chief then attempted to position the 14-foot ladder for safe access into the basement, but as a result of debris and clearance inadequacies, the ladder did not reach the lower level. Once the ladder was somewhat in place, the Assistant Chief and FF#2 descended into the basement and immediately found the victim near the hole in the floor. The victim was dragged to the area of the basement stairs. FF#2 stated that when he was with the victim, he shook him, pinched his ear lobe in an attempt to elicit a response, and checked for a pulse (Note: FF#2 was also an emergency medical technician who reported that the victim was unresponsive, with his mask off at this time). The homeowner arrived on scene and made the fire department aware that a 900 pound safe was positioned in the area above where the Assistant Chief and FF#2 were working. The safe was on the East wall – near the center of the room and had fallen into the main support of the structure. The Assistant Chief and FF#2 moved the victim from under this area. By this time, T-404 (two fire fighters) and R-405 (one fire fighter) had arrived on scene, as well as several fire fighters via POV. FF#1 returned with a fresh air bottle just as FF#2 ascended the ladder.
The Assistant Chief then came out of the structure due to being low on air, assumed IC and immediately advised dispatch (at approximately 1450 hours) that they had a fire fighter down and he requested mutual aid. FF#1 started to descend the ladder but part of the burned-out floor supporting the ladder gave way and FF#1 fell into the basement injuring his knee. Since the ladder attempt was not successful at retrieving the victim, additional members quickly formed to enter the house, traversed the floor, and gained interior access to the basement to assist FF#1 and to retrieve the victim (Photo 4). The victim was found almost immediately and was unresponsive. The initial crew experienced great difficulty in moving the victim over to and up the basement stairs because of the debris into which the victim had fallen and the limited personnel available to move the victim. After approximately 20 minutes, with the help of these other fire fighters, the crews were able to remove the victim. (Note: Difficulty in moving the victim highlights the need for adequate staffing on hand before beginning offensive fire fighting operations.) Immediate medical treatment was provided, and an ambulance transported him to the hospital, where he was pronounced dead. FF#1 was treated for his injured knee.
 |
Photo 4: Basement layout showing stairway to main level of house. |
According to the County Coroner, the cause of death was carbon monoxide intoxication.
Discussion: Engineered I-joists represent an emerging technology within the building sector, and they offer a number of advantages over traditional construction methods that incorporate standard framing materials. Engineered I-joists are lighter in weight. They are stiffer and will not warp, twist, or shrink like traditional framing materials. Engineered I-joists also reduce total construction time and labor costs by virtue of their ease of installation. Engineered I-joists have become readily available only in the past 15 years.
NIOSH Fire Fighter Fatality Investigation and Prevention Program findings from this investigation and a previous report1 of fire fighters falling through floors into burning basements of residential homes prompted a literature search that identified research showing that pre-engineered wooden I-joists floor systems may fail earlier than other systems under direct flame impingement. The Illinois Fire Service Institute (IFSI), at the University of Illinois, “conducted tests to help determine the structural stability of sample floor systems” and published its findings in 1988.2 These studies suggest that engineered wooden I-beams can fail in as little as 4 minutes and 40 seconds under controlled test conditions.
While objective time-to-failure studies of the various lightweight flooring systems being used today have been conducted only in limited cases, evidence from two FFFIPP investigations suggest and seems to support the fact that engineered I-joists quickly lose strength and integrity when damaged and weakened by heat exposure and flame impingement. (Photo 5) Often, the weakened I-joists can be difficult to detect from above as the floor surface above may still appear intact. Fire fighters who operate on floors above fire-damaged engineered I-joists may fall through the weakened floor and become trapped in the fire below. Incident commanders and fire fighters should be aware that these members can fail quickly and without warning, and they should plan interior operations accordingly.
 |
Photo 5: Depicts the significant damage suffered by the webbing of the I-joists as compared to the flanges. This damage resulted in floor instability and failure. Photo courtesy of the fire department. |
Discussion: According to NFPA 1720, “The responsibility for assigning fire companies at an emergency belongs to the incident commander, who establishes priorities and assigns units based on identified objectives.”3 In addition to conducting an initial size-up, the IC must maintain an awareness of the location and function of all companies or units at the incident, initiate and maintain accountability, and control communications for the tactical, command, and emergency traffic channels for the incident. To effectively coordinate and direct fire-fighting operations on the scene, it is essential that adequate staff be available for immediate response to ensure that the IC is not required to become involved in fire-fighting efforts. In this incident, the IC was involved in non-command functions, such as operating the pump on E-402.
Discussion: NFPA 1500 Section 8.3: Risk Management During Emergency Operations, states that “The incident commander shall integrate risk management into the regular functions of incident command."4 Additionally, NFPA 1500 notes that “The concept of risk management shall be utilized on the basis of the following principles:
The NFPA 1500 Annex A.3.3.69.1 provides information that will assist in determining offensive vs. defensive operations. It reads, “Defensive operations are generally performed from the exterior of structures and are based on a determination that the risk to personnel exceeds the potential benefits of offensive actions.”4 Simply stated, risk vs. gain is an evaluation of the potential benefit that a task will accomplish, weighed against the potential risks to fire personnel. Basic guidelines are outlined in the Fire Fighter’s Handbook5:
Discussion: Team continuity involves knowing who is on your team and who the team leader is, staying within visual contact at all times (if visibility is obscured, then teams should remain within touch or voice-distance of each other), communicating needs and observations to the team leader (officer), rotating to rehab and staging as a team, and watching the other team members (practice a strong “buddy-care” approach).6 These key factors help to reduce serious injury or even death resulting from the risks involved in fire-fighting operations by providing personnel with the added safety net of fellow team members. As teams enter a hazardous environment together, they should leave together and stay together to ensure that team continuity is maintained. Fire fighter accountability is an important aspect of fire ground safety that can be compromised when teams are split up. Names on coats, reflective shields or company numbers on helmets, and helmet and turnout clothing colors are visual ques that fire fighters can use to maintain team continuity in poor visibility. In this incident, the victim (Deputy Fire Chief) sent his partner away from the area to perform duties while he stayed alone in the immediate area presumably to attack the fire in the basement from above.
Discussion: Fire departments should have a rapid intervention team (RIT) standing by during any structure fire to rescue a trapped, injured, or missing fire fighter. NFPA 1500, section 8.5.7 states that: “In the initial stages of an incident where only one crew is operating in the hazardous area at a working structural fire, a minimum of four individuals shall be required, consisting of two individuals working as a crew in the hazardous area and two individuals present outside this hazardous area available for assistance or rescue at emergency operations where entry into the danger area is required.” Further, NFPA 1500, section 8.8.7 states that: “At least one dedicated RIT shall be standing by with equipment to provide for the rescue of members that are performing special operations or for members that are in positions that present an immediate danger of injury in the event of equipment failure or collapse.”4 In this incident, the minimum four fire fighters were not present, nor was a RIT team assembled and ready. All rescue attempts were made by fire fighters on-scene who assembled independently and entered the structure without coordination through incident command, first traversing the same floor that had failed in the area to reach the basement access door. In areas where response time is lengthy, a qualified RIT team should always be part of the initial alarm assignment.
Discussion: A trend in the fire service is that some smaller fire companies are adopting the aggressive fire-fighting tactics of larger, well staffed departments. Some of these smaller fire departments do not have the training, equipment, and back-up personnel to accomplish these dangerous tactics safely.7 In this incident, an interior attack was initiated with the only two fire fighters with bunker gear on the scene, and no back-up crew available. Operations should remain defensive until adequate resources arrive to assure interior fire fighter safety. In rural areas and areas with long response times, automatic mutual aid should be established to ensure enough fire fighters arrive in a timely manner to safely perform fireground tasks. Fire departments need to ensure that adequate staffing is available prior to responding to the event. The typical 1000 sq. ft residential house requires approximately 750 gallons per minute (gpm) water flow for extinguishment. Typical staffing on a first alarm to initiate a coordinated fire attack would require 1 fire fighter at the hydrant, 1 fire fighter at the pump panel, 3 hoselines operating at 175 gpm (3 fire fighters on each hoseline = 9 fire fighters), 2 fire fighters assigned as a RIT Team and 1 Incident Commander equals a minimum of 14 fire fighters on the first alarm to initiate water supply and hoseline operations.
Discussion: Communication between fire fighters while they are wearing SCBA face pieces, particularly in a burning building, is difficult. Many SCBA face pieces muffle and distort the voice of the fire fighter wearing them under normal conditions and circumstances. This problem can be magnified when common fireground background noise is added. Several manufacturers now offer battery-powered voice amplifiers with electronic emitters that mount directly to the compatible SCBA face piece and allow the voice of the SCBA wearer to be amplified and projected a much greater distance and with higher clarity over background noise. In this investigation, after first noticing the victim in the basement, the Assistant Chief stated that he could not understand what the victim was saying, and heard only a muffled voice. Immediately after this, he stated that he could hear the victim very clearly, indicating that the victim had probably taken off his SCBA mask in order to communicate.
Discussion: The fire department involved in this incident did not have an established standard operating procedure (SOP) regarding thermal imaging camera (TIC) use at structure fires. TICs can be a useful tool for initial size-up and for locating the seat of a fire. Infrared thermal cameras can assist fire fighters in quickly getting crucial information about the location of the source (seat) of the fire from the exterior of the structure, so that they can plan an effective and rapid response with the entire emergency team. Knowing the location of the most dangerous and hottest part of the fire may help fire fighters determine a safe approach and avoid structural damage in a building that might have otherwise been undetectable. Ceilings and floors that have become dangerously weakened by fire damage and are threatening to collapse may be spotted with a thermal imaging camera. A fire fighter about to enter a room filled with flames and smoke can use a TIC to assist in judging whether it will be safe from falling beams, walls, or other dangers. The use of a thermal imaging camera may provide additional information the Incident Commander can use during the initial size-up. Thermal imaging cameras (TICs) should be used in a timely manner, and fire fighters should be properly trained in their use and be aware of their limitations.8 In this incident, three TIC cameras were stored in the department apparatus but were not utilized during the incident.
Discussion: Fire fighters must act promptly when they become lost, disoriented, injured, low on air, or trapped.9-14 First, they must transmit a “may day” while they still have the capability and sufficient air to communicate. The next step is to manually activate their PASS device. To conserve air while waiting to be rescued, fire fighters should try to stay calm and avoid unnecessary physical activity. If not in immediate danger, they should remain in one place to help rescuers locate them. They should survey their surroundings to get their bearings and determine potential escape routes, and they should stay in radio contact with Incident Command and rescuers. Additionally, fire fighters can attract attention by maximizing the sound of their PASS device (e.g., by pointing it up in an open direction), by pointing their flashlight toward the ceiling or moving it around, and by using a tool to make tapping noises. A crew member who initiates a Mayday call for another person should quickly try to communicate with the missing member via radio and, if unsuccessful, initiate a Mayday providing relevant information as described above.
Discussion: Positive pressure ventilation has become popular and is a useful tool but the Incident Commander must have information as to the fire location, progress and control prior to use. The key to successful positive pressure venting is to control the outlet openings. If too many doors and windows are opened, positive pressure venting will prove ineffective. As with all other ventilation methods, there is a negative side to positive pressure venting. The fire can be pushed toward victims, their escape routes, or into unburned areas.6
Discussion: The National Fire Protection Association, NFPA 1221 Standard for the Installation, Maintenance, and Use of Emergency Services Communications Systems, 2007 Edition, contains a number of requirements for emergency services dispatch systems. Specifically, Chapter 9 contains requirements for a secondary alarm dispatching system so that in the event of a failure of the primary system, a means to switch to the secondary system is immediately available to the telecommunicator.15 In this incident, severe thunderstorms in the area had incapacitated the local 800 MHz radio system. The Assistant Chief reported attempting to contact the 911 dispatch center via the 800 MHz radio system to no avail after an alarm tone was heard at the fire department. The Assistant Chief called the 911 dispatch center on his cell phone and informed the dispatcher that the department had received tones but no audio.
This investigation was conducted by Robert E. Koedam, Chief of the Fatality Investigations Team, and Timothy Merinar, Safety Engineer, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH, located in Morgantown, WV. A technical review was provided by Deputy Chief William Goldfeder, Loveland-Symmes Fire Department and editor of http://www.FireFighterCloseCalls.com.

Return to Fire Fighter Homepage
![]()
This page was last updated on 09/20/07.