Global Collaborations
Inputs: Occupational Safety and Health Risks

This site contains documents in PDF format. You will need Adobe Acrobat Reader to access the file. If you do not have the Acrobat Reader, you may download a free copy from the
Adobe Web site.
Surveillance and Research
U.S. surveillance data are presented in detail in the NIOSH Surveillance Program Web pages.
There are no true global surveillance systems for occupational illness and injury. The International Labor Organization (ILO) collects data from member countries and periodically publishes global and regional estimates. The World Health Organization (WHO) has an ongoing effort to estimate the global burden of disease. Both organizations point out that their figures greatly under-estimate the true burden of global illness and injury due to work.
Global Fatalities
The ILO estimates that, globally, about 2.2 million people die every year from occupational injury and illness. Of this total, about 350,000 deaths are due to fatal occupational injuries1; an enormous toll of suffering for workers and their families, employers and society. In the chart below, the ILO Report provides recent estimates on work-related fatalities caused by both occupational accidents and work-related diseases.
External Link: www.ilo.org/public/english/protection/safework/wdcongrs17/intrep.pdf
(1,174 KB, 50 pages)
Global Nonfatal Injuries and Illnesses
International Labor Organization (ILO)
Estimates of global non-fatal injuries and illnesses are particularly difficult to construct. In a 2005 report, the ILO utilizes a variety of national reports to generate estimates, and states that the global workforce of 2.8 billion persons suffer some 270 million serious non-fatal injuries and 160 million work-related diseases. This takes into account non-recorded, part-time, children, and other informal sector workers.1
Pointing out that fatal accidents are just the tip of the iceberg, ILO uses an accident pyramid to illustrate that 500-2,000 less serious injuries take place for each fatality depending on the type of job.
The relationship of fatal accidents to estimates of non-fatal accidents and other measures of risk is shown in the figure below.
External Link: www.ilo.org/public/english/protection/safework/wdcongrs17/intrep.pdf
(1,174 KB, 50 pages)
World Health Organization (WHO)
WHO has an ongoing Global Burden of Disease (GBD) project that provides comprehensive, consistent, and regularly updated estimates of mortality and morbidity for more than 135 causes of disease and injury.2 In its most recent effort, WHO conducted a Comparative Risk Assessment (CRA) using global data for the year 2000 and a common methodology to estimate the contribution to the health outcomes due to exposures to 26 risk factors grouped in seven major categories of risk factors: childhood and maternal under-nutrition, other diet-related risk factors and physical inactivity, sexual and reproductive health, addictive substances, environmental risks, selected occupational risks, and other risks to health.3
The CRA used a consistent methodology throughout the project so that the impacts of these risk factors could be compared, thus improving the evidence base on distribution and costs of diseases and injuries by risk factor. The purpose was to support rational health policy decisions worldwide to develop interventions to reduce risks. All estimates were stratified by age, gender, and WHO sub-regions, thus providing regional results for the 191 Member States of WHO located in six geographical regions (Africa, Americas, Europe, Eastern Mediterranean, Southeast Asia, and Western Pacific).
The December 2005 Special Issue of the American Journal of Industrial Medicine (AJIM) volume 48, issue 6, pages 395–541 is dedicated to “The Contribution of Occupational Risk Factors to the Global Burden of Disease.”4 The methodologic requirements limited the occupational risk factors that could be studied globally so that the risks studied in individual articles account only for about 800,000 of the estimated 2.2 million deaths that occur annually due to occupational risks. Individual articles address the global burden due to occupational carcinogens, airborne particulates, noise, ergonomic risks for back pain, and risk for traumatic injury; estimating the global burden of infectious disease due to sharps injuries among healthcare workers; and examining previous published estimates of global burden due to occupational risks. Summaries of this work have also been published. 5,6
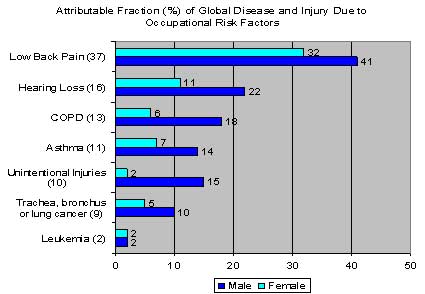
As shown in the figure below, the study concluded that occupational risk factors such as the following, contribute markedly to global illness and injury:
- 37% of back pain
- 16% of hearing loss
- 13% of Chronic Obstructive Pulmonary Disease (COPD)
- 11% of asthma
- 9% of Trachea, bronchus lung cancer
- 8% of injuries
- 2% of leukemia
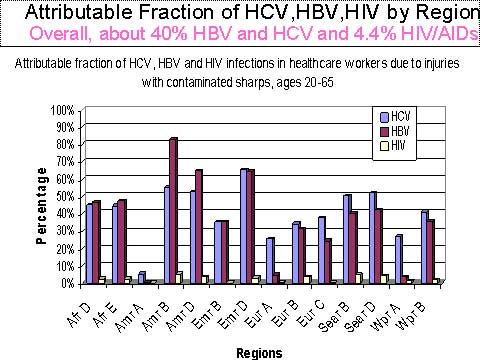
WHO also conducted a special risk analysis of Hepatitis B (HBV), Hepatitis C (HCV), and HIV infections among healthcare workers due to contaminated sharps, such as syringe needles, scalpels, and broken glass7. This analysis illustrates the general problem that high risks exist in the small worker population that has exposure. WHO found that among the 35 million healthcare workers worldwide, there were 3 million percutaneous exposures to bloodborne pathogens in 2000. This is equivalent to between 0.1 and 4.7 sharps injuries per year per healthcare worker. WHO concluded that about 40% of all HBV and HCV cases present in healthcare workers, was due to sharps injuries, with wide regional variation. WHO also found that 4.4% of HIV infections in healthcare workers globally were due to sharps injuries, with between 1% and 12% found in different regions.
Because of the lack of global data, other risk factors widespread in workplaces had to be excluded that cause reproductive disorders, dermatitis, infectious disease, coronary heart disease, intentional injuries, musculoskeletal disorders of the upper extremities, and many cancers. Psychosocial risk factors, such as workplace stress, could not be studied, nor could pesticide, heavy metal, or solvent exposures. The analysis also excluded children under 15 who work, due to the absence of adequate global data. Overall, the WHO global burden study of selected occupational risk factors provides a detailed analysis for only about 800,000 (less than 40%) of the 2.2 million deaths estimated by ILO to be due to occupational risks each year.
Next Steps
In order to assist policy makers and scientists in the countries, WHO has made available guidance for performing national and local assessments of disease and injury burden due to the selected occupational risk factors. Documents illustrating how to assess the national and local burden of disease from noise, carcinogens, and particulate exposure in the workplace are available free of charge. 7-11
External link: http://
www.who.int/quantifying_ehimpacts/publications/en/
Joint ILO/WHO Committee on Occupational Health
The importance of occupational health to both Ministers of Health and Ministers of Labor is illustrated by the long tradition of collaboration between the ILO and WHO. In fact, the Joint ILO / WHO Committee on Occupational Health was formed shortly after WHO was established; the first meeting occurred in 1950. The 13th Session of the Joint ILO / WHO Committee on Occupational Health took place in December, 2003. The Committee membership of 15 persons included representatives of employers, workers, and governments from 14 countries. The United Nations (UN) Office at Geneva, the European Commission, and 8 international non-governmental organizations were also represented. The final unanimous recommendations concerning areas of collaboration between ILO and WHO are listed below. The Committee recommended that WHO and ILO collaboration focus on the following key areas:
- Guidance and support for national occupational safety and health programs, including:
- Providing basic occupational health services
- Promoting OSH management systems and tools, including control banding
- Developing national profiles and indicators
- Assessing the cost effectiveness of OSH interventions
- Establishing effective enforcement agencies
- Enhancing regional collaboration and coordination, including:
- Developing and disseminating models for cooperation; for example, the Intensive Partnership in Africa
- Coordination and enhancement of information and educational programs and materials, including:
- Developing a joint internet-based global portal
- Statistics
- Awareness-raising activities and instruments, such as campaigns, events and special days
The Committee also recommended that special attention should be paid to the following global occupational safety and health issues in future ILO / WHO collaboration:
- Elimination of silicosis and asbestos-related diseases
- Ergonomics
- Violence at work
- List of occupational diseases
- Occupational injuries
A complete copy of the meeting report is posted on the ILO Web site. Details and background papers are also available.
External Link: http://www.ilo.org/public/english/protection/safework/health/session13/index.htm
References
- Decent work – Safe work, Introductory report to the XVIIth World Congress on Safety and Health at Work, 2005. International Labor Organization.
External Link: www.ilo.org/public/english/protection/safework/wdcongrs17/intrep.pdf
(1,174 KB, 50 pages)
- World Health Organization 2004. Global Burden of Disease Estimates.
External Link: http://www3.who.int/whosis/menu.cfm?path=evidence,burden,burden_estimates&
language=english
- Ezzati M, Lopez A, Murray C (Eds.) Comparative Quantification of Health Risks: Global and Regional Burden of Disease Attributable to Selected Major Risk Factors. Geneva: 2005 World Health Organization.
- Fingerhut M. Editor. Contribution of Occupational Risks to the Global Burden of Disease. Special Issue AJIM 48 (6) 2005: 395 – 541. This issue contains 11 articles and an editorial authored by WHO and ILO leaders in occupational health.
External link: http://www3.interscience.wiley.com/journal/112142320/issue?CRETRY=1&SRETRY=0
Note: References 5 and 6 summarize the content of the Special Issue AJIM and point out next steps to be taken.
- Fingerhut M, Driscoll T, Imel Nelson D, Concha-Barrientos M, Punnett L, Pruss-Ustin A, Steenland K, Leigh J, Corvalan C. Contribution of occupational risk factors to the global burden of disease – a summary of findings. SJWEH Suppl 2005 (1): 58-61
External link: http://www.sjweh.fi/show_abstract.php?abstract_id=939
- Fingerhut M, Nelson D, Driscoll T, Concha-Barrientos M, Steenland K, Punnett L, Prüss-Üstün A, Leigh J, Corvalan C, Eijkemans G, Takala J. The Contribution of Occupational Risks to the Global Burden of Disease: Summary and Next Steps. La Medicina del Lavoro In 97(2):313-323 (2006).
- Pruss-Ustun A, Rapiti E, Hutin Y. 2005. Estimation of the global burden of desease attributable to contaminated sharps injuries among health-care workers. Am J Ind Med. 48 (6): 482-49.
- Concha-Barrientos M, Cambell-Lendrum M, Steenland K. Occupational noise: Assessing the burden of disease from work-related hearing impairment at national and local levels. Geneva: World Health Organization 2004 (Environmental burden of disease series No. 9).
- Driscoll T, Steenland K, Pruss-Ustun A, Nelson D, Leigh J. Occupational carcinogens: Assessing the environmental burden of disease at national and local levels. Geneva: World Health Organization 2004 (Environmental burden of disease series No. 6).
- Driscoll T, Steenland K, Nelson D, Leigh J. Occupational airborne particulates: Assessing the environmental burden of disease at national and local levels. Geneva: WHO 2004 (Environmental burden of disease series No. 7).
- Rapiti E, Pruss-Ustun A, Hutin Y. Sharps injuries: Assessing the burden of disease from sharps injuries to health-care workers at national and local levels. Geneva: World Health Organization 2004 (Environmental burden of disease series No. 11).