
Global Health E-Brief
WELCOME to the third quarter Global Health E-Brief, designed to inform readers about key global health activities at the Centers for Disease Control and Prevention (CDC). Our third issue for 2008 highlights how CDC has responded to global public health emergencies. Whether natural disasters such as cyclones or earthquakes; deadly, recurrent disease outbreaks; or man-made emergencies arising from political unrest, CDC is committed to working with Ministries of Health and other partners to assess and respond to public health needs resulting from these critical events.
IN THIS ISSUE- CDC Perseveres to Assess Public Health Needs After Cyclone Nargis
- Public Health Work Continued in Kenya Despite Post-election Violence
- CDC Foundation Donation of Mobile Technology Devices Helps Fight Disease in Earthquake-torn China
- CDC Experts Work with Uganda Ministries of Health and Tourism to Protect Tourists from Deadly Marburg Virus
- CDC and Partners Educate Kenyans about Simple Intervention to Ease Disruptive Cholera Outbreaks
CDC Perseveres to Assess Public Health Needs After Cyclone Nargis

Focus group conducting surveys to
identify needs in special populations.
Nargis, a category 3 cyclone, made landfall May 2, 2008, on the southern edge of Burma (also known as Myanmar). Two months later, the official death toll was 84,537, another 53,836 people were still missing, and 800,000 people were displaced.
The worst natural disaster in the history of Burma, Cyclone Nargis was the most devastating cyclone to strike Asia since 1991. Nargis swept across the country with wind speeds of up to 200 kilometers per hour and heavy rain. When the storm subsided, there was near-total destruction of fields and shelter in the areas of direct impact.
In response to this global emergency, the United Nations (UN) deployed staff to the capital city of Yangon to provide informatics assistance and coordinate information for humanitarian response through the establishment of a Humanitarian Information Center (HIC). The Union of Burma, the UN, and the Association of Southeast Asian Nations (ASEAN) joined forces to coordinate relief activities. One of their first critical activities was to develop a joint assessment to analyze the extent of destruction and determine key recovery and humanitarian needs.
CDC joined the relief efforts at the request of the Information Management and Mine Action Programs (iMMAP), a U.S.-based organization that works on the effective use of information management practices and principles in the service of humanitarian relief and development. iMMAP and CDC have a long history of setting up HICs around the world. CDC and iMMAP staff, including CDC informatics expert Carl Kinkade, were deployed to the UN to work on the assessment in Yangon.
To rapidly assess the humanitarian needs of the extraordinarily large affected area—around 17,000 square miles—relief workers had to consider logistics, staffing, coordination and methodology.
Kinkade helped survey individual households, teachers and representatives of special populations in the worst—affected townships. The survey included questions on health, food and nutrition, education, women and children, water and sanitation, agriculture, livelihood, temporary settlements, and emergency shelter. He and his colleagues collectively visited 291 villages, across 30 townships, gathering almost 5,000 paper surveys over 10 days in June.
The logistics were one of the biggest challenges, according to Kinkade. “When you try to survey villages that have been flooded or have no roads to get to them, it requires hours on small boats, walking, or helicopter to get the enumerators to the villages.”
”Then we had to bring 5,000 surveys back to Yangon to be analyzed.”
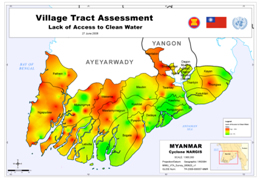
CDC provided analysis of the collected
data to identify areas of greatest need.
Despite the challenges of rapidly completing an assessment of that magnitude, the data documented the devastation and the needs of people in affected villages. The devastation included entire villages leveled by the 12 foot storm surge, contaminated drinking water from ponds due to salination from the surge, dead livestock, and rice fields flooded with salt water. Public health issues that the Burma health system will need to be alert to for some time include stress, malnutrition from poor diets, and potential outbreaks of diarrhea because of poor sanitary conditions.
The data also help the humanitarian community make the case for responding to similar disasters in the future by showing the potential for continued suffering if the response is not effective.
A unique challenge to CDC′s participation in the response is the current state of the US Government′s relationship with Burma, according to Mike Gerber, CDC′s lead for international emergency and refugee health. Due to Burma′s military leadership, visas were hard to obtain, especially for US government agencies.
“Because the US Government does not have diplomatic relations with Burma, CDC could not offer its typical support for this effort,” Gerber said. “Even so, through Carl Kinkade′s efforts as part of an international team, CDC made a substantial contribution to the rapid collection of information needed for effective emergency response.”
The next phase of the assessment is evaluation and monitoring of the humanitarian effort to inform leaders of the relief efforts in progress. CDC continues to provide support through iMMAP to help the UN and Burma response to the current and ongoing health needs of Cyclone Nargis survivors.
Public Health Work Continued in Kenya Despite Post-election Violence

Tony Langat, a pharmacist with
KEMRI-CDC, speaks to a patient.
More than 1,000 people were killed and another 300,000 displaced as a result of violent protests when members of rival political parties contested the Kenyan presidential election in December 2007. During the following two months, CDC offices in Nairobi (including clinics in the Kibera informal settlement) and rural Kenya were closed periodically because of concerns for staff safety. Despite the upheaval, the public health work being done at CDC Kenya and its partner institution, the Kenya Medical Research Institute (KEMRI), continued throughout this chaotic period in Kenya.
As others fled the violent regions, several heroic KEMRI/CDC staff reported to work to provide the critical care and treatment on which so many Kenyans rely. When the violence began, Mary Agola, a nurse with KEMRI-CDC was at Lwak Mission Hospital in rural Kenya. Many of her colleagues had returned to their home districts to vote and could not return because of the violence. Realizing that hospital operations would stop if they left, Agola and other staff stayed. During the next two weeks, she and other KEMRI-CDC staff including health recorders Mary Pacho, Kennedy Jaramba, Judith Ongaro, and George Odhiambo; lab technologists Nicholas Omondi and Christine Awuor; and clinical officer Harun Chilaho, cared for the regular flow of people sick with malaria, pneumonia and HIV, in addition to the surge of patients injured during the post-election violence. In addition to the KEMRI-CDC clinical team, community workers also continued to visit households in the surveillance areas to collect data on health status.
Agola and the other KEMRI-CDC staff had the support of the community—which even staged mock demonstrations to keep troublemakers away—to keep the hospital running. “It′s true we were frightened, but we felt a responsibility to our work as well as to the people who were affected by the violence,” Agola said. “Other hospitals had closed and people were coming long distances for help.” Staff replacements began arriving the week of January 7, but the KEMRI-CDC staff continued working until January 20th to be sure that people who needed care received it. As a result, the Lwak Hospital never closed its doors. KEMRI-CDC staff helped the community in other ways as well. The Kisumu Field Station in rural Kenya held a blood drive on January 11 and collected 32 pints of blood for use in community hospitals. In addition, the KEMRI-CDC collaboration joined Red Cross International and other partners in Nyanza Province to provide medical care. Through temporary medical camps, they provided drugs, medical care, psychosocial support, nutrition support, voluntary counseling and testing for HIV, food, and legal support. On February 2, more than 1,000 people attended one such camp.
KEMRI-CDC staff also distributed malaria treatment and bednets, and several staff attended “alternatives to violence” workshops to discuss ways to bring peace to their own lives and to their communities. This violent episode illustrates how non-health issues, such as an election, can have a significant negative impact on the public health infrastructure of a country. CDC′s response shows the agency′s broad public health expertise that can be mobilized against violence and injury prevention as well as infectious diseases. In addition, the response shows CDC′s global reach is intentionally nimble to provide assistance in response to changing environments and public health needs.
Today, the violence has subsided, but disruptions in food supply, immunizations, medications, and health services are expected to affect Kenyans′ health for some time. Looking forward, KEMRI-CDC will evaluate the public health impact of the post-election violence and respond to what may become lasting impacts on public health in Kenya.
CDC Foundation Donation of Mobile Technology Devices Helps Fight Disease in Earthquake-torn China

CDC′s Dr. Ramesh Krishamurthy and Dr. Yu Wang,
director of CDC China discuss the use of handheld
computers to restore health surveillance activities
following the earthquake.
Six CDC scientists were scheduled to leave for China in just two days. Officials from China′s CDC were reporting that public health facilities in Sichuan province had been demolished by the May 2008 earthquake and that they had very limited capacity to assess the region′s health needs or monitor for potential disease outbreaks. The U.S. CDC experts were planning to work with their counterparts at China′s CDC to rapidly get a health surveillance system up and running by using mobile technology for data collection.
Using mobile technology for surveillance is still an emerging idea in public health, and neither U.S. CDC nor China CDC had enough handheld computers to get the job done. Even if the U.S. team could work through the necessary government process to obtain the handheld PDA units they needed, they did not know how they would get them to China quickly enough through diplomatic channels. So, CDC asked the CDC Foundation for help.
The Foundation was ready to use funds from its Global Disaster Response Fund to help purchase the handheld units, but first reached out to partner organizations to see if the units might be secured through an in-kind gift. The Foundation immediately contacted corporate leaders at HP. HP had previously donated equipment to CDC through the Foundation to meet needs following the 2004 tsunami that devastated Southeast Asia. HP leaders quickly agreed to donate 500 HP iPAQ Travel Companions with GPS technology, valued at approximately $300,000, and ship them directly to China CDC in Beijing. The units arrived within one week of the U.S. CDC team, so they were able to begin helping Chinese scientists re-establish a health surveillance network almost immediately.
“HP and its employees have a long history of helping those in need,” said Isaiah Cheung, vice president and general manager, Personal Systems Group, HP China and Hong Kong. “The public health surveillance system, supported by HP iPAQ GPS travel companions, will go a long way toward preventing Sichuan earthquake survivors from suffering additional pain due to disease.”
Microsoft also donated handheld mobile devices directly to CDC China, and, working with the CDC Foundation, USGlobalSat, Inc., a subsidiary of GPS manufacturer GlobalSat Technology of Taiwan, provided wireless Bluetooth GPS receivers to ensure that the devices donated by Microsoft had the GPS capabilities health teams required.
Says Leslie A. Lenert, M.D., M.S., director of CDC′s National Center for Public Health Informatics, “With the new system we helped them design, and with equipment donations organized by the CDC Foundation, China CDC now is able to quickly collect public health data in earthquake-affected areas where communications capacity has been destroyed and send it to China CDC headquarters for analysis. This allows China CDC to rapidly get the right resources to the right places to save lives by preventing or reducing disease and injury.”
As efforts in China have shifted from emergency response to recovery, the health and well-being of an estimated 5 million displaced persons and the rebuilding of health system infrastructure have become chief concerns. Mobile technology with geographic information systems (GIS), like the handheld units donated by HP and the components donated by USGlobalSat, Inc., can be used to collect data, map locations of clinics and shelters and transmit critical information for rapid analysis. CDC will continue to provide technical assistance and expertise as China works to prevent disease outbreaks and rebuild the public health system in Sichuan province.
(This article was originally published in The Frontline Newsletter, Fall 2008, by the CDC Foundation: http://www.cdcfoundation.org/frontline/2008/)
CDC Experts Work with Uganda Ministries of Health and Tourism to Protect Tourists from Deadly Marburg Virus
the Uganda Public Health
and tourism authorities in
developing materials to
educate Ugandans and
others about safe travel.
In July 2008, a Dutch tourist died of Marburg viral hemorrhagic fever following her return to the Netherlands from a vacation in Uganda. Marburg is a very rare but severe type of hemorrhagic fever caused by a virus similar to the group of Ebola viruses. During the trip, the Dutch tourist visited a cave near Queen Elizabeth National Park located in the western part of the country. After the diagnosis was confirmed, public health authorities in the Netherlands immediately notified others with whom she may have had contact. Fortunately, no one else was infected.
Recognizing that other tourists could be at risk from similar exposures during visits to their country, the Uganda Ministry of Health requested assistance from CDC to help respond to the potential public health emergency. In early August, CDC sent a three person team to work with the Uganda Ministry of Health, the Uganda Wildlife Authority (UWA), and the Association of Uganda Tour Operators. Together, the group quickly created and distributed messages about safe and healthy travel to Uganda. The activities included:
- Reaching out to Uganda and US-based African tour operators to describe the risks associated with exposure to bats and recommending that travelers not enter caves or other bat habitats;
- Developing printed products, created by the CDC team with guidance and approval from the Ugandan public health and tourism authorities, for specific audiences:
- A ‘Safe and Healthy Travel in Uganda′ brochure for distribution to international travelers. The brochure provides guidance on preventing disease during travel, as well as pre- and post-travel recommendations for travelers.
- An ‘Ebola and Marburg Hemorrhagic Fevers′ brochure and a companion poster to educate residents and health providers in at-risk areas about precautions to prevent the two diseases and symptoms to watch for in the event of an exposure.
- Posting a Travelers Health Notice on the CDC web site recommending that tourists and other visitors not enter caves or mines inhabited by bats.
To further investigate the ecology of Marburg virus in bats in Uganda, CDC sent a second team to collect and test bats from the cave for the Marburg virus. Tissue samples from the bats were initially examined at the Uganda Virus Research Institute in Entebbe. Additional analysis at CDC headquarters in Atlanta is expected to result in more information about the characteristics of the virus and lead to further public health recommendations to protect the public.
This collaboration between CDC, the Ugandan Ministry of Health, Ugandan Wildlife Authority, and the tourism industry effectively used scientific inquiry to create messages to protect public health and prevent a potential public health crisis. The products created during the response—the first such collaboration by Uganda′s public health and tourism agencies—featured consistent messages to protect both the public′s health and the tourism industry that makes important contributions to Uganda′s economy.
The success of this collaboration is attributable to CDC′s technical expertise and the willingness of Ugandan authorities, both public and private, to work together. The materials will be distributed broadly and authorities also plan to develop surveys to gather additional data from international travelers to Uganda, the Uganda Wildlife Authority staff, and the tourism industry about how to promote safe, healthy travel.
CDC and Partners Educate Kenyans about Simple Intervention to Ease Disruptive Cholera Outbreaks
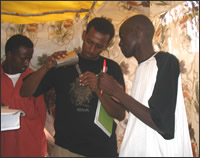
Teddy Malachi (right) and Jamal Ahmed (center)
testing water during a response to a cholera
outbreak at Dadaab Refugee Camp in Kenya.
Teddy Malachi, CDC′s foot soldier in the battle against cholera in Nyanza Province, Kenya, has been busy lately. Seven times since March of this year he has traveled to rural villages or semi-urban slums to respond to outbreaks. In hospitals, clinics, schools, and at community meetings, Malachi has worked with local partners to give people the tools to protect themselves from cholera, an ancient disease that can cause explosive, potentially lethal epidemics of diarrhea.
The tools are simple—disinfectant solution to kill cholera-causing germs in drinking water stored in the home, soap for washing hands, and counseling techniques to motivate people to use these products to prevent cholera and other waterborne diseases.
Cholera is a disease that has defied efforts to keep it under control, and remains a serious problem throughout many parts of the world. From 1995 to 2005, there have been over 632 reported cholera outbreaks and 19,600 deaths related to those 632 reports. In 2008 alone, there have been numerous outbreaks: 1,200 infected and 60 dead in Kenya, 13 dead in Zimbabwe, 90 infected in Benin, 35 dead in Nigeria, 36 infected and 5 dead in Iraq. A large, on-going outbreak in Guinea-Bissau, to which CDC recently responded, jointly with the Brazilian Ministry of Health, has infected approximately 9,800 people (as of Oct. 6) and claimed 178 lives.
While some countries have experienced long-lasting endemic cholera, a series of countries and sub-regions are regularly affected by disruptive outbreaks. Cholera has been particularly devastating in Africa, with 95% of cholera cases and 98% of cholera deaths occurring in sub-Saharan Africa.
Cholera is a disease of poverty. It has persisted in sub-Saharan Africa because of lack of access to piped, treated water and sewage treatment systems. It is likely exacerbated by widespread malnutrition in that part of the world. Unfortunately, the obvious solution of building necessary water and sewage infrastructure will likely take billions of dollars and decades to achieve. The question is, in the meantime, what can be done to save lives and protect people′s health now.
CDC′s answer is development of simple, inexpensive, household interventions that are implemented locally. One such intervention is the Safe Water System (SWS), a water treatment technique that uses locally-produced bleach solution, safe water storage to prevent recontamination, and behavior change techniques - components that make the system effective, sustainable, and scalable. To learn more about SWS, please see CDC′s second quarter 2007 e-brief (http://www.cdc.gov/washington/EGlobalHealthEditions/2007_q2_ebrief.pdf). CDC also conducts public health research to understand the most effective hand-washing techniques and the most effective ways to motivate behavior change.
When a SWS project is put in place, the response to cholera is simplified. Local health authorities and other partners can deliver an inexpensive, locally-available, and culturally familiar product to the site of the cholera outbreak and then develop communications campaigns to encourage the desired behavior change. In 2007 alone, Population Services International (PSI), a CDC partner, used the tools of the SWS to respond to cholera outbreaks in 14 countries. Malachi, who works with the Safe Water and AIDS Project, a Kenyan non-governmental organization that works closely with PSI, has himself responded to 14 outbreaks in Kenya in 2007 and 2008.
Solving the cholera problem will take more time and effort, but with a simple approach, and dedicated partners like PSI and individuals like Malachi, CDC is doing its part to respond to these disruptive, recurrent outbreaks and provide the tools for a healthier world.
News Bytes...News Bytes...News Bytes...News Bytes...News Bytes...News Bytes...News Bytes...
CDC identifies new arenavirus as cause of unusual cases of acute febrile syndrome in Africa
The results of tests conducted at CDC in Atlanta and at the National Institute for Communicable Diseases (NICD) of the National Health Laboratory Service in Johannesburg, South Africa, provide preliminary evidence that the causative agent of the disease which has resulted in the recent deaths of 4 people in hospitals in Johannesburg, has been preliminarily identified as an Old World arenavirus related to the Lassa fever virus of West Africa. Arenaviruses cause chronic infection in wild rodents (multimammate mice) with excretion of virus in urine, which can contaminate human food or house dust.
Within three weeks of the first reports, the new arenavirus was identified by immunohistochemical tests performed at CDC in Atlanta on autopsy liver and skin samples taken with biopsy needles and skin punches in the Special Pathogens Unit of the National Institute for Communicable Diseases, South Africa.
Other tests further confirm that the infections were caused by a virus which is different from lymphocytic choriomeningitis virus (LCMV), Lassa fever virus (LASV), and other known Old World arenaviruses. Successful isolation of the causative agent means that more detailed characterization, including full genome sequencing and electron microscopy, can now take place.
This outbreak represents a cluster of cases confined to individuals with very close contact in a health-care setting. Monitoring of contacts, active case finding and investigation and management of suspected cases will continue as needed. Collection of additional clinical, epidemiological and laboratory data is ongoing and data will be updated accordingly.
CDC, the NICD, and the World Health Organization continue to monitor persons who had close contact with persons who became ill for new cases. Analysis continues at the NICD and CDC in order to characterize this virus more fully. CDC and NICD are technical partners in the Global Outbreak Alert and Response Network (GOARN), a technical collaboration based at the World Health Organization.
CDC – Thailand Collaborates with Regional Partners to Convene Expert Forum on Hand, Foot, and Mouth Disease in the Asia-Pacific Region
Hand, foot, and mouth disease (HFMD) is usually a mild illness, most frequently reported in young children. HFMD can be caused by a number of different enteroviruses. Over the past decade, however, HFMD caused by enterovirus (EV) 71 has caused large outbreaks associated with a disproportionately high percentage of severe and fatal HFMD cases in the Asia-Pacific region. During 2008 alone, HFMD outbreaks linked to EV71 affected tens of thousands of children, with more than 45 reported deaths in China, Taiwan, Singapore, Malaysia, and Thailand.
In response to these recent outbreaks, CDC emerging infectious disease experts in Thailand collaborated with regional partners, including the Regional Emerging Diseases Intervention (REDI) Centre and the Singapore Ministry of Health, to convene a meeting of experts in HFMD and EV71. The late August meeting enabled scientists to share and compare experiences, review the state of knowledge regarding the diagnosis, causes, treatment, control, and prevention of the disease, and identify priority areas around which future collaborative research and intervention project could be conducted to strengthen prevention, control, and management of HFMD. The forum brought together CDC scientists and approximately 80 scientific experts from several countries in the region, including Australia, Burma, Brunei, Indonesia, Malaysia ,People′s Republic of China, Singapore, Thailand, and Vietnam. Meeting proceedings and recommendations are currently being compiled and will be available later this year. Additional publications summarizing scientific data and presentations from the forum are also planned.

Content Management: Office of Enterprise Communication
Page last modified: October 30, 2008
