
On October 27, 2003, a 49-year-old male volunteer Assistant Chief (the victim) was fatally injured after being struck by a privately owned vehicle (POV) at a road construction site. At approximately 2145 hours, the victim and six other volunteer fire fighters responded in three fire apparatus to a reported smoking generator at a road construction site. Two of the three fire apparatus returned to the fire department. The victim and two other fire fighters remained with the brush truck to wait for a representative of the construction company. Upon leaving, the crew stopped to replace a road-closed barricade at the entrance to the construction site. Shortly thereafter, a civilian in a POV failed to make the turn necessary to detour around the construction site and struck the victim who was standing next to the brush truck. The victim was dragged about 60 ft and then trapped beneath the truck. He was declared dead at the scene.
NIOSH concludes that, to minimize the risk of similar occurrences, fire departments should:

Incident Scene
On October 27, 2003, a 49-year-old male volunteer Assistant Chief (the victim) died after being struck by a privately owned vehicle (POV) at a road construction zone. On October 30, 2003, the U.S. Fire Administration (USFA) notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. On November 19-20, 2003, a safety and occupational health specialist from the NIOSH Fire Fighter Fatality Investigation and Prevention Program, Division of Safety Research, investigated the incident. The NIOSH investigator met with the Chief of the career division and the Chief of the volunteer division of this combination fire department, the two fire fighters who were with the victim at the time of the incident, and the investigating police officer. The NIOSH investigator visited the site of the incident, and reviewed the department’s standard operating procedures (SOPs), the police report and photographs, and the medical examiner’s report. The State Occupational Safety & Health Administration (OSHA) incident report was reviewed. The OSHA investigator later was interviewed by phone.
Department
This combination fire department has 55 career fire fighters in 4 stations and
25 volunteers in 2 stations. It serves a population of approximately 67,000
in an area of about 48 square miles. Volunteer fire fighters are paid an hourly
rate while in training or on duty.
Training
The victim had been Assistant Chief of the volunteer division for 4 years and
a volunteer fire fighter for 18 years. The victim had over 265 hours of training
including Apparatus Operation. He was certified as NFPA Fire Fighter Level I
& II. As required by the State, the victim took a minimum of 24 hours of
training per year. There was no record of the victim having had specific training
on safe work practices while responding to calls in or near moving traffic.
Road and Weather Conditions
The incident occurred at the entrance to a construction site where road and
utility upgrades were in progress. The construction had been ongoing for over
three months at the time of the incident. Near the construction site, the main
road narrowed from four lanes to two, the pavement ended, and the main highway
was closed. Main traffic heading south on the highway was detoured to the southeast
via a sharp left turn. The detour was marked by 20 mph construction and curve
signs. A traffic lane was formed using orange plastic barrels located on both
shoulders (Photo 1). The temporary road at the detour
site consisted of dirt and gravel and had a rough, washboard surface. According
to the State OSHA report and the investigating police officer, a representative
of the state Department of Transportation (DOT) office visited the construction
site and verified that appropriate traffic control signs (Road Work Ahead, Reduced
Speed Limit 20 mph, and curve signs) and barricades appeared to be in place
at the time of the incident. At the time of the incident, it was dark and the
temperature was 34 degrees F with light rain.
Apparatus
A tanker, an engine and a brush truck responded to the call. The engine and
the tanker returned to the station leaving behind a brush truck, with a crew
of three, including the victim, to wait for the owner of the generator. The
brush truck was a 2001 heavy-duty pick-up. It was equipped with a specially
designed slide-in unit that held 200 gal of water and 15 gal of foam, both of
which were full at the time of the incident. The headlights and emergency flashers
(strobe lights in the grill and rotating light bars on top) were all in operation
at the time of the incident.
Personal Protective Equipment
All of the crew on the brush truck, including the victim, were wearing turnout
gear without helmets. This gear has horizontal stripes with retroreflectivea
material: two around the coat - one near the bottom of the coat and another
10 inches above; two stripes on each sleeve, 6 inches apart; and a stripe 4
inches above the bottom of each pant leg. The color of the background material
is brown for the volunteer division and black for the career division.
On October 27, 2003, at 2137 hours, this fire department was dispatched for a smoking generator at a road construction site. Seven fire fighters in three apparatus – an engine, a tanker and a brush truck - responded at approximately 2145 hours. The victim responded in the tanker with two other fire fighters. The generator was located about one mile inside the road construction site, i.e., one mile beyond the barricades. Fire fighters moved one of the barricades to allow the apparatus to enter. When they examined the generator they determined that the problem was not a fire but an electrical malfunction. They then contacted the contractor and instructed him to come and shut down the generator. The tanker and the engine crews returned to the station leaving behind the brush truck to wait for the owner of the generator. The victim decided to ride back in the brush truck.
As soon as the company representative arrived (approximately one hour later), the brush truck crew and the victim departed for the fire station. At the entrance to the construction site, just north of the road-closed barricades, they stopped to replace the barricade they had moved upon entering. They parked their brush truck facing north with its engine running, headlights on, and emergency flashers operating. All three fire fighters exited the truck. As he reached for the barricade, one of the fire fighters reported that he saw a POV heading towards them that was fishtailing and which seemed to be moving well in excess of the posted speed limit of 20 mph. He yelled “look out” and, along with another fire fighter, dove out of the way. The southbound POV, a 1994 pickup, failed to make the sharp left-hand turn necessary to detour around the construction site. It then hit the left front corner of the brush truck, continued along the side of the truck, and struck the victim who was standing towards the rear. The victim was dragged approximately 60 feet before the POV came to a stop (Photo 2). The POV had struck three construction barrels on the right shoulder of the roadway before striking the brush truck and the fire fighter.
The two surviving fire fighters approached the driver of the POV to check his condition and then looked for the victim. They found the victim underneath the front of the POV. The front of the POV was resting on its left front axle because its left front tire had broken off and folded up under the vehicle. The fire fighters briefly checked for the victim’s pulse and then went to their brush truck to get equipment and call for help. When they returned to the victim, the driver of the POV had left the scene on foot. Additional fire units, an ambulance, and police officers arrived shortly thereafter. The victim was declared dead at the scene.
The police searched throughout the night for the driver of the POV but were unable to locate him. He turned himself in to police the next morning.
The cause of death according to the autopsy report was craniocerebral injuries and closed head trauma.
Discussion: As stated in NFPA 1451 (8.1.4.1), “fire service vehicles shall be utilized as a shield from oncoming traffic whenever possible.” Apparatus should be angled on the roadway to create a physical barrier between the work area and approaching traffic. Emergency personnel should stay within the “shadow” created by the blocking apparatus at all times. Forward-facing lights such as headlights should be turned off to prevent distracting motorists traveling in the opposite direction.
Discussion: Fire fighters working in or near moving traffic are in danger of being struck by motor vehicles. Department SOPs can help establish safe work practices in such situations. SOPs should include, but not be limited to, the following: positioning apparatus to provide a physical barrier between responders and moving traffic, operating defensively (e.g., never turn your back on traffic when working in a non-secure area), methods to establish a secure work area, releasing the scene back to normal operation, and wearing appropriate personal protective apparel. An example of an SOP for safe positioning of apparatus while operating in or near moving traffic can be found at http://www.respondersafety.com. At the time of the incident, the fire department did not have an SOP regarding this topic.
Discussion: Emergency responders should operate defensively with an awareness of the high risk associated with working in or near moving traffic. As emphasized on the respondersafety.com website, responding emergency service personnel should “never trust approaching traffic.” Motorists may ignore traffic signs and regulations for various reasons including poor visibility, distraction, being under the influence of alcohol or drugs, and/or because of a medical condition that affects their judgment or abilities. Nighttime incidents are especially hazardous due to reduced visibility and slowed driver reaction time to hazards. Training should include, but not be limited to, positioning apparatus to create a physical barrier between traffic and the work area, and wearing helmets and high-visibility safety apparel at all times. Because each incident varies, all emergency responders should have ongoing, appropriate, task-specific training.
This incident occurred at night, and, although traffic was detoured around the construction zone via signs, barrels, and barricades, a POV failed to make the turn necessary to avoid the construction area and struck the victim who was standing inside the construction zone.
Discussion: Personnel working in or around moving traffic need to be highly visible, especially at night. Personnel working in such settings are considered “highway workers” by the Department of Transportation (DOT) and, thus, fall under the Manual on Uniform Traffic Control Devices (MUTCD) regulations. Section 6E.02 of the MUTCD describes high-visibility clothing requirements. For daytime work, the standard requires that the (flagger’s) vest, shirt, or jacket must be either “orange, yellow, yellow-green, or a fluorescent version of these colors.” Retroreflective trim is essential for visibility at night. For nighttime work, the DOT requires that similar outside garments must be retroreflective. The retroreflective material must be either “orange, yellow, white, silver, yellow-green, or a fluorescent version of these colors, and must be visible at a minimum distance of 300 m (1,000 ft).” The American National Standards Institute (ANSI) published a standard for high-visibility safety apparel (ANSI/ISEA 107-1999) which specifies the type and amount of material needed in apparel to enhance the visibility of workers under hazardous situations, day or night.
The background color of the victim’s turnout gear was brown. It had retroreflective stripes on the coat, sleeves and pants and likely was visible at night. Relying solely on turnout gear, however, is problematic. It is not as visible as a safety vest (e.g., it is not fluorescent and therefore not as visible during the day) and its effectiveness may be diminished due to exposure to heat, soot, and dirt from fire ground operations. Although wearing a safety vest may not have prevented this incident, it is good safety practice to wear one over the turnout coat for increased visibility during all roadway incidents, day and night. A vest that meets ANSI Class 3 requirements is preferred. In addition, it is good practice to wear a helmet during such work.
This incident was investigated by Linda Frederick, Safety and Occupational Health Specialist, Division of Safety Research, Surveillance and Field Investigations Branch, NIOSH.
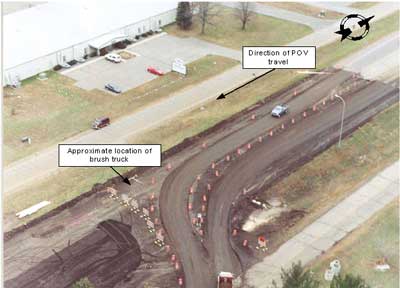 |
Photo 1. Aerial view of detour around construction
site - Courtesy of Police Department |
 |
Photo 2. Incident Scene - Courtesy of Police
Department |

Return to Fire Fighter Homepage
![]()
This page was last updated on 07/01/04.