Structural Collapse at an Auto Parts Store Fire Claims the Lives of One Career Lieutenant and Two Volunteer Fire Fighters - Oregon
SUMMARY
On November 25, 2002, at approximately 1320 hours, occupants of an auto parts store returned from lunch to discover a light haze in the air and the smell of something burning. They searched for the source of the haze and burning smell and discovered what appeared to be the source of a fire. At 1351 hours they called 911. Units were immediately dispatched to the auto parts store with reports of smoke in the building. Fire fighters advanced attack lines into the auto parts store and began their interior attack. Crews began opening up the ceiling and wall on the mezzanine where they found fire in the rafters. Three of the eight fire fighters operating on the mezzanine began running low on air. As they were exiting the building, the ventilation crews on the roof began opening the skylights and cutting holes in the roof. The stability of the roof was rapidly deteriorating forcing everyone off the roof. The IC called for an evacuation of the building. Five fire fighters were still operating in the building when the ceiling collapsed. Two fire fighters escaped. Attempts were made to rescue the three fire fighters while conditions quickly deteriorated. Numerous fire fighters entered the building and removed one of the victims. He was transported to the area hospital and later pronounced dead. Approximately 2 hours later, conditions improved for crews to enter and locate the other two victims on the mezzanine. The victims were pronounced dead about an hour later by the Deputy Medical Examiner.
NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should
Incident Site
INTRODUCTION
On November 25, 2002, a 46-year-old male career Lieutenant (Victim #1), a 30-year-old
male volunteer fire fighter (Victim #2), and a 33-year-old male volunteer fire
fighter (Victim #3) died when the roof collapsed at an auto parts store. On
November 26, 2002, the U.S. Fire Administration notified the National Institute
for Occupational Safety and Health (NIOSH) of this incident. On December 11,
2002, two Safety and Occupational Health Specialists, the NIOSH Fire Fighter
Fatality Investigation and Prevention Program’s Team Leader and a Safety
Engineer investigated this incident. Meetings were conducted with the Chief
of the fire department, Battalion Chief of Administration, the local International
Association of Fire Fighters (IAFF) representative, the City Manager, a Senior
Fire Investigator from the National Fire Protection Association (NFPA), and
the Deputy State Fire Marshal who also investigated this incident. Interviews
were conducted with the officers and fire fighters who were at the incident
scene. The investigators reviewed the victims’ training records, the department’s
standard operating procedures (SOPs), the fire department’s incident report
and the Deputy State Fire Marshals’ report. The incident site was visited
and photographed.
Four self-contained breathing apparatus (SCBA) units, three worn by the victims, were sent to the NIOSH Respirator Branch in Bruceton, Pennsylvania, for further evaluation. The fourth unit had not been involved in this incident but had a reported problem in function. The purpose of the testing, requested by the fire department, was to determine each SCBA’s conformance to the approval performance requirements of Title 42, Code of Federal Regulations, Part 84 (42 CFR 84). Further testing was conducted to determine conformance to the National Fire Protection Association (NFPA) Air Flow Performance requirements of NFPA 1981 - Standard on Open-Circuit Self-Contained Breathing Apparatus for the Fire Service, 1997 Edition. Two of the victims’ units were too heavily damaged to safely be pressurized and tested. The other two units were subjected to seven performance tests. The low-air alarm of one of the victim’s units was not functional, causing the SCBA to fail the Remaining Service Life Indicator Test and NFPA Air Flow Performance Test. The low-air alarm of the other unit was out of adjustment, causing it to fail the Remaining Service Life Indicator Test. It also failed the Alarm Sound Level Test by sounding at less than the required 80 decibel sound level (a report summarizing this evaluation is included as an Appendix). Note: Additional evaluations of these units have been requested by the fire department. The final report will be posted to the internet as an Appendix to this report when available.
The combination fire department involved in this incident is comprised of 19
career fire fighters and 25 volunteer fire fighters serving a population of
approximately 16,000 in a geographical area of about 10.5 square miles.
Training and Experience
Victim #1 was a career Lieutenant who had approximately 14 years of experience
with this combination fire department and a total of 23 years of experience
as a fire fighter. He was certified NFPA Fire Fighter Level I & II, as a
Driver/Operator, and as a Fire Service Instructor. Additional training included
tactical operations for company officers I & II, fire fighting tactics and
strategy, building construction, and fire fighter safety and survival.
Victim #2 was a volunteer fire fighter who had approximately 3 years of experience with this combination fire department and a total of 10 years of experience as a fire fighter. He was certified NFPA Fire Fighter Level I & II, as a Driver/Operator, and as a Fire Service Instructor.
Victim #3 was a volunteer fire fighter who had approximately 8 years of experience
with this combination fire department and a total of 15 years of experience
as a fire fighter. He was certified NFPA Fire Fighter Level I & II and as
a Driver/Operator.
Equipment and Personnel
Initial dispatch response included:
• Engine 8132 (Victim #1, Victim #2, Victim #3, Fire Fighter #4 and Fire
Fighter #5 [Driver/Operator], and an aerial operator)
• Engine 8131 (Driver/Operator and two fire fighters)
• Rescue 8171 (Driver and a fire fighter)
• Ladder 8151 ( Fire Fighter #1, Fire Fighter #2 and Fire Fighter #3[Driver/Operator])
• Staff 8101 (Chief - IC)
• Command 8111 (On-duty Battalion Chief).
Mutual-aid combination fire department response:
• Engine 8306 (Officer and five fire fighters)
• Staff Vehicle 8301 (Chief Officer)
• Staff Vehicle 8302 (Chief Officer)
• Staff Vehicle 8303 (three fire fighters)
• Ladder 8310 (three fire fighters).
Additional personnel from both departments arrived on the scene in their personally
owned vehicles.
Additional units were dispatched on subsequent alarms; however, only those
units directly involved in the fatal event are discussed in the investigation
section of this report.
Structure
The structure was built in approximately 1938 and was of Type IV heavy timber
construction. The building had numerous modifications which included the addition
of a warehouse and a mezzanine. This was a non-sprinklered building encompassing
approximately 13,520 square feet of floor space. The ceiling was comprised of
8-inch wide by ¾-inch thick old-growth fir ship lap, with 3/8-inch Furtex
glued to the surface. The ceiling was attached to 2-inch by 10-inch wood ceiling
joists. The height of the ceiling in the sales area was approximately 14-feet
and at the mezzanine was 7-feet. The roof was constructed of the same material
and in the same manner as the ceiling. The roof was supported by 2-inch by 13-inch
wood roof rafters and 9-inch by 9-inch wooden posts supporting 9-inch by 13-inch
wooden beams.
INVESTIGATION
On November 25, 2002, at approximately 1320 hours, the occupants of an auto parts store returned from lunch and discovered a light haze in the air and could smell something burning. The occupants searched the store but could not find the source of the haze or smell. One of the occupants went outside and on the North side of the building (B-Side) put a ladder up to the roof. He went to the roof but was unable to find anything. After exiting the roof, he met the occupant from the attached automotive machine shop. They discussed the haze and smell of something burning. Together they returned to the roof where they found the chimney to be hot to the touch. They exited the roof, entered the auto parts store, and noticed a red glow in the bathroom area on the mezzanine. Note: The red glow was caused by the fire above the ceiling and behind the wall. They attempted to extinguish the red glow with a portable fire extinguisher. Their attempts to extinguish the red glow were unsuccessful so the occupants called 911 at 1351 hours.
At 1351 hours, units were dispatched to an auto parts store with reports of fire in the ceiling of the bathroom. Initial dispatch response included Ladder 8151, Engine 8132, Rescue 8171, Engine 8131, Staff 8101, and Command 8111. Command 8111 (Battalion Chief) arrived on the scene, assumed command (initial Incident Commander [IC]), and reported nothing showing (no visible fire or smoke) to Central Dispatch. The property owner approached the initial IC and informed him that the fire was near the chimney in the bathroom on the mezzanine and that all of the occupants had exited the building. The IC could see a light haze of smoke at the drop ceiling level. Ladder 8151 arrived on the scene and the IC informed one of the fire fighters as to the location of the fire.
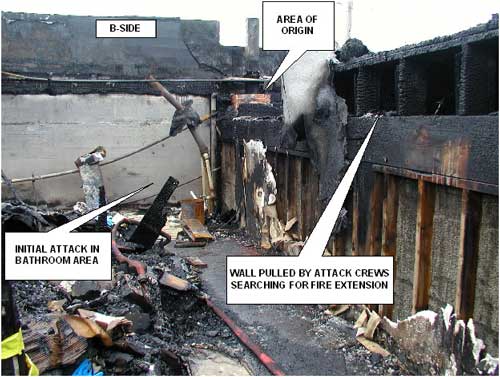
At 1356 hours, the Chief (Staff 8101) of the fire department arrived on the scene. The initial IC (Command 8111) transferred command to the Chief. Brown smoke was now visible at the roof level near the chimney with no visible fire. The IC then radioed responding units to advise them that it was a working fire in a commercial structure. The property owner, standing near the front door (A-Side) with the IC, pointed toward the mezzanine and said that the fire was in the bathroom up on the mezzanine (Photo 1 and Diagram 1).
Fire Fighter #1 and Fire Fighter #2 from Ladder 8151 advanced a 1 ¾-inch handline (200 foot pre-connect) through the front door. The two fire fighters advanced the line toward the north end of the sales counter. They saw fire at the ceiling level approximately 20-25 feet from the front wall in the northwest corner of the building. Note: It is believed that the fire was coming from a scuttle/vent space. The crew then applied water and knocked the fire down. The two fire fighters repositioned the line to the center of the sales counter before proceeding down the center aisle leading to the stairs of the mezzanine (Diagram 1). The two fire fighters could hear crackling as they reached the stairs (Diagram 2).
The Battalion Chief (initial IC) assisted in establishing a water supply to Ladder 8151. He was ordered by the IC to do a walk-around of the building as part of the size-up of the incident. The IC requested mutual-aid units from Central Dispatch. Engine 8132 arrived on the scene and fire fighters from the Engine pulled a 1 ¾-inch back-up line off Ladder 8151.
Fire Fighter #1 and Fire Fighter #2 advanced the attack line to the top of the stairs and onto the mezzanine. They advanced to the back wall of the mezzanine where they saw, to their left, the fully involved bathroom (B-Side of building). Note: The two fire fighters reported to NIOSH investigators that at this point, they encountered a light haze of smoke and very little heat on the mezzanine. They began their attack on the bathroom area and knocked the fire down. They opened up the ceiling near the bathroom and found fire in the rafters which they quickly knocked down. Three fire fighters (Victim #3, Fire Fighter #3 and Fire Fighter #4) advanced two handlines from Ladder 8151 to the counter and continued with one handline to the mezzanine. Note: Fire fighters reported to NIOSH investigators that the lights in the building were still on and that there was a grayish/brownish colored smoke at what they believed to be the ceiling level. The actual ceiling height was deceiving because of the drop ceiling and suspended lights above the sales counter and shelving (Diagram 2). They encountered heavy smoke conditions with no visible fire upon reaching the top of the mezzanine. They met up with the two fire fighters on the initial attack line and assisted them with pulling ceiling material. The crews then began pulling wall material and attacking the fire between the rafters of the automotive machine shop (Diagram 1 and Photo 1). Fire Fighter #5 and Victim #2 entered the front of the building and followed the handlines to the mezzanine. Victim #1 entered the building and proceeded to the mezzanine. In an attempt to clear smoke from the mezzanine, Fire Fighter #5 searched for windows to open along the back wall and in the office. There were now eight fire fighters (Victims #1 - #3 and Fire Fighter’s #1- #5) operating with two handlines along the back wall of the mezzanine. Victim #1 radioed command requesting roof ventilation and for a positive pressure ventilation (PPV) fan to be set up on the A-Side of the building.
At approximately 1408 hours, mutual-aid units began arriving on the scene. Engine 8306 was ordered to the rear of the building to protect the exposure (five fire fighters from Engine 8306 were assigned by the IC to the roof to perform vertical ventilation). Staff 8301 (Chief of mutual-aid combination department) became the Division “C” command and Staff 8302 (Assistant Chief of mutual-aid combination department) the Incident Safety Officer (ISO). Engine 8131 arrived on the scene.
Five fire fighters from mutual-aid Engine 8306 and a fire fighter from Engine 8131 were now on the roof (accessed via Ladder 8151) and radioed command that they were ready to begin ventilating the roof. A small flame could be seen near the chimney on the B-Side of the building (this was determined by the State Fire Marshal to be the point of origin).
Fire fighters on the C-Side of the building were now pulling handlines off Engine 8306 and advancing them into the automotive machine shop. The Division “C” command officer entered the shipping and receiving area from the C-Side and proceeded to a man-door that led to the auto parts store (the door was located directly below the mezzanine). He opened the door and heard crews operating on the mezzanine above him. Crews on the C-Side were now in the automotive machine shop attacking the fire near the point of origin (Diagram 1). Note: There was little to no fire damage in the automotive machine shop and shipping and receiving area portions of the building.
As the interior attack crews continued pulling wall and ceiling material on the mezzanine, they experienced a momentary loss of water pressure. Note: There were delays in establishing a water supply to Ladder 8151 as personnel were having difficulty with the Storz coupling. Ladder 8151 has a 375 gallon tank that was initially utilized until they were successful in hooking up to a hydrant. Fire Fighters #1, #2, and #4 were now low on air and proceeded to exit. Fire Fighter # 3 radioed command and requested additional manpower. Fire Fighter #4 passed the nozzle to Victim #3 who was still working near the bathroom. As Fire Fighter #4 was exiting, he ran into Victim #1 near the corner of the break room where he provided details of what they had encountered and accomplished. Visibility was now reduced to zero but the heat was still relatively mild. As the three fire fighters proceeded toward the top of the stairs they passed two more fire fighters (believed to be Victim #2 and Fire Fighter #5). Note: At this time five fire fighters were operating on the mezzanine (Victim #1, Victim #2, Victim #3, Fire Fighter #3 and Fire Fighter #5). Victim #2 and Victim #3 each had a nozzle and were hitting fire between the rafters of the automotive machine shop while Victim #1 (working with Victim #3 near the bathroom) and Fire Fighter #5 (working with Victim #2 along the back wall of the mezzanine) continued pulling ceiling and wall material (Photo 1).
As the three fire fighters followed the handline down the stairs they heard the skylights on the roof being broken out. Four fighters on the roof were breaking out the skylights. Two other fire fighters began cutting a 6- by 8-foot hole, to the east, approximately 15 feet from the chimney (point of origin). Initially, no smoke was coming from the first skylight but then it began emitting a heavy dark gray smoke. Crews proceeded to break out the second skylight where heavy smoke began billowing out.
Fire Fighters #1, #2, and #4 exited the building and approached the IC to inform him of what they had completed and the location of the fire. The IC passed command to Command 8111 (Battalion Chief [initial IC]) so that he could go to the roof to check on roof operations. The crew on the roof requested a handline. The senior fire fighter in charge of the ventilation crew noticed that the roof began to feel “spongy” and told his crew members that the roof was getting weak. The senior fire fighter in charge of the ventilation crew ordered the crew off the roof. After the Chief reached the roof he could see the roof tar bubbling, smoke along the wall near the A/B-corner, and heavy smoke pushing out of the skylights. He also noticed that the roof felt “soft” and “spongy” near the A-Side wall.
Fire Fighter #3 was now low on air and proceeded to leave the mezzanine. Fire Fighter #5 passed his flashlight to Victim #2 when his low-air alarm began sounding. He followed the hose line to the top of the stairs. As he reached the top of the stairs he was knocked to the bottom of the stairs by falling debris. Fire Fighter #3 was near the bottom of the stairs and was knocked to the floor. Note: It is believed that Victim #3 was directly behind Fire Fighter #5 when the ceiling collapsed. Victim #1 and Victim #2 were behind Victim #3. As Fire Fighter #5 was knocked to the bottom of the stairs, Victim #3 was either partially trapped at the top of the stairs or was knocked over the stair railing. Victim #1 and Victim #2 received the full force of the ceiling collapse and were covered in debris near the corner of the break room (Photo 2). Fire Fighter #3 was out of air and forced to exit the building. As Fire Fighter #5 gained his bearings he could see that the mezzanine area was now fully involved with fire. He yelled for the other fire fighters on the mezzanine but did not receive a response. In an attempt to get their attention he began pulling on the hose line, but did not get a response. He then ran out of air and was forced to exit the building.
As the ventilation crew was exiting the roof, the Chief ordered an evacuation of the building. Command 8111, who was still acting as the IC, radioed for crews to evacuate the building. Drivers and fire fighters began blowing the air horns on the apparatus on the A-Side of the building. Note: The department’s evacuation procedure is for an announcement over the radio by the IC and for apparatus air horns to be blown. Central Dispatch does not make a simultaneous evacuation notice. The Chief was the last to leave the roof. As he was climbing onto the ladder he could see one of the skylights drop into the building. A deep red flame and heavy smoke began blowing out of the hole. Fire Fighter #5 now exited the building, ran into the Incident Safety Officer (ISO) and told him to radio the fire fighters that were still inside. The ISO, along with other officers and fire fighters, attempted to radio the three fire fighters still inside. They did not receive a response.
As the Chief got off the ladder he heard Fire Fighter #5 report that there were fire fighters still in the building and that there was some kind of an explosion. The Chief (now acting as the IC), ordered the ventilation crew to become the Rapid Intervention Team (RIT). Additional handlines were pulled from the various apparatus to protect the egress on the A-Side of the building. The Division “C” command officer proceeded through the automotive machine shop to the man-door below the mezzanine after being informed of the missing fire fighters. He opened the door and could hear personal alert safety systems (PASS) sounding overhead on the mezzanine. A personnel accountability report (PAR) was conducted. Note: Victim #1, Victim #2, and Victim #3 were noted as still missing in the building. The identity of Victim #2 was not known until a fire fighter reported Victim #2’s identity to the IC. The RIT entered the A-Side of the building in an attempt to locate the three missing fire fighters. The fire began to intensify rapidly as the front windows began to break. Fire was now visibly rolling along the ceiling from the back toward the front of the auto parts store. The RIT had made two separate attempts to enter and search the building before they were forced to exit the building.
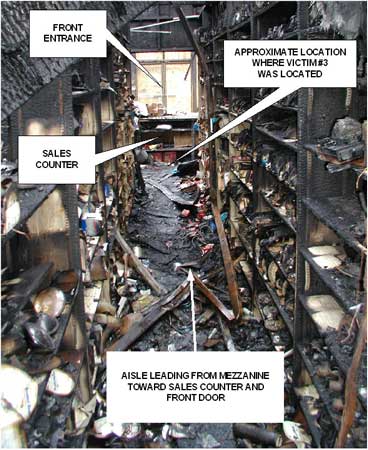
Approximately 5 minutes later, Fire Fighter #1, operating a 2 ½-inch handline near the front of the building, reported to the IC that he could hear a personal alert safety system (PASS) sounding. Fire Fighter #1 and Fire Fighter #5 (who had changed out his SCBA air bottle with a new one) entered the building and approached the sales counter. Fire Fighter #5 climbed over the counter and found Victim #3 (Diagram 1, Diagram 2, Photo 3 and Photo 4). Note: Victim #3 was found face down with his face mask on and all of his protective gear in place. Apparently he was able to find the handlines leading from the mezzanine stairs to the front of the building. Fire Fighter #1 exited and asked crews to assist in retrieving Victim #3. Numerous fire fighters entered and were able to remove Victim #3. He was provided advanced life support measures by the Medic 5 crew before being transported to the area hospital where he was later pronounced dead.
An additional mutual-aid department arrived on the scene and a second attempt was made to enter and search the building for Victim #1 and Victim #2. The crews on the C-Side of the building attempted to perform a rescue operation but were unsuccessful. A second evacuation was ordered as conditions still remained too dangerous for crews to operate on the interior of the building.
Operations went defensive until, approximately 2 hours later, conditions improved for crews to enter and locate Victim #1 and Victim #2 on the mezzanine. Crews left Victim #1 and Victim #2 in place for further examination by the State Fire Marshal and the Deputy Medical Examiner. The victims were pronounced dead about an hour later by the Deputy Medical Examiner (Diagram 1, Diagram 2, Photo 2 and Photo 4).
CAUSE OF DEATH
The cause of death as recorded on the death certificates for all three victims was asphyxiation.
RECOMMENDATIONS/DISCUSSIONS
Recommendation #1: Fire departments should ensure that fire fighters provide the Incident Commander with interior size-up reports. 1-5
Discussion: Interior size-up is just as important as exterior size-up. Since the Incident Commander (IC) and other command officers, including the Incident Safety Officer (ISO), are staged outside, the interior conditions should be communicated to them as soon as possible. Knowing the location and the size of the fire inside the building lays the foundation for all subsequent operations. Interior conditions could change the IC’s strategy or tactics and provide the ISO with key information for risk management decisions. For example, if heavy smoke is emitting from the exterior roof system, but fire fighters cannot find any fire in the interior, it is a good possibility that the fire is above them in the roof system. It is important for the IC and ISO to immediately obtain this type of information to help make the proper decisions. Departments should ensure that the first officer or fire fighter inside the structure evaluates interior conditions and reports them immediately to the IC. Dunn states “if the fire has spread to the space above the ceiling immediately notify the officer in command of the fire. Also, if you discover a suspended ceiling communicate this information to command. Never pass fire that threatens to cut off your retreat.”
The initial attack crew encountered fire coming from a vent at the ceiling level above the sales counter at the front of the building. The IC was never informed of the fire near the front of the building and was only aware of the fire on the mezzanine as pointed out to him by the property owner. Fire fighters provided information to the IC about the location of the fire and what they had accomplished during their attack after they had exited the structure.
Recommendation #2: Fire departments should ensure that fire fighters open concealed spaces to determine whether the fire is in these areas. 6, 7
Discussion: Fire fighters may have difficulty in finding the exact location or the extension of fire in a building, even though heavy smoke makes it clear that fire is present. When fire is present in a void or concealed space there may be little or no visible smoke. All fire fighters should look for, and act on, signs of fire or heavy smoke coming from the roof, or other distant locations. If the fire emerges behind the fire fighter, egress may be cut off, leading to the possibility of entrapment.
Recommendation #3: Fire departments should ensure that pre-emergency planning is completed for mercantile and business occupancies. 3, 8
Discussion: Pre-emergency planning, preplanning, and preincident planning are all terms that mean essentially the same thing. By first identifying target hazards within a department’s jurisdiction, the fire department can prioritize and begin to establish pre-emergency plans for those target hazards. Pre-emergency planning consists of a pre-emergency survey of the property, the development of information resources that would be useful during the event, and the development of procedures that would be used during an emergency. Pre-emergency planning can help in identifying: the age of the structure; structural integrity; type of roof structure and supports; type of interior support structures; type of building materials; building contents (fuel load); and, means of ingress and egress. The fire department can assign the first-due companies to complete the pre-emergency survey, allowing personnel to become familiar with the property.
Dunn states “commercial occupancies are more dangerous to personnel. A study from 1989 to 1993 revealed that 3.1 fire fighters died for every 100,000 residence occupancy fires, and 11.6 fire fighters died for every 100,000 non-residence fires. Fire fighters should know a commercial building fire in a store office or warehouse is more dangerous than one in a residence building.”
Inspections of the building had been completed by the fire department prior to the incident, however, no pre-emergency plans were ever developed.
Recommendation #4: Fire departments should ensure that a Rapid Intervention Team (RIT) is established and in position. 3, 6, 9
Discussion: A rapid intervention team (RIT) should respond to every major fire. The team should report to the officer in command and should remain at an area designated by the IC until an intervention is required to rescue a fire fighter. The RIT should have all the tools necessary to complete the job–e.g., a search rope, rescue rope, first-aid kit, and a resuscitator to use in case a fire fighter needs assistance. These teams can intervene quickly to rescue fire fighters who become disoriented, lost in smoke-filled environments, trapped by fire, involved in structural collapse, or run out of breathing air. A RIT should be established, in position and ready for deployment during the initial stages of an incident. A RIT was not established until the ventilation crew exited the roof, changed out their air bottles and became the RIT.
Recommendation #5: Fire departments should consider using a thermal imaging camera as a part of the interior size-up operation to aid in locating fires in concealed areas. 10
Discussion: Thermal imaging cameras are being used more frequently by the fire service. One function of the camera is to locate the fire or heat source. Infrared thermal cameras assist fire fighters in quickly getting crucial information about the location of the source (seat) of the fire from the exterior of the structure, so they can plan an effective and rapid response with the entire emergency team. Knowing the location of the most dangerous and hottest part of the fire may help fire fighters determine a safe approach and avoid structural damage in a building that might have otherwise been undetectable. Ceilings and floors that have become dangerously weakened by fire damage and are threatening to collapse may be spotted with a thermal imaging camera. The use of a thermal imaging camera may provide additional information the Incident Commander can use during the initial size-up. At the time of the incident the fire department did not have a thermal imaging camera (TIC).
Recommendation #6: Fire Departments should ensure that local citizens are provided with information on fire prevention and the need to report emergency situations as soon as possible to the proper authorities. 7, 11
Discussion: One of the simplest and most effective methods of achieving the goal of the preservation of life and property is prevention. The importance of citizens reporting an emergency situation, as soon as possible, to the proper authorities cannot be overemphasized. Any delay allows the fire a chance to increase in intensity and to spread to uninvolved areas. Brannigan states “make it clear that the fire department should be called if smoke is even smelled. This might indicate a hidden fire.” As stated in the fire fighter’s handbook “teaching our citizens to recognize life safety hazards and to react appropriately is clearly a fire department function and responsibility.” According to the Deputy State Fire Marshals’ report, the occupants of the building spent approximately 30 minutes attempting to locate the source of “a light haze in the air and the smell of something burning” and that the occupants had attempted to extinguish what was believed to be a fire in the bathroom area on the mezzanine before calling 911. The State Fire Marshal’s Office suspects that the fire had possibly started earlier that day when an incinerator was ignited to dispose of waste products.
Recommendation #7: Fire departments should ensure that self-contained breathing apparatus (SCBAs) and equipment are properly inspected, used, and maintained to ensure they function properly when needed. 12, 13
Discussion: It is rare for an SCBA respirator performance evaluation, in and of itself, to point to causes of a fatality. In this case, it was not possible to determine if the deficiencies discovered during the testing of the one unit involved in this incident (Appendix) existed prior to the victim’s death or were sustained subsequent to his death from fire or recovery efforts. NFPA 1404, Chapter 6-2.1, and OSHA 29CFR 1910(c)(1)(v) require a preventive maintenance program to be in place to prevent SCBA malfunction and equipment failure during use. NFPA 1404 contains general guidelines that all fire departments should follow to ensure that all in-service SCBAs are in good working order and will function properly when needed. An SCBA will only provide the highest level of protection when it is properly serviced and maintained. Both NFPA 1404, (Chapter 5-1.4) and the Occupational Safety and Health Administration (OSHA) Respirator Standard (29CFR 1910.134(h)(3)(i)(A) require the SCBA to be inspected prior to use. This inspection should include a functional check to ensure that the regulator, low-air alarm, bypass valve, and other features of the SCBA are working properly.
Recommendation #8: Fire departments should ensure that fire command always maintains close accountability for all personnel operating on the fireground. 14, 15
Discussion: Although there is no evidence that this recommendation would have prevented these fatalities, it is being provided as a reminder of a good safety practice. Accountability on the fireground is paramount and may be accomplished by several methods. It is the responsibility of all officers to account for every fire fighter assigned to their company and relay this information to IC. A fire fighter should communicate with the supervising officer by portable radio to ensure accountability and indicate completion of assignments and duties. One of the most important aids for accountability at a fire is the Incident Command System (ICS). As a fire escalates and additional fire companies respond, communication assists the IC with accounting for all fire fighter companies at the fire, at the staging area, and at rehabilitation. With an accountability system in place, the IC may readily identify the location of all fire fighters on the fireground. Additionally, the IC would be able to initiate rescue within minutes of realizing a fire fighter is trapped or missing.
Additionally,
Recommendation #9: Building owners should ensure that building permits are obtained and local building codes are followed when additions or modifications are made. 16, 17
Discussion: The NFPA Fire Protection Handbook states “throughout history there have been building regulations for preventing fire and restricting its spread. Over the years these regulations have evolved into the codes and standards developed by committees concerned with fire protection. The requirements contained in building codes are generally based upon the known properties of materials, the hazards presented by various occupancies, and the lessons learned from previous experiences, such as fire and natural disasters.”
The city reviewed building and mechanical permit records maintained by the city for the incident building, and relevant building and mechanical code requirements. No records were found for the chimney roof structure, believed to be the point of origin of the fire. The chimney was not installed per code requirements.
INVESTIGATOR INFORMATION
This incident was investigated by Mark McFall and Carolyn Guglielmo, Safety and Occupational Health Specialists, Tim Merinar, Safety Engineer, and Richard Braddee, Team Leader, Fire Fighter Fatality and Prevention Team, Trauma Investigations Section, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH.
Diagram 1. Aerial view of incident site
Diagram 2. Profile view from the south of the auto parts
store depicting the area of
origin, fire spread, and approximate locations of victims
Photo 1. North-East corner of mezzanine where attack crews were operating
Photo 2. View of east wall on mezzanine
Photo 3. View of sales counter where victim #3 was found
Photo 4. Aerial view of auto parts store
Status Investigation Report of Four
Self-Contained Breathing Apparatus
Oregon Fire Department
NIOSH Task No. TN-12789
August 11, 2003
National Personal Protective Technology
Laboratory
Respirator Branch
Quality Assurance Section
Disclaimer
Investigator Information
The SCBA inspections and performance tests were conducted by and this report was written by Vance Kochenderfer, Quality Assurance Specialist, Respirator Branch, National Personal Protective Technology Laboratory, National Institute for Occupational Safety and Health, located in Bruceton, Pennsylvania.
The purpose of Respirator Status Investigations is to determine the conformance of each respirator to the NIOSH approval requirements found in Title 42, Code of Federal Regulations, Part 84 (42 CFR 84). A number of performance tests are selected from the complete list of Part 84 requirements and each respirator is tested in its “as received” condition to determine its conformance to those performance requirements. Each respirator is also inspected to determine its conformance to the quality assurance documentation on file at NIOSH. In order to gain additional information about its overall performance, each respirator may also be subjected to other recognized test parameters, such as National Fire Protection Association (NFPA) consensus standards. While the test results give an indication of the respirator’s conformance to the NFPA approval requirements, NIOSH does not actively correlate the test results from its NFPA test equipment with those of certification organizations which list NFPA-compliant products. Thus, the NFPA test results are provided for information purposes only. Selected tests are conducted only after it has been determined that each respirator is in a condition that is safe to be pressurized, handled, and tested. Respirators whose condition has deteriorated to the point where the health and safety of NIOSH personnel and/or property is at risk will not be tested.
Status Investigation Report of Four
Self-Contained Breathing Apparatus
Submitted by the
Oregon Fire Department
NIOSH Task No. TN-12789
Background
As part of the National Institute for Occupational Safety and Health
(NIOSH) Fire Fighter Fatality Investigation and Prevention Program,
the Respirator Branch agreed to examine and evaluate four ISI 4500 psi, 30-minute,
self-contained breathing apparatus (SCBA). The Oregon Fire Department reported
that three of the SCBA were last used during interior firefighting operations
at a structure fire on November 25, 2002. The fourth, designated as Unit #4,
was not involved in that incident but a problem was reportedly experienced with
the low-air alarm whistle. This SCBA status investigation was assigned NIOSH
Task Number TN-12789. The Oregon Fire Department was advised that NIOSH would
provide a written report of the inspections and any applicable test results.
The SCBA, sealed in corrugated cardboard boxes, were delivered to the NIOSH
facility in Bruceton, Pennsylvania on January 27, 2003. Upon arrival, the sealed
packages were taken to the Firefighter SCBA Evaluation Lab (Building 108) and
stored under lock until the time of the evaluation.
SCBA Inspection
The first package from the Fire Department was opened, and the SCBA inspection
was initiated on July 9, 2003. Inspection of the four SCBA was concluded on
July 16, 2003. The SCBA were inspected by Vance Kochenderfer, Quality Assurance
Specialist, of the Respirator Branch, National Personal Protective Technology
Laboratory (NPPTL), NIOSH. The SCBA were examined, component by component, in
the condition as received to determine their conformance to the NIOSH-approved
configuration. The entire inspection process was videotaped. The SCBA were identified
as the ISI Magnum model.
Units #1 and #2 were severely damaged by exposure to heat, and neither SCBA
was in a condition suitable for testing. Unit #3 showed signs of normal wear
due to use and was very sooty. Other than some damage to the demand valve housing
and release latch, it appeared to be in good condition. Unit #4 was provided
without a facepiece and also showed evidence of use, but was overall in very
good condition.
SCBA Compressed Air Cylinder Contents
During the inspection, it was noted that the compressed air cylinder on Unit
#4 was partially pressurized. An air sample was collected from the cylinder
and forwarded to an accredited laboratory for analysis. The laboratory, Dräger
Lab Services, analyzed the sample in accordancewith the standards and methodologies
found in the Compressed Gas Association’s standard, ANSI/CGA G-7.1, Commodity
Specification for Air. The test report indicates that the sample met the
standard for Grade D air. In addition, the sample met OSHA’s moisture
content requirement (dewpoint below -50F) in 29 CFR 1910.134(i)(4)(iii). However,
it did not meet the more stringent guidelines published in NFPA 1500, Fire
Department Safety and Health Program, 2002 Edition. Section 7.9.1 of that
document specifies a moisture content of no more than 24 parts per million,
which corresponds to a dewpoint of approximately -65F.
SCBA Testing
The purpose of the testing was to determine the SCBA’s conformance to
the approval performance requirements of Title 42, Code of Federal Regulations,
Part 84 (42 CFR 84). Further testing was conducted to provide an indication
of the SCBA’s conformance to the National Fire Protection Association
(NFPA) Air Flow Performance requirements of NFPA 1981, Standard on Open-Circuit
Self-Contained Breathing Apparatus for the Fire Service, 1997 Edition.
Although the SCBA were certified to the 1987 edition of this standard, the Air
Flow Performance Test specified in the 1997 edition is identical to the one
in that earlier revision.
The following performance tests were conducted on the SCBA:
NIOSH SCBA Certification Tests (in accordance with the performance requirements of 42 CFR 84):1. Positive Pressure Test [§ 84.70(a)(2)(ii)]; 2. Rated Service Time Test (duration) [§ 84.95]; 3. Gas Flow Test [§ 84.93]; 4. Exhalation Breathing Resistance Test [§ 84.91(c)]; 5. Static Facepiece Pressure Test [§ 84.91(d)]; 6. Remaining Service Life Indicator Test (low-air alarm) [§ 84.83(f)]
National Fire Protection Association (NFPA) Tests (in accordance with NFPA 1981, 1997 Edition): 7. Air Flow Performance Test [Chapter 6, 6-1] Testing of Unit #3 was initiated on July 15, 2003. Five performance tests were completed that day. The Exhalation Breathing Resistance Test and Static Facepiece Pressure Test were conducted on July 17, 2003. Testing of Unit #4 was initiated on July 17, 2003. All six performance tests were completed that day using the facepiece supplied with Unit #3. The Exhalation Breathing Resistance Test was not performed on this unit. In this model SCBA, the exhalation resistance is mainly influenced by the facepiece and it was judged that using a substitute facepiece with the unit would not provide a useful result. It was noted during testing that the low-air alarm whistle on Unit #4 sounded fainter than normal. Therefore, it was additionally subjected to the Alarm Sound Level Test on August 11, 2003. All testing was videotaped with the exception of the Exhalation Breathing Resistance Test, Static Facepiece Pressure Test, and Alarm Sound Level Test. Unit #3 met the requirements of all tests except the Remaining Service Life Indicator Test and NFPA Air Flow Performance Test. The low-air alarm whistle did not activate at any time during testing. As both of those tests require the proper function of the alarm, the SCBA was unable to successfully complete them. Unit #4 did not meet the requirements of the Remaining Service Life Indicator Test. The low-air alarm whistle activated at a higher pressure than that allowed by the requirement. This would result in the user having an earlier-than-normal warning of cylinder exhaustion. In addition, the whistle was not loud enough to meet the requirement of the Alarm Sound Level Test. The SCBA successfully passed all other testing.
Summary and Conclusions
Four SCBA were submitted to NIOSH by the Oregon Fire Department for evaluation.
The SCBA were delivered to NIOSH on January 27, 2003. The SCBA were inspected
between July 9 and July 16, 2003. The four units were identified as ISI Magnum
30-minute, 4500 psi, SCBA (NIOSH approval number TC-13F-236). All except for
Unit #2 were labeled as compliant to the 1987 edition of NFPA 1981. While Units
#1 and #2 were too heavily damaged, it was determined that Units #3 and #4 could
be safely pressurized and tested. Units #3 and #4 were each subjected to seven
performance tests. As no facepiece was provided with Unit #4, the one supplied
with Unit #3 was substituted for testing. Testing began on July 15, 2003, and
was completed on July 17, 2003. The low-air alarm whistle of Unit #3 was not
functional, causing the SCBA to fail the Remaining Service Life Indicator Test
and NFPA Air Flow Performance Test. The low-air alarm whistle of Unit #4 was
out of adjustment, causing it to fail the Remaining Service Life Indicator Test.
It also failed the Alarm Sound Level Test. No maintenance or repair work was
performed on the SCBA at any time.
In light of the information obtained during inspection and testing, the Institute
recommends that additional investigation be performed into the problems noted
with the low-air alarm whistles. Should the Oregon Fire Department consent,
NIOSH will conduct a more detailed examination of this issue. Following inspection
and testing, the SCBA were returned to the packages in which they were received
and stored under lock in Building 108 at the NIOSH facility in Bruceton, Pennsylvania,
and secured there pending further action or return to the Oregon Fire Department.
It is doubtful that either Unit #1 or Unit #2 could be practically repaired and returned to service. If the other SCBA are to be placed back in service, they must be repaired, inspected, and tested by a qualified service technician, paying particular attention to the low-air alarm whistles.

Return to Fire Fighter Homepage
![]()
This page was last updated on 09/26/03