2001 Surgeon General's Report—Women and Smoking
At A Glance
Disclaimer
The Burden:
This year alone, lung cancer will kill nearly 68,000 U.S. women. That’s
one in every four cancer deaths among women, and about 27,000 more deaths
than from breast cancer (41,000). In 1999, approximately 165,000 women died
prematurely from smoking-related diseases, like cancer and heart disease.
Women also face unique health effects from smoking such as problems related
to pregnancy.
The Trends:
In the 1990s, the decline in smoking rates among adult women stalled
and, at the same time, rates were rising steeply among teenaged girls, blunting
earlier progress. Smoking rates among women with less than a high school
education are three times higher than for college graduates. Nearly all
women who smoke started as teenagers—and 30% of high school senior
girls are still current smokers.
The Hope:
We have the solutions for preventing and reducing smoking among women.
Quitting smoking has great health benefits for women of all ages. Thanks
to an aggressive, sustained anti-smoking program, California has seen a
decline in women’s lung cancer rates while they are still rising in the
rest of the country. The voice of women is needed to counter tobacco marketing
campaigns that equate success for women with smoking.
" When calling attention to public
health problems, we must not misuse the word ‘epidemic.’ But there is no
better word to describe the 600–percent increase since 1950 in women’s death
rates for lung cancer, a disease primarily caused by cigarette smoking.
Clearly, smoking-related disease among women is a full-blown epidemic."
David Satcher, M.D., Ph.D.
Surgeon General
Women and Smoking: a Report
of the Surgeon General makes its overarching theme clear-smoking is
a woman’s issue. This report summarizes what is now known about smoking
among women, including patterns and trends in smoking habits, factors associated
with starting to smoke and continuing to smoke, the consequences of smoking
on women’s health and interventions for cessation and prevention. What the
report also makes apparent is how the tobacco industry has historically
and contemporarily created marketing specifically targeted at women. Smoking
is the leading known cause of preventable death and disease among women.
In 2000, far more women died of lung cancer than of breast cancer. A number
of things need to be acted on to curb the epidemic of smoking and smoking-related
diseases among women in the United States and throughout the world.
- Increase awareness of the impact of smoking on women’s health and
counter the tobacco industry’s targeting of women.
- Support women’s anti-tobacco advocacy efforts and publicize that
most women are nonsmokers.
- Continue to build the science base for understanding the health
effects of smoking on women in particular.
- Act now: more than enough is already known to enable us to support
efforts to stop smoking at both individual and societal levels.
- Do everything possible to stop the epidemic
of smoking and smoking-related diseases among women globally.
Major Conclusions
of the Surgeon General’s Report
- Despite all that is known of the devastating health consequences
of smoking, 22.0% of women smoked cigarettes in 1998. Cigarette
smoking became prevalent among men before women, and smoking prevalence
in the United States has always been lower among women than among men.
However, the once-wide gender gap in smoking prevalence narrowed until
the mid-1980s and has since remained fairly constant. Smoking prevalence
today is nearly three times higher among women who have only 9 to 11
years of education (32.9%) than among women with 16 or more years
of education (11.2%).
- In 2000, 29.7% of high school senior girls reported having
smoked within the past 30 days. Smoking prevalence among white girls
declined from the mid-1970s to the early 1980s, followed by a decade
of little change. Smoking prevalence then increased markedly in the
early 1990s, and declined somewhat in the late 1990s. The increase dampened
much of the earlier progress. Among black girls, smoking prevalence
declined substantially from the mid-1970s to the early 1990s, followed
by some increases until the mid-1990s. Data on long-term trends in smoking
prevalence among high school seniors of other racial or ethnic groups
are not available.
- Since 1980, approximately 3 million U.S. women have died prematurely
from smoking related neoplastic, cardiovascular, respiratory, and pediatric
diseases, as well as cigarette-caused burns. Each year during the 1990s,
U.S. women lost an estimated 2.1 million years of life due to these
smoking attributable premature deaths. Additionally, women who smoke
experience gender-specific health consequences, including increased
risk of various adverse reproductive outcomes.
- Lung cancer is now the leading cause of cancer death among U.S.
women; it surpassed breast cancer in 1987. About 90% of all lung
cancer deaths among women who continue to smoke are attributable to
smoking.
- Exposure to environmental tobacco smoke is a cause of lung cancer
and coronary heart disease among women who are lifetime nonsmokers.
Infants born to women exposed to environmental tobacco smoke during
pregnancy have a small decrement in birth weight and a slightly increased
risk of intrauterine growth retardation compared to infants of nonexposed
women.
- Women who stop smoking greatly reduce their risk of dying prematurely,
and quitting smoking is beneficial at all ages. Although some clinical
intervention studies suggest that women may have more difficulty quitting
smoking than men, national survey data show that women are quitting
at rates similar to or even higher than those for men. Prevention and
cessation interventions are generally of similar effectiveness for women
and men and, to date, few gender differences in factors related to smoking
initiation and successful quitting have been identified.
- Smoking during pregnancy remains a major public health problem despite
increased knowledge of the adverse health effects of smoking during
pregnancy. Although the prevalence of smoking during pregnancy has declined
steadily in recent years, substantial numbers of pregnant women continue
to smoke, and only about one-third of women who stop smoking during
pregnancy are still abstinent one year after the delivery.
- Tobacco industry marketing is a factor influencing susceptibility
to and initiation of smoking among girls, in the United States and overseas.
Myriad examples of tobacco ads and promotions targeted to women indicate
that such marketing is dominated by themes of social desirability and
independence. These themes are conveyed through ads featuring slim,
attractive, athletic models, images very much at odds with the serious
health consequences experienced by so many women who smoke.
Prevalence of current smoking among women aged 18 years or older, all
women, by education (1998), and by race/ethnicity (1997–1998), United States.
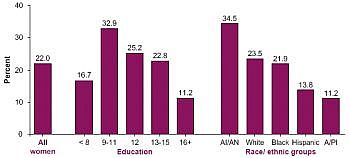
Source: National Health Interview Survey, 1998.Source:
National Health Interview Survey, 1997–1998.
Age-adjusted death rates for lung cancer and breast cancer among women,
United States, 1930–1997
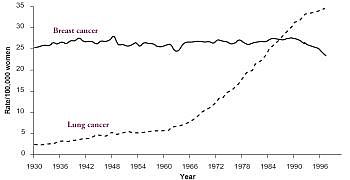
Note: Death rates are age–adjusted to the 1970 population.
Sources: Parker et al. 1996; National Center for Health Statistics 1999;
Ries et al. 2000; American Cancer
Society, unpublished data.
Patterns of Tobacco
Use Among Women and Girls
- The prevalence of current smoking among women was 22% in
1998. Smoking prevalence was highest among American Indian or Alaska
Native women, intermediate among white women and black women, and lowest
among Hispanic women and Asian or Pacific Islander women. By educational
level, smoking prevalence is nearly three times higher among women with
9 to 11 years of education than among women with 16 or more years of
education.
- Much of the progress in reducing smoking prevalence among girls
in the 1970s and 1980s was lost with the increase in prevalence in the
1990s: current smoking among high school senior girls was the same in
2000 as in 1988. Although smoking prevalence was higher among high school
senior girls than among high school senior boys in the 1970s and early
1980s, prevalence has been comparable since the mid–1980s.
- Smoking declined substantially among black girls from the mid–1970s
through the early 1990s; the decline among white girls for this same
period was small.
- Smoking during pregnancy appears to have decreased from 1989 through
1998. Despite increased knowledge of the adverse health effects of smoking
during pregnancy, estimates of women smoking during pregnancy range
from 12.9% to as high as 22%.
- Since the late 1970s or early 1980s, women are just as likely to
attempt to quit and succeed as are men.
- Smoking prevalence among women varies markedly across countries;
it is as low as an estimated 7% in developing countries to 24
percent in developed countries. Thwarting further increases in tobacco
use among women is one of the greatest disease prevention opportunities
in the world today.
Health Consequences
of Tobacco Use Among Women
- A woman’s annual risk for death more than doubles among continuing
smokers compared with persons who have never smoked in all age groups
from 45 through 74 years.
- The risk for lung cancer increases with quantity, duration, and
intensity of smoking. The risk for dying of lung cancer is 20 times
higher among women who smoke two or more packs of cigarettes per day
than among women who do not smoke.
- Smoking is a major cause of cancers of the oropharynx and bladder
among women. Evidence is also strong that women who smoke have increased
risks for liver, colorectal, and cervical cancer, and cancers of the
pancreas and kidney. For cancers of the larynx and esophagus, evidence
among women is more limited but consistent with large increases in risk.
- Smoking is a major cause of coronary heart disease among women.
Risk increases with the number of cigarettes smoked and the duration
of smoking. Risk is substantially reduced within 1 or 2 years of smoking
cessation. This immediate benefit is followed by a more gradual reduction
in risk to that among nonsmokers by 10 to 15 or more years after cessation.
- Women who smoke have an increased risk for stroke and subarachnoid
hemorrhage. The increased risk for stroke associated with smoking is
reversible after smoking cessation; after 5 to 15 years of abstinence,
the risk approaches that of women who have never smoked.
- Women who smoke have an increased risk for death from ruptured abdominal
aortic aneurysm. They also have risk for peripheral vascular atherosclerosis,
but cessation is associated with improvements in symptoms, prognosis,
and survival. Smoking is also a strong predictor of the progression
and severity of carotid atherosclerosis among women, but smoking cessation
appears to slow the rate of progression.
- Cigarette smoking is a primary cause of chronic obstructive pulmonary
disease (COPD) among women, and the risk increases with the amount and
duration of smoking. Approximately 90% of deaths from COPD among
women in the United States can be attributed to cigarette smoking.
- Adolescent girls who smoke have reduced rates of lung growth, and
adult women who smoke experience a premature decline of lung function.
- Women who smoke have increased risks for conception delay and for
both primary and secondary infertility and may have a modest increase
in risks for ectopic pregnancy and spontaneous abortion. They are younger
at natural menopause than non–smokers and may experience more menopausal
symptoms.
- Women who quit smoking before or during pregnancy reduce the risk
for adverse reproductive outcomes, including conception delay, infertility,
preterm premature rupture of membranes, preterm delivery, and low birth
weight.
- Postmenopausal women who currently smoke have lower bone density
than do women who do not smoke. Also women who currently smoke have
an increased risk for hip fracture compared with nonsmoking women.
- The association of smoking and depression is particularly important
among women because they are more likely to be diagnosed with depression
than are men.
- Exposure to environmental tobacco smoke is a cause of lung cancer
among women who have never smoked and is associated with increased coronary
heart disease risk.
Factors Influencing
Tobacco Use Among Women
- Girls who initiate smoking are more likely than those who do not
smoke to have parents or friends who smoke. They also tend to have weaker
attachments to parents and family and stronger attachments to peers
and friends. They perceive smoking prevalence to be higher than it actually
is, are inclined to risk taking and rebelliousness, have a weaker commitment
to school or religion, have less knowledge of the adverse consequences
of smoking and the addictiveness of nicotine, believe that smoking can
control weight and negative moods, and have a positive image of smokers.
- Women who continue to smoke and those who fail at attempts to stop
smoking tend to have lower education and employment levels than do women
who quit smoking. They also tend to be more addicted to cigarettes,
as evidenced by the smoking of a higher number of cigarettes per day,
to be cognitively less ready to stop smoking, to have less social support
for stopping, and to be less confident in resisting temptations to smoke.
- Women have been extensively targeted in tobacco marketing, and tobacco
companies have produced brands specifically for women, both in the United
States and overseas. Myriad examples of tobacco ads and promotions targeted
to women indicated that such marketing is dominated by themes of both
social desirability and independence, which are conveyed through ads
featuring slim, attractive, athletic models. Between 1995 and 1998,
expenditures for domestic cigarette advertising and promotion increased
from $4.90 billion to $6.73 billion. Tobacco industry marketing, including
product design, advertising, and promotional activities, is a factor
influencing susceptibility to and initiation of smoking.
- The dependence of the media on revenues from tobacco advertising
oriented to women, coupled with tobacco company sponsorship of women’s
fashions and of artistic, athletic, political, and other events, has
tended to stifle media coverage of the health consequences of smoking
among women and to mute criticism of the tobacco industry by women public
figures.
Efforts to Reduce
Tobacco Use Among Women
- Using evidence from studies that vary in design, sample characteristics,
and intensity of the interventions studied, researchers to date have
not found consistent gender–specific differences in the effectiveness
of intervention programs for tobacco use.
- A higher percentage of women stop smoking during pregnancy, both
spontaneously and with assistance, than at other times in their lives.
Using pregnancy–specific programs can increase smoking cessation rates,
which benefits infant health and is cost effective. Only about one–third
of women who stop smoking during pregnancy are still abstinent one year
after the delivery.
- Successful interventions have been developed to prevent smoking
among young people, but little systematic effort has been focused on
developing and evaluating prevention interventions specifically for
girls.
Disclaimer: Data and findings provided on this page reflect the content of
this particular Surgeon General's Report. More recent information may exist
elsewhere on the Smoking & Tobacco Use Web site (for example, in fact sheets,
frequently asked questions, or other materials that are reviewed on a regular
basis and updated accordingly).
Page last updated March 27, 2001