
On April 8, 2004 a 71-year-old male volunteer Chief (the victim) was seriously injured during a church fire when he was struck by bricks and burning debris that fell from an outward collapse of a brick façade. The victim died from his injuries four months later. He had arrived at the scene of the fire one minute after the first alarm and approximately 15 minutes before the collapse. He assumed Incident Command, performed a 360° size-up of the scene, and was in front of the church verbally calling for fire fighters to evacuate the structure when the collapse occurred. The victim was transported by helicopter to a hospital and later transferred to a rehabilitation center where he remained until August 1, 2004 when he died from his injuries.
NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should:
Additionally, municipalities should:
 |
Photo courtesy of the fire department. |
On August 1, 2004, four months after being injured, a 71 year-old male volunteer Chief died. The victim was struck by bricks and burning debris that fell from an outward collapse of a church façade. On August 3, 2004, the United States Fire Administration notified the National Institute for Occupational Safety and Health (NIOSH) of the fatality. On September 22, 2004, an investigator from the NIOSH Fire Fighter Fatality Investigation and Prevention Program investigated the incident. The investigator visited the fire scene and interviewed the officers and fire fighters who were on the scene at the time of the incident. The investigator met with representatives from the police department and reviewed fire and police dispatch records. The incident was also investigated by the Federal Bureau of Alcohol, Tobacco, and Firearms, the State Bomb and Arson Squad, and the State Occupational Safety and Health Administration. Their findings were reviewed by the NIOSH investigator. Copies of the department's standard operating procedures (SOPs), the victim’s training records, and the death certificate were also reviewed.
Department
The volunteer department is comprised of one fire station and serves a population
of about 2,250 in an area of about three square miles. There are approximately
20 volunteer fire fighters in the department.
Training and Experience
The 71 year-old victim had been with the department for 48 years and had served
as Chief for the last 12 years. During his 48 years of service, the victim completed
hundreds of hours of training. Records from the most recent three years document
131 hours of training including engine operator, hazardous materials, personal
protective equipment, and officer training.
Equipment and Personnel
There were four fire apparatus (Engine 1 [E1], Engine 3 [E3], Engine 5 [E5]
and Truck 2 [T2]) on the scene when the collapse occurred at 1045 hours. E1
with a fire fighter/driver arrived on the scene at 1033 hours. T2 arrived on
the scene at 1036 hours and was driven by the victim’s son (FF1) who was
one of the fire fighters injured during the collapse. E3 and E5, each with a
fire fighter/driver, radioed that they were on the scene at 1036 hours. The
victim and the other fire fighter who was injured during the collapse (FF2)
arrived via their personal vehicles. By the time the fire was brought under
control, there were 59 fire service personnel from three companies, seven apparatus,
and one emergency medical unit on site.
Structure
The structure was a functioning church that was originally built in 1870. It
was a single story building of wood-frame construction and had a partial basement
with approximately 2,233 total square feet of useable space. The church was
renovated in 1920 and exterior walls of brick veneer were constructed over the
wood frame at that time. The gabled roof was covered by wood and composition
shingles. The interior walls were made of wood panels. There was a suspended
acoustic tile ceiling in the vestibule area where it is believed the fire originated.
Flooring consisted of carpet over a pre-existing wooden floor. Until the mid
1960’s, the church was heated by a free-standing coal stove. A church
officer reported to arson investigators that coal dust had accumulated within
the walls and above the ceiling which may have contributed to a rapid fire-spread.
The building was not equipped with a sprinkler system or smoke detectors.
Weather
The weather was fair and sunny with a temperature of approximately 70º
F. The wind was blowing at about 5 miles-per-hour. There is no indication that
weather was a contributory factor in this fatality.
On the morning of April 8, 2004 at 1029 hours, a volunteer department was dispatched to a working church fire. At the time of the initial alarm, the victim was leaving the town hall which is one block from the church. He arrived at the scene of the fire via his personal vehicle at 1030 hours, assumed Incident Command and performed a 360° size-up of the scene. He radioed at 1031 hours that he saw no signs of fire, but following a walk-around of the structure, radioed at 1032 hours that heavy smoke was showing.
The scene of the fire was located two blocks from the fire station and the first apparatus arrived within four minutes of the initial alarm. E1 manned by a fire fighter/driver radioed he was on the scene at 1033 hours. T2, which was driven by the victim’s son (FF1), radioed he was on the scene at 1036 hours. Also arriving at 1036 hours was E5 from the victim’s department and E3 from a mutual aid department.
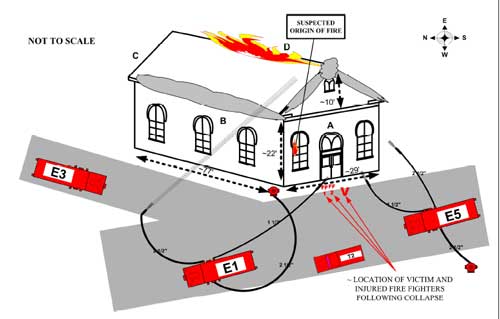
At approximately 1038 hours, FF1 and FF2 donned full turnout gear and masked-up before forcibly entering the front of the structure. They carried a charged 1½” line off of E5. At 1042 hours FF1 radioed for a pike pole to pull ceiling tile in the AB corner of the vestibule and check for fire extension where it was believed the fire had originated. At approximately the same time, two fire fighters had pulled a 2½” line off of E1 and set up in the street near the AB corner of the church. The fire fighters were directing a water stream onto the AB roof corner toward the front of the structure (see Diagram).
The victim had just completed a 360° walk-around of the structure. He was wearing civilian pants and shoes, but had donned his turnout coat and helmet. Very quickly, thick gray smoke began to appear near the A side roof apex, the AB corner, and out of the front upper level window. Flames were just beginning to show at the roof ridgeline and appeared to be moving toward side A (Photo 1). It is believed that the victim made the decision to evacuate the structure when he witnessed the quickly deteriorating conditions. He began walking toward the front entrance of the church while verbally calling for FF1 and FF2 to immediately come out of the structure. At approximately 1045 hours, as the two fire fighters exited the structure through the front door, the entire roof collapsed inward and the brick façade above the gutter line on the A side wall fell outward onto the street (Photo 2). The victim was in front of, and facing, the A side wall. The falling burning debris struck him and the impact caused him to fall backwards into the street. He was removed from the debris in less than a minute, but suffered burns and multiple body traumas. FF1 and FF2 were also struck by the debris as they exited the church. At the time of the collapse, both fire fighters were in, or very near, the front doorway. It is believed they were protected from more serious injuries due to their proximity to the A side wall and the protection of their turnout gear. The injured fire fighters were transported to a local hospital where they were treated and released. The victim was air lifted to a hospital and later transferred to a rehabilitation center where he remained until his death on August 1, 2004.
The cause of death was identified by the medical examiner as multiple blunt force trauma and thermal injuries.
Discussion: According to NFPA 15001, the Incident Commander shall integrate risk management into the regular functions of Incident Command. The concept of risk management shall be utilized on the basis of the following principles:
The offensive versus defensive command decision is an ongoing one that requires continual evaluation of these major factors throughout the attack.
Klaene and Sanders2 state that structural conditions bear heavily on, and the entire operation is governed by, the offensive/defensive decision. An operation that begins as an offensive attack sometimes changes to defensive, but the actions being taken during either attack must be coordinated as offensive or defensive; they must never be both. Brunacini3 states that “the offensive and defensive modes are independent events. Effective fire operations (safe, sane, and predictable) are conducted either on the inside or the outside of the building. Any mixture of the two basic modes begins to set the stage for loss of life and property.”
In this incident, fire fighters set up a 2½” handline in the street to the north of the AB corner of the church. They directed the stream toward flames beginning to show near the roof apex at the A wall. During this same period of time, two fire fighters entered the front of the church with a charged 1½” line to check for fire extension in the front vestibule area. The collapse occurred approximately fifteen minutes after the first alarm and just as fire fighters were evacuating the structure.
Discussion: Upon arrival, and at any time during a structure fire, if size-up determines that structural integrity is questionable, a collapse zone must be established. A collapse zone is an area around and away from a structure in which debris might land if the structure fails. This area should be equal to the height of the building plus an additional allowance for debris scatter, and at a minimum should be equal to 1½ times the height of the building.4 For example, if the wall were 20 feet high, the collapse zone boundary should be established at least 30 feet away from the wall.
Knowledge of building construction and how fire reacts in a building can assist in making determinations of structural stability. Dodson outlines the following seven-steps to assist fire scene personnel in analyzing the potential for structure collapse.5
Immediate safety precautions must be taken if factors indicate the potential for a building collapse. All persons operating inside the structure must be evacuated immediately and a collapse zone should be established around the perimeter. Once a collapse zone has been established, the area should be clearly marked and monitored, to make certain that no fire fighters enter the danger zone.
According to Dunn, structural collapse during firefighting can be expected to increase and one factor contributing to the increase is the age of buildings.6 Older buildings can be weakened due to age. Structures may become badly deteriorated as wood shrinks and rots, and mortar loses its adhesive qualities. One estimate identifies 75 to 100 years as the age at which buildings begin to deteriorate and conditions may contribute to collapse. In this incident, the original church structure had been built approximately 130 years ago.
It is believed the victim had recognized the quickly deteriorating conditions and the possibility of a collapse when he decided to call for the fire fighters to evacuate the church. Neither the victim nor the two fire fighters had time to escape from the collapse zone and were struck by falling debris.
Discussion: Evacuation signals are used when command personnel decide that all fire fighters should be evacuated from a burning building or other hazardous area because conditions have deteriorated beyond the point of reasonable safety. All fire fighters should be familiar with their department’s method of sounding an evacuation signal. There are several ways this communication can be done. The two most common methods are to (1) broadcast a radio message ordering all fire fighters to evacuate, and (2) sound an audible warning device (air horn) on the apparatus at the fire scene for an extended period of time.7 The message should be broadcast several times to make sure everyone hears it.
In this incident, the victim walked toward the structure to personally call to the fire fighters who were working just inside the front door. This department’s evacuation signal is three sustained blasts from the air horn. The collapse occurred before the order for the signal was given.
Discussion: According to NFPA 1500 Chapter 7, “The fire department shall provide each member with the appropriate protective clothing and protective equipment to provide protection from the hazards to which the member is or is likely to be exposed. Such protective clothing and protective equipment shall be suitable for the tasks that the member is expected to perform. Protective clothing and protective equipment shall be used whenever the member is exposed or potentially exposed to the hazards for which it is provided.”1
The victim in this incident was wearing his bunker coat and helmet. However, he was not wearing bunker pants or boots which may have contributed to the gravity of his injuries.
Discussion: SOGs are a set of organizational directives that establish a standard course of action on the fireground to increase the effectiveness of the fire fighting team. SOGs are characterized as being written and official. They are applied to all situations, enforced, and integrated into the management model. They generally include such areas as: basic command functions; communications and dispatching; fireground safety including discussions on risk management and establishing a collapse zone; guidelines that establish and describe tactical priorities and related support functions; method of initial resource deployment; and an outline of responsibilities and functions for various individuals and units.8 Unwritten directives may be difficult to learn, remember, and apply. One approach to establishing SOGs is to have officers and fire fighters decide how all operations will be conducted and then commit to those decisions in writing.
It is imperative that companies perform their duties as described in their SOGs unless directed or approved by the Incident Commander (IC) to do otherwise. Dunn states “A standard operating procedure (or guideline) provides accountability and control. It is a general plan of who does what and when. It lets companies know where they should be operating and what they should be doing. A standard operating procedure should be created for the most frequent type of fire to which a company responds.”9
An example of pertinent interior/exterior fire-ground operation guidelines are listed below:10
The department SOGs should declare that fire extinguishment and control must consider fire fighter safety first.
At the time of the incident, this department had administrative SOPs but no documented specific and detailed procedures for fireground operations.
Discussion: NFPA 1620 provides guidance to assist departments in establishing pre-incident plans. Pre-incident planning that includes agreements formed by a coalition of all involved parties including mutual aid fire departments, EMS companies, and police, will present a coordinated response to emergency situations, and may save valuable time by a more rapid implementation of pre-determined protocols.11 Mutual aid companies should train together and not wait until an incident occurs to attempt to integrate the participating departments into a functional team. Differences in equipment and procedures need to be identified and resolved before an emergency where lives may be at stake. Procedures and protocols that are jointly developed, and have the support of the majority of participating departments, will greatly enhance overall safety and efficiency on the fireground. Once methods and procedures are agreed upon, training protocols must be developed and joint-training sessions conducted to relay appropriate information to all affected department members.12
By the time the fire was brought under control, there were 59 fire service personnel from three companies, seven apparatus and one emergency medical unit on site. Coordination of fireground efforts may have been enhanced if pre-incident planning and joint training had taken place among mutual aid departments.
Discussion: Building codes and standards are currently used as guidelines for preserving newly constructed buildings and improving occupant safety. However, before municipalities adopted or enforced specific codes and standards, many buildings were designed and constructed without incorporating such standards. NFPA 909, Code for the Protection of Cultural Resource Properties – Museums, Libraries, and Places of Worship,13 states that according to a recent NFPA study of fires that occurred in houses of worship, from 1987 to 1998 an average of 1,580 places of worship were seriously damaged or destroyed by fire each year. This equated to four properties per day with an annual average for direct property damage totaling $44.2 million dollars.
NFPA 909 B.4.2.3 states that “a properly designed automatic sprinkler system is the most effective single means of preventing serious fires. Automatic sprinklers combined with good building design and fire-resistive construction, finishes, and furnishings are the best way to ensure safer places of worship.” There is also a strong possibility that sprinklers could reduce fire fighter fatalities, since they contain, and even extinguish, fire prior to the arrival of the fire department. The structure involved in this incident did not have a sprinkler system.
This incident was investigated, and the report was authored, by Virginia Lutz, Safety and Occupational Health Specialist, NIOSH, Division of Safety Research, Surveillance and Field Investigation Branch.
 |
 |
 |
Photo 2. After collapse of roof and facade.
Photo courtesy of the fire department. |

Return to Fire Fighter Homepage
![]()
This page was last updated on 01/23/06.