
On November 7, 2005, a 32-year-old male career fire fighter/engineer (the victim) was fatally injured during a silo fire at a livestock feed supplement manufacturing plant. As the fire was being contained in one silo, the victim and the department’s training officer were directed to search for fire extension in an adjacent silo. The victim, who was dressed in full turnout gear and wearing his self-contained breathing apparatus (SCBA), received operating instructions from a plant employee on the use of a manlift to access the top of the silo. About one minute later, as the victim was being elevated, the manlift came to an abrupt stop. After investigating potential problems with the manlift, a plant employee climbed a fixed ladder and found the victim wedged between the manlift and the edge of the floor opening on the fourth level. The victim was not breathing and was unresponsive. The plant employee used the victim’s radio to call “fire fighter down.” Several minutes later, a Captain climbed the fixed ladder to the fourth floor and tried chest compressions with no success. The victim was later pronounced dead on the scene. NIOSH investigators concluded that to minimize the risk of similar occurrences, fire departments should:
Additionally, owners/managers of manufacturing plants should
On November 7, 2005, a 32-year-old male career fire fighter/engineer (the victim) was fatally injured during a silo fire at a livestock feed supplement manufacturing plant. On November 9, 2005, the U.S. Fire Administration (USFA) and the International Association of Fire Fighters (IAFF) notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. On December 13 - 16, 2005, a General Engineer and the Senior Investigator from the NIOSH Fire Fighter Fatality Investigation and Prevention Program investigated this incident. A meeting was conducted with the Chief and Deputy Chief of the involved fire department, two representatives from the State Fire Marshal’s Office, and the manufacturing plant’s general manager. Interviews were conducted with officers and fire fighters who were at the incident scene. The NIOSH investigators reviewed the department’s standard operating guidelines (SOGs), the Fire Marshal’s report, the victim’s training records, photographs of the incident scene, written witness statements, dispatch transcriptions and the coroner’s report. The victim’s protective clothing, SCBA, and manually activated PASS device were examined and photographs of the PASS device obtained. A site visit of the incident scene was made and photographs were taken.
Fire Department and Apparatus
The combination department has two stations with a total of 27 career and 8 volunteer fire fighters serving a population of about 18,000 residents in a geographic area of approximately 92 square miles. The victim responded on Tanker #5 [T5]. Engine #1 [E1] , Engine #3 [E3], Tanker #4 [T4], Ladder #1 [L1], and a Deputy Chief from the responding fire department were also on scene preceding the fatal event.
Training/Experience
The victim had completed the National Fire Protection Association (NFPA) Fire Fighter Level I and II training and a Confined Space Entry Program, in addition to various administrative and technical courses. The victim was a career fire fighter with more than 12 years fire fighting experience. The victim had been a volunteer fire fighter for 6 years before becoming a career fire fighter in 1999.
Building Information
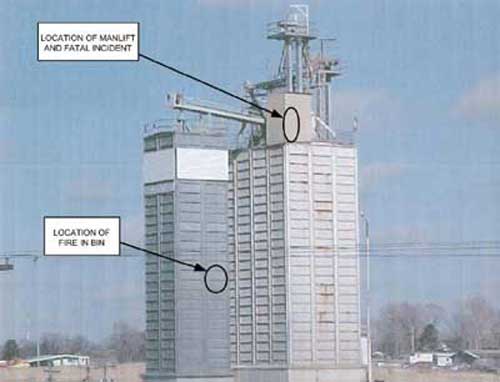
The building was a multi-level, non-sprinklered livestock feed supplement manufacturing plant that was constructed of sheet metal walls and roof over a wood frame with lightweight wood trusses and 2 metal silos (see Photo1).
At 1254 hours, on November 7, 2005, five apparatus (T5, E1, E3, T4, and L1) were dispatched from two stations of the same department to a livestock feed supplement manufacturing plant with a reported silo fire. The Deputy Chief had arrived on scene at 1301 hours, via a fire department truck, and indicated nothing showing just prior to establishing incident command. At 1302 hours, the victim arrived on the scene in T5, and E1 arrived seconds later. At 1304 hours, E3 and T4 arrived on scene. Upon arrival, the Deputy Chief met with the plant’s general manager, who indicated that wheat hulls were on fire in one of the bins in the west silo. A plant employee stated that there might be more than one fire because there were 5 separate bins in the 100 foot tall silo. The Deputy Chief was told that there were approximately 75,000 pounds of product in the silo.
Accountability tags were collected by the Deputy Chief from all crews as an attack 1 ¾-inch pre-connect hose line, from E1, was advanced to the bottom of the silo bin. Shortly thereafter, a second line was brought into the bottom of the silo bin for backup. At 1324 hours, L1 arrived on scene.
The Deputy Chief requested that the Captain from E1 send a couple of fire fighters to the top of the west silo where light smoke was visible to determine the status of the fire and to check for fire extension. The ladder on L1 only extended to 75 feet and could not reach the top of the silo. The only access to the top of the west silo was via a manlift in the east silo or a fixed ladder attached to the manlift’s frame and then over a catwalk to the west silo. The Captain from E1 requested that the victim and the Training Officer finish bunkering up and take the manlift to the top of the east silo then cross the catwalk to check for fire extension. The Training Officer and victim donned their SCBAs and entered the plant where they met a plant employee who escorted them to the manlift. The employee instructed the victim and the Training Officer on how to operate the manlift by pulling on a cord that ran adjacent to the belt. (Note: The manlift traveled from the plant’s basement through four floor openings to the top floor which was approximately 100 feet high.)
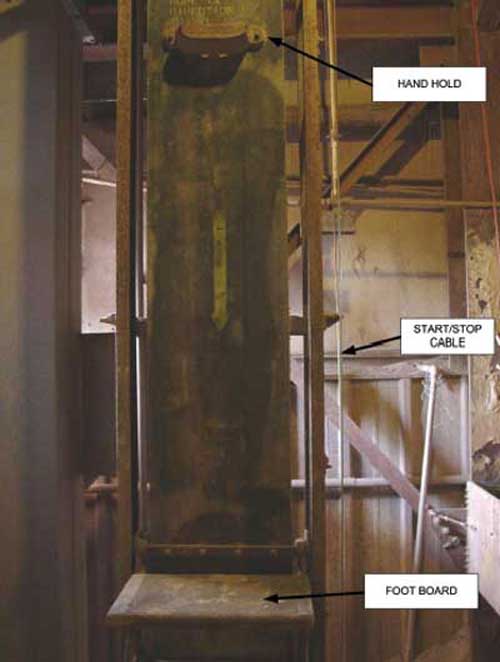
Since the manlift could only accommodate one individual at a time, the victim stepped on the manlift’s foot board and went up first (see Photo 2). About a minute passed and the manlift stopped abruptly. The Training Officer thought the victim had made it to the top and had gotten off the manlift. The manlift’s foot board was not lined up at the ground floor level so the Training Officer and plant employee tried to operate the manlift to get it to line up to the ground floor level; however, the manlift did not move. The Training Officer tried to radio the Captain from E1 (who was assisting the interior crew) that they were having difficulty with the manlift, but his radio was not operating properly. The plant employee checked the electrical control panel for the manlift and found no problem, and informed another employee of the situation. The second employee climbed the ladder that is part of the exterior frame support of the manlift to assess the situation. When he got to the top he saw that the victim was entrapped between the manlift and the edge of the floor opening. He went to the edge of the east silo and called for help. The IC could see him, but could not understand what was being said. The employee realized no one could understand what he was saying so he retrieved the victim’s radio on the floor of the manlift and communicated – “fire fighter down.”
At 1332 hours, the IC radioed that someone was down and advised the Captain from E1 that they needed to send someone up top to check out the situation. The Captain from E1 started climbing the manlift ladder but needed to stop at the third level (about ¾ the way up) because of fatigue. The Captain from L1 then climbed the ladder, passed the E1 Captain on the third level, and made it to the victim where he immediately checked for vital signs and proceeded to do chest compressions. The Engineer from T4 also climbed the ladder to the third level where he called the Captain from L1 and asked what assistance was needed. The L1 Captain responded that the victim was dead on scene. The Engineer from T4 continued to climb to the top where he checked the victim’s vital signs and found none.
The victim apparently did not experience any difficulty in riding the manlift to the third level. However, when he traveled through the fourth floor opening, his SCBA became wedged between the edges of the floor opening and caused the victim to be compressed by the manlift frame. The access opening which the manlift passed through was about 20 inches from the manlift belt to the floor edge (see Photo 3). The victim with bunker gear and SCBA was estimated to be 24 inches wide. The top of the SCBA cylinder hit the bottom edge of the floor opening. About a third of the diameter of the cylinder contacted the bottom edge of the floor opening (see Photo 4). When the cylinder didn’t clear the opening, the victim was pulled backwards while the manlift continued upward. This action forced the victim’s legs to bend at the knees pushing them into the metal frame support of the manlift. The backside of the cylinder, about 1/3rd in from the top of the cylinder, hit the outside edge of the manlift foot platform pushing the bottom of the SCBA into the victim’s back. Thus, the victim’s chest was compressed by the SCBA harness straps and his lower back sustained pressure from the lower part of the SCBA harness causing positional asphyxia.
The coroner listed cause of death as positional asphyxia due to entrapment between the manlift and floor access opening.
Discussion: National Fire Protection Association (NFPA) 1620 § 2-2.6.2 states “the pre-incident plan should be the foundation for decision making during an emergency situation and provides important data that will assist the incident commander in developing appropriate strategies and tactics for managing the incident.”1 This standard states that “the primary purpose of a pre-incident plan is to help responding personnel effectively manage emergencies with available resources. Pre-incident planning involves evaluating the protection systems, building construction, contents, and operating procedures that can impact emergency operations.” A pre-incident plan identifies deviations from normal operations and can be complex and formal, or simply a notation about a particular problem such as the presence of flammable liquids, explosive hazards, structural damage from a previous fire, or mechanical hazards that may be present. NFPA 1620 outlines the steps involved in developing, maintaining, and using a pre-incident plan by breaking the incident down into pre-, during- and after-incident phases. In the pre-incident phase, for example, it covers factors such as physical elements and site considerations, occupant considerations, protection systems and water supplies, and special hazard considerations. The presence of concealed spaces or difficult areas to navigate, such as traveling through floor openings with the aid of a manlift, can be noted in pre-incident visits and referenced. The access opening through the fourth floor was smaller than the floor openings of the preceding three levels which could have been noted during the pre-incident planning process.
Discussion: In this case, the victim apparently did not turn on his manual PASS device while conducting a search for fire extension. The Training Officer and plant employees were in positions where they could have heard the PASS alarm, if it was alarming. Although its unknown if a rescue would have been successful if the alarm had been heard, especially at 100 vertical feet, it’s still important that PASS devices are checked on a regular basis and activated during fire fighting activities.
When fire departments only have manual PASS devices, they should maintain a policy of activation of all PASS devices on the fire ground and especially when conducting interior operations. Recognizing the problem of individuals not activating their PASS, many fire departments are utilizing automatic activating models. The NFPA 1982: Standard on Personal Alert Safety Systems, 1998 Edition, recommends automatic activation PASS devices.2
Discussion: With increasing complexity in equipment and response techniques, written standard operating guidelines (SOGs) provide individual fire department members an opportunity to read and maintain common understanding of operational procedures. The NIOSH Alert: “Preventing Injuries and Deaths of Fire Fighters”3 identifies a need to follow and establish fire-fighting policies and procedures. Guidelines should be reviewed, revised and fully implemented to be effective and enforceable. In this case, the department SOGs were inadequate, in that they had not been reviewed, revised, or trained on for 10 years. This could address guidelines for manually activating the PASS and assuring radios are in working order.
Discussion: The fireground communications process combines electronic communication equipment, a set of standard operating procedures or guidelines, and the fire fighters who will use the equipment. To be effective, the communications network must integrate the equipment (which is to be in proper working order) and procedures or guidelines (which should include equipment maintenance) with the dynamic situation at the incident site, especially in terms of the human factors affecting their use. The incident management system shall include standard operating guidelines (SOGs) for radio communications that provide for the use of standard protocols and terminology at all types of incidents.4 Fire departments should review both operating procedures and human factors issues to ensure effective radio communication on the fireground. NFPA 1221 addresses emergency communications needs.5
In this case, the training officer, who was waiting to go up the man lift behind the victim, tried to radio the IC that the manlift was not operating after the victim went up, but his radio did not function reportedly due to a low battery.
Discussion: Owners/managers of manufacturing plants should identify hazards and mark or eliminate those hazards not only for the safety of employees, but for emergency responders as well. In this case, the plant had been in existence since the late 1930’s and the manlift was installed at that time. Since then, codes have been developed for manlifts which include floor opening specifications. According to the Occupational Safety and Health Administration (OSHA) manlift safety requirements for floor openings (29 CFR 1910.68(b)(5)(i)), floor openings for both “up” and “down” runs shall be not less than 36 inches nor more than 40 inches for a 16-inch belt (applicable to this incident) and shall extend not less than 24 inches, nor more than 28 inches from the face of the belt. In this incident, the opening from the face of the belt was approximately 20 inches which is about 4 inches less than the minimum required.6 The floor openings of the preceding three floors were within the minimum requirement.
This incident was investigated by Matt Bowyer, General Engineer and Richard Braddee, Senior Investigator with the Fire Fighter Fatality Investigation and Prevention Program, Division of Safety Research at NIOSH.
 |
 |
 |
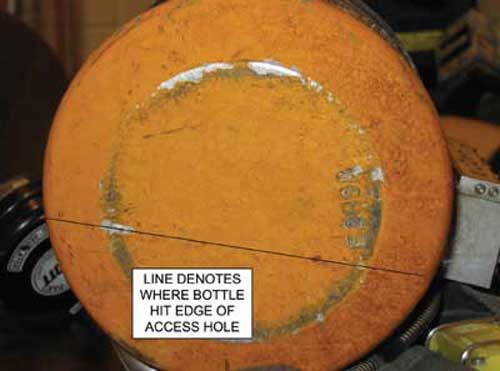 |
Photo 4. Impact line on top of SCBA bottle from edge of floor opening. |

Return to Fire Fighter Homepage
![]()
This page was last updated on 08/24/06.